
Abstract
BACKGROUND:
Asymmetry and scar formation of the nipple-areola complex (NAC) after reduction mammoplasty with periareolar suture are common complications and can significantly affect patient satisfaction.
OBJECTIVE:
The aim of this study was to investigate possible procedure-specific influencing factors on asymmetry and shape disturbances of the nipple-areola complex to optimize postoperative outcome and thus improve patient satisfaction.
METHODS:
78 patients were followed-up after a 5-year period as part of a retrospective cohort study. Objective parameters as areolar diameter, symmetry, scar patterns, dimensions of the breast, and anthropometric measurements were recorded. All patients underwent surgery according to an established treatment algorithm depending on the preoperative measurements. Follow up was 1 week, 6 week, 6 months and 3 years postoperatively.
RESULTS:
The periareolar suture-technique significantly influenced the symmetry and shape of the NAC. Compared to the intraoperative determined diameter and the postoperative diameter, the net-suture technique showed the highest NAC symmetry and minimal divergence. Patients who underwent Hall-Findlay mammoplasty showed significantly higher rates of asymmetry and deformity of the NAC with teardrop formation in comparison to Lejour mammoplasty. Scar formation was affected by periareolar ruffle formation especially after purse string suture.
CONCLUSIONS:
Regardless of what reduction mammoplasty techniques and periareolar suturing-technique are used, a tension-free suture of the NAC is crucial for shape, symmetry and scar formation. The net suture technique resulted in significantly higher symmetry of the NAC.
Keywords
Background
Bilateral reduction mammoplasty, a common surgical procedure worldwide, is primarily indicated for women experiencing physical discomfort or psychological distress due to macromastia. The procedure not only reduces breast size but also improves breast shape and symmetry, significantly enhancing the patient’s quality of life [1]. Nipple-areolar complex creation is the last step in mammoplasty surgery and plays a significant role in patients’ overall satisfaction. However, achieving optimal postoperative outcomes, particularly concerning the nipple-areola complex (NAC), remains a challenge. The NAC’s shape, size, symmetry, and scarring significantly influence the aesthetic outcome and patient satisfaction post-surgery. We could demonstrate this finding in a previous study concerning congenital breast asymmetry by Noisser et al. [2]
Despite the high prevalence of reduction mammoplasty, with over 500 000 procedures [3] performed in 2021, complications related to the NAC, such as distortion, asymmetry and scarring, are common. Therefore, understanding the factors influencing the NAC’s postoperative appearance is crucial for surgeons to optimize surgical techniques and patient counseling.
This paper aims to explore the various factors influencing the shape, size, symmetry, and scar formation of the NAC following bilateral reduction mammoplasty. By doing so, we hope to provide a comprehensive guide for surgeons to enhance postoperative outcomes and patient satisfaction.
Methods
Study design
In a retrospective cohort study, 78 patients were followed up over a period of 5 years postoperatively. Breast reduction surgery was performed in accordance with an established surgery algorithm in 2020 at the Department of Plastic, Aesthetic, Hand and Reconstructive Surgery of the University hospital Regensburg. Different suture techniques of the NAC were performed after an in-house surgical protocol. Data collection was approved by the ethics committee of the University Hospital Regensburg (20-1654-101). To objectify postoperative outcomes, patients underwent standardized follow-up examinations preoperatively, at one week, six weeks, six months, and three years postoperatively.
During these follow-up examinations clinical data such as complications and anthropometric data of the breast were collected. Further a digital three-dimensional image of the breast was taken and the patients’ quality of life was examined using a validated questionnaire (Breast-Q™).
Participants
A total of 78 female patients who underwent breast reduction surgery were included in this study. The mean preoperative weight of the participants was 73.5 kg, with a mean age of 47 years and a mean BMI of 26.7. The mean preoperative weight of the breast was 948,63 g. The relevant metadata of the patient collective are listed in Table 1.
