
Abstract
CONTEXT:
Global sales of compression garments have risen sharply in recent years. Due to the availability of a wide range of compression garments, this study aims to evaluate the effect of two types of compression garments and kinesio tape on edema formation and tissue perfusion in the lower extremities. Over-the-counter compression knee stockings and kinesio tape were compared with a prototype of high-end compression stockings that combine kinesio tape and a common knee bandage. The high-end compression stockings were designed by Cube with the aim of combining the positive effects of kinesio tape and compression garments on edema formation and tissue perfusion.
DESIGN:
Clinical cross-over study.
METHODS:
Before and after a 6-hour compression period, the knee regions on both, the treated and non-treated leg, of participants were examined using a 3-D scan to detect changes in volume. Also measured were local temperature (°C), oxygen saturation (SpO2), perfusion index (Pi), blood pressure (mmHg), compression pressure (mmHg), range of motion, body-mass-index (BMI) and limb-circumference (cm). Two different types of compression garments were examined: a novel high-end compression stocking (A) and a common compression stocking (B). In addition, kinesio tape was compared to compression garments (C). After each experimental day, a one-day break was taken to prevent an unwanted overlay effect. Male and female participants between the ages of 18 and 60 were randomly selected.
RESULTS:
The high-end compression garment (A) showed a statistically significant (P = 0.009) reduction of edema intraindividually. Comparing the three treatment groups, compression (A) lead to a reduction of edema. However, the reduction was not statistically significant (P = 0.585). The compression garment B and kinesio tape showed an increase in edema in the lower limb. There was a positive correlation between the highest compression pressure (A: 9.8 mmHg) and volume decrease over the period of 6 hours. Lighter compression (B: 8.2 mmHg) led to an increase in leg volume after compression application over 6 hours. There was no significant difference in tissue oxygen saturation with the two types of compression and kinesio tape. The tissue temperature below the compression garment was highest in the compression group A. Nevertheless, we could not demonstrate a statistically significant correlation between tissue temperature and volume difference.
The range in motion of the lower limb decreased after 6 hours with both compression A and B and with kinesio tape.
CONCLUSION:
The novel bandage showed a statistically significant reduction in edema when compared intraindividually, but no statistically significant advantage was found when compared with the other compression garment B and kinesio tape.
Despite the widespread use of kinesio tape, we did not find any improvement in the range of motion, edema prevention and circulation in the lower limb after application of kinesio tape.
Keywords
Introduction
The global compression and shapewear market had an estimated value of over 2.82 billion USD in 2021 [1]. The predicted compound annual growth rate is over 5%. Despite the enormous demand, few studies have scientifically examined the effectiveness of different types of compression materials and kinesio tape. In our study, two types of compression garments were examined for their effect on tissue perfusion, range of motion, and edema prevention in the lower limbs. Compression garments are a commonly used method to prevent edema and have greatly increased in popularity in professional and semi-professional sports. Furthermore, compression is used in the prevention of edema and in patients with venous insufficiency as well as lymph- or lipedema [2]. Other studies have shown that patients with occupational leg edema benefit from compression stockings worn on the lower limbs [3]. The compression garments examined in this study differed in the materials used, and therefore in the compression class. In addition, kinesio tape was evaluated based on the same parameters. There is only limited evidence showing the benefits of kinesio taping in reducing edema. Nevertheless, kinesio tape is popular among physiotherapists, chiropractors, and athletic trainers, and is furthermore used in preventing edema, treating cancer-related edema, preventing injuries, and improving performance [4, 5]. Studies in rats suggest that kinesio taping can lead to an increase in epidermal-dermal distance, resulting in increased lymph flow [6, 7]. Furthermore, kinesio tape is said to improve pain management and musculoskeletal rehabilitation [8, 9].
In our study, a classic compression garment was compared to a prototype high-end compression stocking that is a hybrid of compression garment and kinesio tape. The hypothesis of this study was that changes in local microcirculation due to compression and/or kinesio taping might reduce edema formation and therefore improve the range of motion in the lower limb. In addition, a possible correlation between compression pressure and edema reduction was examined.
Material and methods
This randomized prospective clinical cross-sectional study was approved by the University of Regensburg institutional review board (20-2088-101). This study is registered as a clinical trial under the following registration number: DRKS00024991.