Anthropomorphic data of the patient collective
Anthropomorphic data of the patient collective
Breast reduction surgery was performed using the Hall-Findlay, U-scar (horizontal reduction technique), and Lejour technique. These techniques were chosen based on standardized in-house surgical protocols based on patient-specific factors and anthropomorphic data. The NAC diameter was determined intraoperatively with a freeman areola marker ranging from 36–42 mm. Periareolar suture of the NAC was performed using the following techniques (Fig. 1):
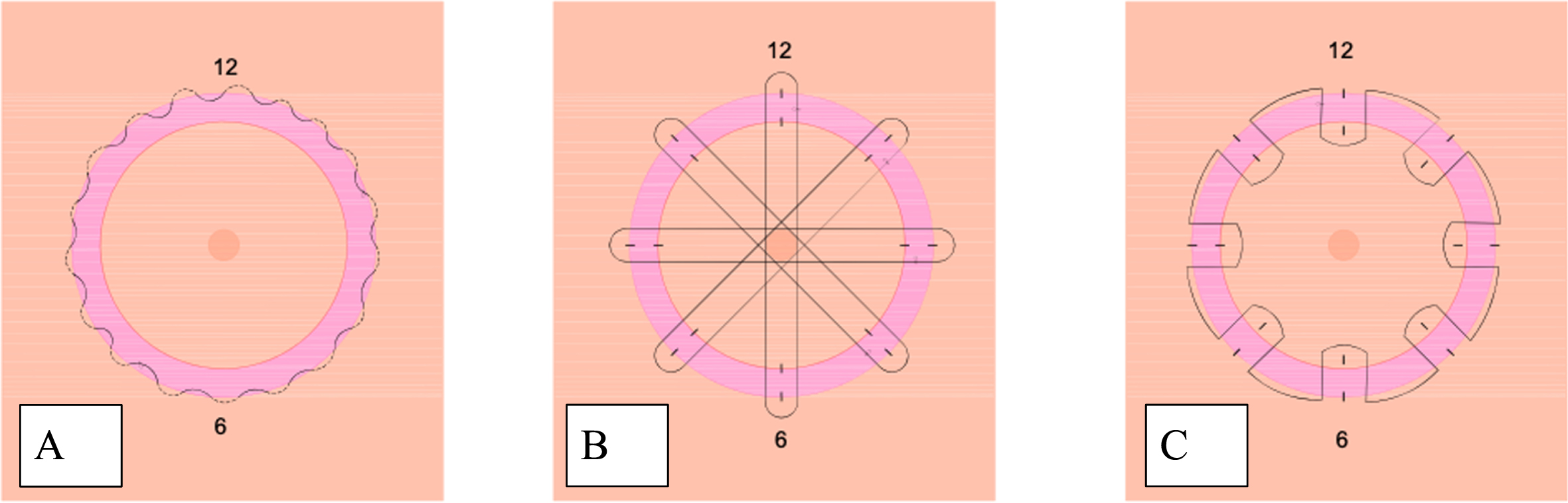
Periareolar suture techniques: A: purse-string suture, B: net-suture, C: wheel suture.
In the purse string suture (Fig. 1A.), as in a purse string, the periareolar skin is gathered by a continuous subcutaneous suture using PDS 4-0, thus reducing the diameter of the opening. In the reduced NAC opening, the NAC is then sutured to the periareolar skin using a continuous intracutaneous suture with Monocryl 4-0. Fine corrections can be made with Seralon 5-0 [4, 5].
Net-suture
The net-suture technique allows deep dermal support of the areola. This can especially prevent prolapsing of the NAC (Fig. 1B.). The suture is made with a straight needle and a PDS 3-0 thread. A total of 4 sutures are made, starting on one side in the area of the periareolar skin, passing through the areola to the opposite side, where the suture is passed again into the wound margin of the periareolar skin and back through the areola to the initial side of the suture. While passing the suture from one side to the other, the skin of the areolar is penetrated subdermal. However, the skin under the nipple needs to be left out to prevent nipple inversion. The sutures are knotted after setting the desired areolar diameter. Subsequently, the periareolar skin and the NAC are sutured in a continuous intracutaneous suture technique using Monocryl 3-0. Fine corrections are made using Seralon 5-0.
Wheel suture
The wheel suture is particularly suitable for periareolar wound closures with a large circumferential difference between the periareolar skin and the NAC. The redundancy of the diameter requires a precise suture technique to achieve the most even distribution of the periareolar skin excess. In the wheel suture (Fig. 1C.), the NAC and periareolar skin are marked at 12-,3-,6-, and 9- o’clock. Then, a deep-dermal, continuous suture is made using PDS 3-0 as follows: The suture begins deep dermally as a horizontal mattress suture approximately 0.4 cm from the wound edge of the periareolar skin from the first to the next mark. The suture is then continued in the area of the NAC. Here, a now shorter section is also stitched deep dermally in the sense of a horizontal mattress suture. The suture is continued in the same manner around the whole areola. Due to the difference in suture length in the area of the NAC and the periareolar skin, the excess periareolar skin is evenly distributed over the smaller circumference of the NAC. By pulling on both ends of the suture, the diameter of the NAC can be determined. This is followed by an intracutaneous continuous suture using Monocryl 3-0 and, if necessary, fine corrections using Seralon 5-0 [6].
Examination
Patients were examined after a standardized postoperative protocol, preoperatively, 1 week, 6 weeks, 6 months, and 2 years postoperatively. Anthropometric measurements, such as weight and BMI, were recorded. Additionally, breast measurements were obtained using the Vectra H2 camera system, which provides accurate and detailed 3d model of the breast. These 3d-models were evaluated for breast volume, shape, and symmetry [7]. Further were the following objective parameters evaluated: symmetry of the breast, symmetry of the areolae and volume difference of both breasts. For this purpose, patients were measured with a tape measure on the skin surface. Postoperative breast volume was calculated using the Breast-V formula proposed by Longo et al. [8] for ptotic breasts and extended by Huang et al. [9] for non-ptotic breasts. Both formulas have been used in several studies [10–13].
Statistical analysis
SPSS® Statistics version 25.0.0. (IBM®, Armonk; New York) was used for statistical analysis. Because our data did not follow a normal distribution in either group or in any of the cases (Kolmogorov-Smirnov test and Shapiro-Wilk test), the Mann-Whitney test was applied to detect differences between groups. P values < 0.05 were considered statistically significant.
Results
Measuring the change of intraoperatively determined NAC diameter and the postoperative measured NAC diameter in comparison to the three different types of NAC suture techniques showed that the net-suture lead to the smallest NAC diameter divergence postoperatively of 4.22 mm (±3.11). The purse string pouch suture technique led to a mean NAC diameter divergence of 5.35 mm (±6.65) and the wheel suture technique showed a mean NAC diameter divergence in comparison to the intraoperatively determined diameter of 8.52 mm (±3.50). Therefore, the postoperative measured NAC-diameter, sutured with the net-suture, was closest to the intraoperatively determined NAC-diameter. The net-suture is consequently the most reliable method to keep the postoperative result as constant as possible. Comparing all three suture techniques with each other, the net suture technique showed significant less diameter divergence in comparison to the wheel and purse-string suture Fig. 2.
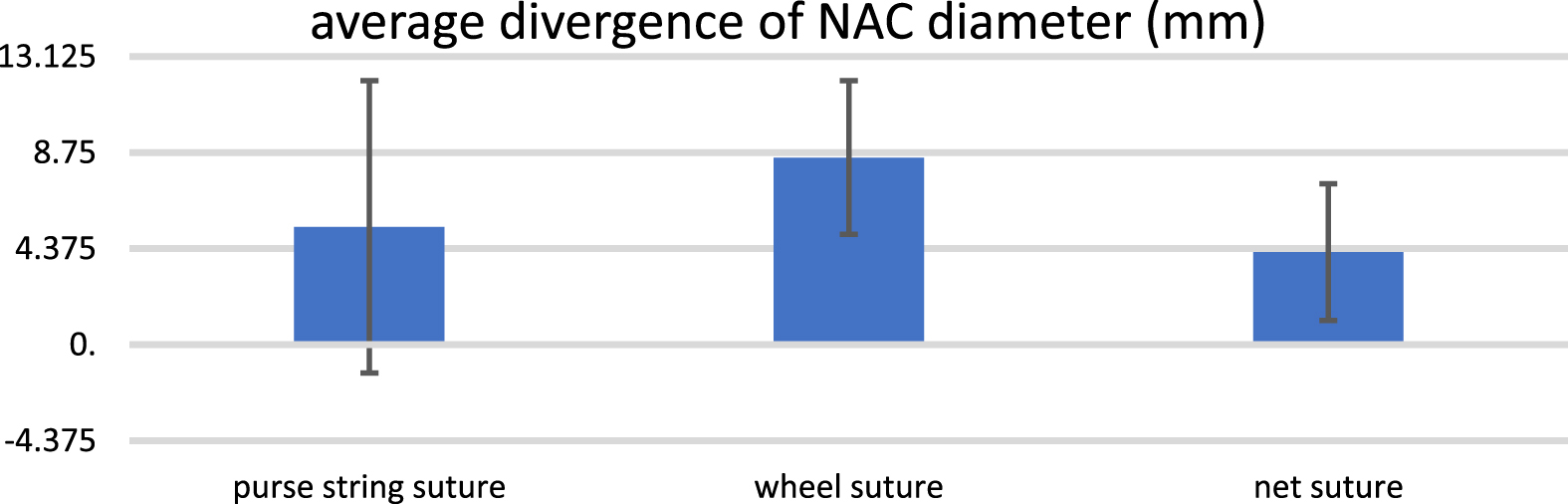
Average divergence of NAC diameter in mm comparing the intraoperatively determined NAC diameter with the postoperative diameter in (mm).