35 randomly selected male and female participants between the ages of 18 and 60 (mean 34.6 years) were included. An additional inclusion criterion was a body mass index (BMI) between 18.5-24.9 (kg/m2). Exclusion criteria were: epilepsy, increased light sensitivity, pre-existing lymphatic conditions, and prior surgery on the lower extremity. The participants provided informed consent in accordance with the Helsinki Declaration. Two different types of compression garments were examined in the knee regions of participants: a novel high-end compression garment, designed by the company Cube and produced by the company Enchess, which combines compression material and kinesio tape (A), and a standard, over-the-counter compression garment (B) as well as kinesio tape (C). The sequence of the application of the different types of compression was randomized by constrained block randomization. The process of allocation was concealed. However, once the sequence number was revealed, the principal investigator (GB) became aware of the group allocation and subsequently assumed the roles of therapist, data collector, and analyst. All participants were naive to the hypothesis of the study.
The duration of compression was six hours (t = 0: before application, t = 6: after 6 hours of application). Participants pursued their daily jobs/work while wearing the garments and kinesio tape. The examination was every other day to prevent overlay effects. The compression garment was always applied to the right leg. The left leg was not subject to treatment and thus served as a interindividual control group.
Compression garment sizes ranging from XS-XL were determined by standardized EU sizing charts used in retail. The kinesio tape used was standard over-the-counter kinesio tape by Leukotape K, BSNmedical GmbH Leukotape®. The tape was applied in standing position in accordance with standard protocol.
The following parameters were evaluated on both the treated and untreated leg before and after each period of treatment: The volume of both legs was measured using 3D-volumetry obtained by a handheld 3-D camera (Artec EVA, Artec, Luxembourg). The legs were measured in a lunge-step position with a defined stride length of 50 cm. The image was visualised with software (Artec Studio 14, company Artec, Luxembourg), and a laptop was connected to the camera. The result was a three-dimensional coloured image of the scanned body part. Markings were drawn on anatomically prominent parts of the legs’ bone structure such as the malleolus medialis and lateralis. In addition, the range of motion of the knee joint was assessed using the neutral zero method. Also measured were tissue perfusion (SpO2), perfusion index (Pi), skin temperature (°C), compression pressure (mmHG), heart rate, and blood pressure (mmHg).
Perfusion index, SpO2, compression pressure, and temperature were measured on the ventral thigh as well as the dorsal and medioventral lower leg. The pressure of the compression garment applied to the leg was measured using a pressure probe (Fraunhofer Institute, Würzburg, Germany), which was applied under the compression garment. The measurement was carried out using a measuring device (PeakTech 3335 DMM) from PeakTech GmbH. The measured values were recorded in nanoferrates (nF) and later translated into mmHg using a calibration curve. The Perfusion index, temperature, and tissue SpO2 were measured using a Masimo Rad-97 Pulse CO-Oximeter (Masimo, USA). The blood pressure and peripheral SpO2 saturation were measured with an IntelliVue X3, MX450 (Philips, Germany). The body fat percentage was quantified with standardised body fat measuring forceps. Body circumference was measured using a measuring tape. To calculate the BMI, we used the Durin-Womersley Caliper formula. All the collected data were entered manually into a SPSS file.
Subsequently, the statistical analysis was carried out with the programme IBM® SPSS® Statistics (version 25, 64-bit version). First, descriptive parameters such as mean, maximum, minimum, and percentiles were determined. The effect of treatment was determined by means of suitably exact tests. The Spearman-Rho test was used to evaluate the effect of compression pressure on the volume of the leg, the influence of the BMI on the leg volume, and the possible effect of different temperatures on the leg volume. The Wilcoxon test was used to investigate the mobility of the knee joint, temperature differences, and oxygen saturation.
Results
Comparing the change of the relative volume in liter (t6 - t0) of the right leg (intervention) with the left leg (control-group), showed that use of compression garment A resulted in a statistically significant (p = 0.009) decrease in volume –0.5 l (±2.8%) in comparison to the control group (left leg) +0.7 l (±2.8%) (Wilcoxon Test). Compression garment (B) and the kinesio tape (C) both showed a statistically significant increase in relative volume in liter (t6 - t0) in comparison to the control leg (B: t0 = 7.249 l±1.080, t6 = 7.308±1.153; p = 0.022) (C: t0 = 7.334±1.191, t6 = 7.428±1.247; p = 0.002).
Therefore, compression garment A was the only compression that led to a statistically significant decrease in volume compared intraindividually.
Average means in % change in volume from time t0 to time t6 with results of Wilcoxon tests of control and intervention group (A, B, C)
Average means in % change in volume from time t0 to time t6 with results of Wilcoxon tests of control and intervention group (A, B, C)
However, comparing compression garment A, B and kinesio tape with each other, there was no statistically significant edema reduction p = 0.585 (t0 = 7.407 (±1.137), t6 = 7.364l (±1.138)). Gender distribution was 77.1% male and 22.9% female.