Correlating the NAC diameter divergence postoperatively in comparison to the different reduction mammoplasty techniques showed the following results (Fig. 3):
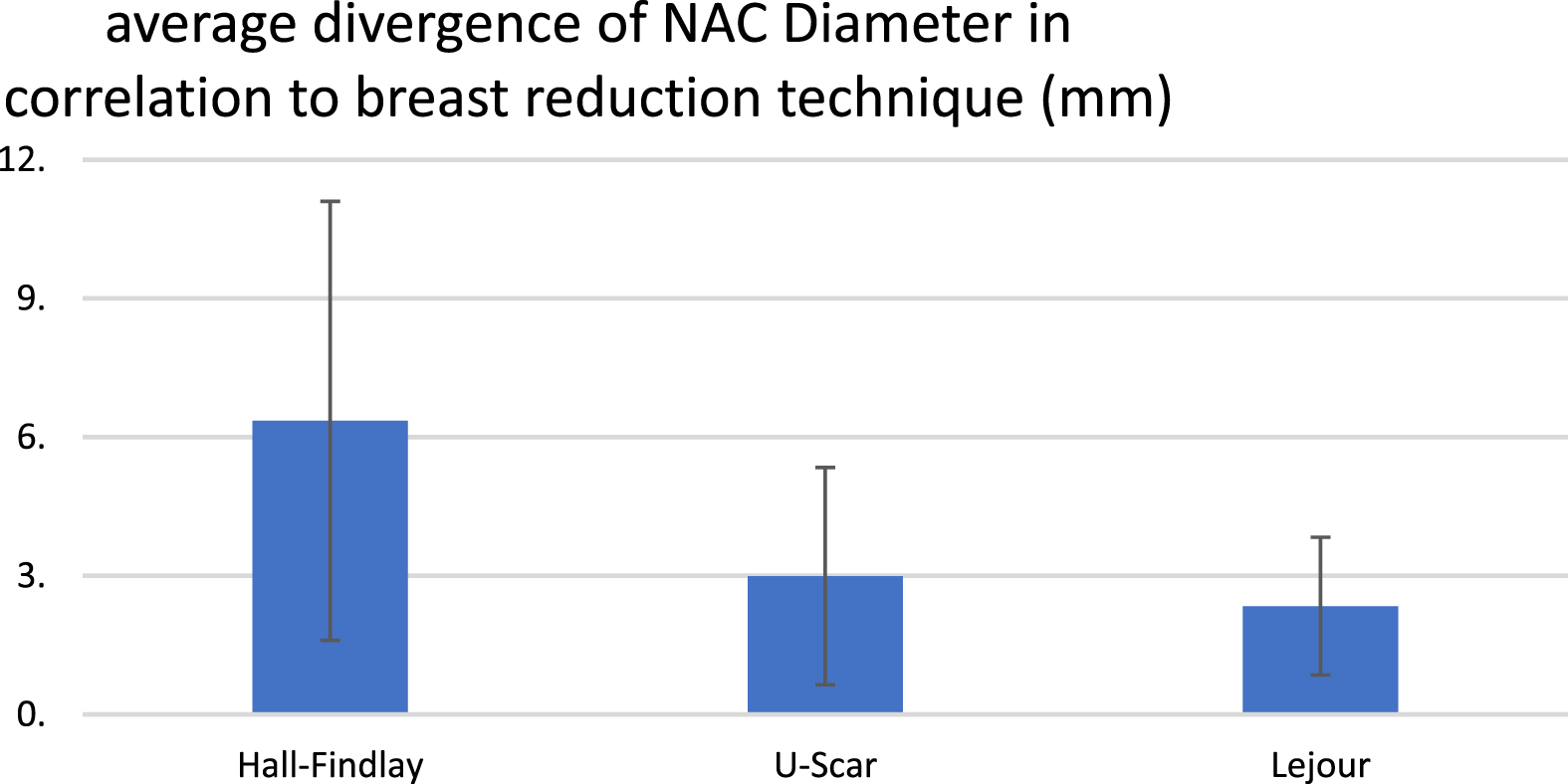
Average divergence of NAC diameter (intra vs. postoperative) in mm comparing the three different mamma reduction techniques: Hall-Findlay, U-Scar, Lejour.
Breast reduction after Lejour technique led to the smallest divergence of the intraoperative determined NAC diameter in the postoperative follow up examinations. The average NAC deviation (intraoperative vs. postoperative) with Lejour technique was 2.34 mm (±1.40). U-Scar technique mamma reduction showed an average deviation of the intraoperative NAC diameter in comparison to the postoperative NAC diameter of 2.99 mm (±2.35). The highest deviation of the intraoperative and postoperative NAC diameter was seen using Hall Findlay mamma reduction technique with average deviation of 6.35 mm (±4.74).
Comparing the postoperative breast weight measured with Breast-V formula proposed by Longo et al. [8] and the postoperative NAC symmetry revealed the following results (Fig. 4). There was no significant correlation found between breast weight and NAC symmetry. The patient group with a postoperative breast weight between 300 g and 350 g showed a postoperative NAC divergence in comparison to the intraoperative determined NAC diameter of 6.31±13.22. Patient group with breast weight between 351–400 g showed a mean NAC diameter divergence of 5.88 mm (±14). Group between breast weight of 401 –450 g showed a mean divergence between intra- and postoperative NAC diameter of 6.6 mm±12.66. Patient group with breast weight of 451 –500 g showed a mean NAC diameter divergence of 2.88±8.91. The group with the highest breast volume postoperative ranging from 501–550 g showed a mean divergence of NAC diameter of 4.63±18.35.
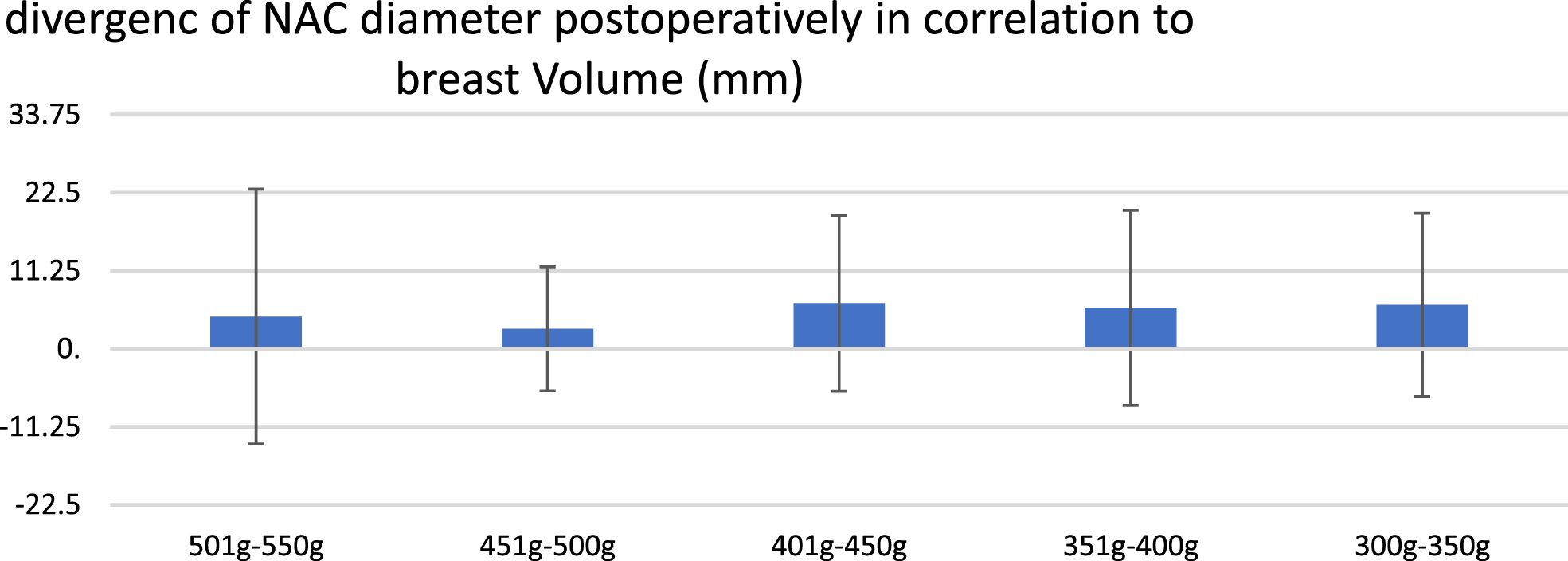
Postoperative NAC diameter divergence(mm) in comparison to postoperative breast weight (g) using Breast-V formula proposed by Longo et al. [8].
No instance of wound healing disorders were observed among any of the patients subjected to the three different suture techniques.
NAC creation is a critical step in breast reduction. The study’s primary finding demonstrates that the most important factor influencing the NAC size, symmetry and postoperative diameter in correlation to intraoperative diameter is the correct periareolar suturing technique. The net-suture technique which provides an extensive support of the NAC showed the smallest divergence of intra- and postoperative NAC diameter. This finding is consistent with our hypothesis and the existing literature. This novel suture technique with its “fishing-net” appearance, provides a wide distributed support of the NAC. The used monofilament polydioxanone suture retains its strength over a longer period of time. As described by Ray et al. [14] the PDS suture holds its strength over a period of 4 weeks up to 58% in comparison to other monofilament resorbable suture. As a result, the suture of the NAC is free of tension for a longer period of time and can thus contribute to better wound healing. The purse-string suture technique and wheel suture technique, both techniques who don’t pass the NAC from one side to the other and only suture on the outer borders of the periareolar and NAC skin seem to give less support to the NAC in the process of wound healing and therefore lead to greater changes in postoperative NAC diameter in comparison to the intraoperative determined diameter.
In addition, our study showed that the surgical technique of breast reduction is significantly related to the postoperative NAC shape. Hall-Findlay technique, where the NAC is transpositioned with a superiomedial pedicle led to biggest divergence of intraoperative determined NAC diameter and the postoperative NAC diameter. This might be affected by the multidirectional vectors of tension due to rotation of the pedicle in a cranial motion [15]. The vector of scar tension differs between the Hall-Findlay and Lejour technique fundamentally. The Lejour technique which is a vertical mastopexy with cranial pedicle/ monobloc mastopexy has therefore only one vertical vector of tension of the subcutaneous and breast-gland tissue [16]. Consequently, tension on NAC scar is less in comparison to Hall-Findlay mammoplasty. The effect of tension on scar formation and symmetrical changes has already been described by Meyers et al. [17].
Considering the postoperative breast volume, which was examined using the Breast-V after Longo et al. [8], there was no correlation between symmetry of the NAC and the breast volume.
There was no clinical evidence of postoperative microcirculation disorders with any suture technique. In addition, there was no intraoperative microcirculatory disturbance as described by Veith et al. [18].
Conclusion
Regardless of the reduction mammoplasty techniques and periareolar suturing-technique, a tension-free suture of the NAC is crucial for the shape, symmetry and scar formation of the NAC. The net suture technique resulted in significantly higher symmetry of the NAC in comparison to the commonly used pearl-string and wheel suture technique. A tension free suture in all surgical techniques is crucial to counteract postoperative deformation of the NAC. Vectors of tension do influence scar formation and consequently symmetry of the NAC and should always be considered while planning wound closure and selecting wound suture.
Footnotes
Acknowledgments
We sincerely thank all patients who participated in this study.
Conflict of interest
There are no conflicts of interest.
Authors contributions
Brebant, Prantl, Diesch contributed to the conception of the study; Eigenberger, Anders, Griesbeck contributed to data collection; Diesch, Anders, Wiesmeier, Griesbeck, Brebant, Brix contributed to data analysis and interpretation; Diesch, Brebant, Prantl drafted the manuscript; and Wiesmeier, Anders, Brix, Griesbeck, Eigenberger revised the manuscript. All authors read and approved the final manuscript.