Figure 1 shows the boxplots of the volume difference (in %). Compression A showed significantly different changes in volume in comparison to B, C, and the control-group (A-B: p = 0.017, A-C: p = 0.026, A-control: p < 0.001). Statistically significant gender differences in volume difference (in %) could not be detected (Mann-Whitney-U test). No statistically significant correlation between the volume difference (in %) and the BMI, age, or body fat percentage could be determined (rank correlation according to Spearman).
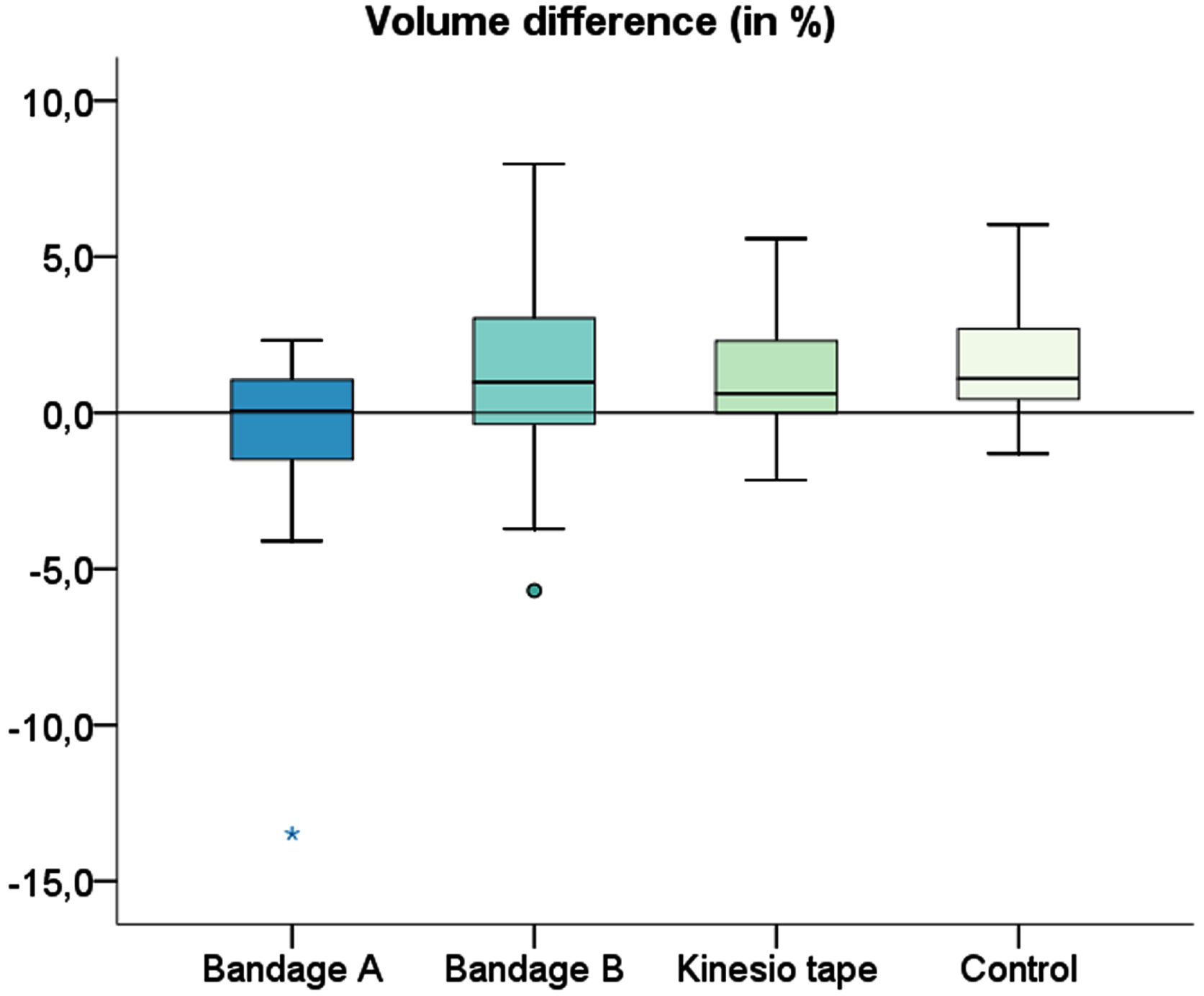
Boxplots of the volume difference (in %) for different interventions (A = high-end compression garment with kinesio tape within the garment; B = standard knee compression garment; C = kinesio taping) and the control measurement.
When looking at the mean pressure (mmHg), the mean value of the measured points (musculus quadriceps femoris, musculus triceps surae, and tibial tuberosity) showed no statistically significant difference between compressions A and B (P = 0.080). On average, compression A had a pressure of 9.8mmHg and B a pressure of 8.2mmHg.
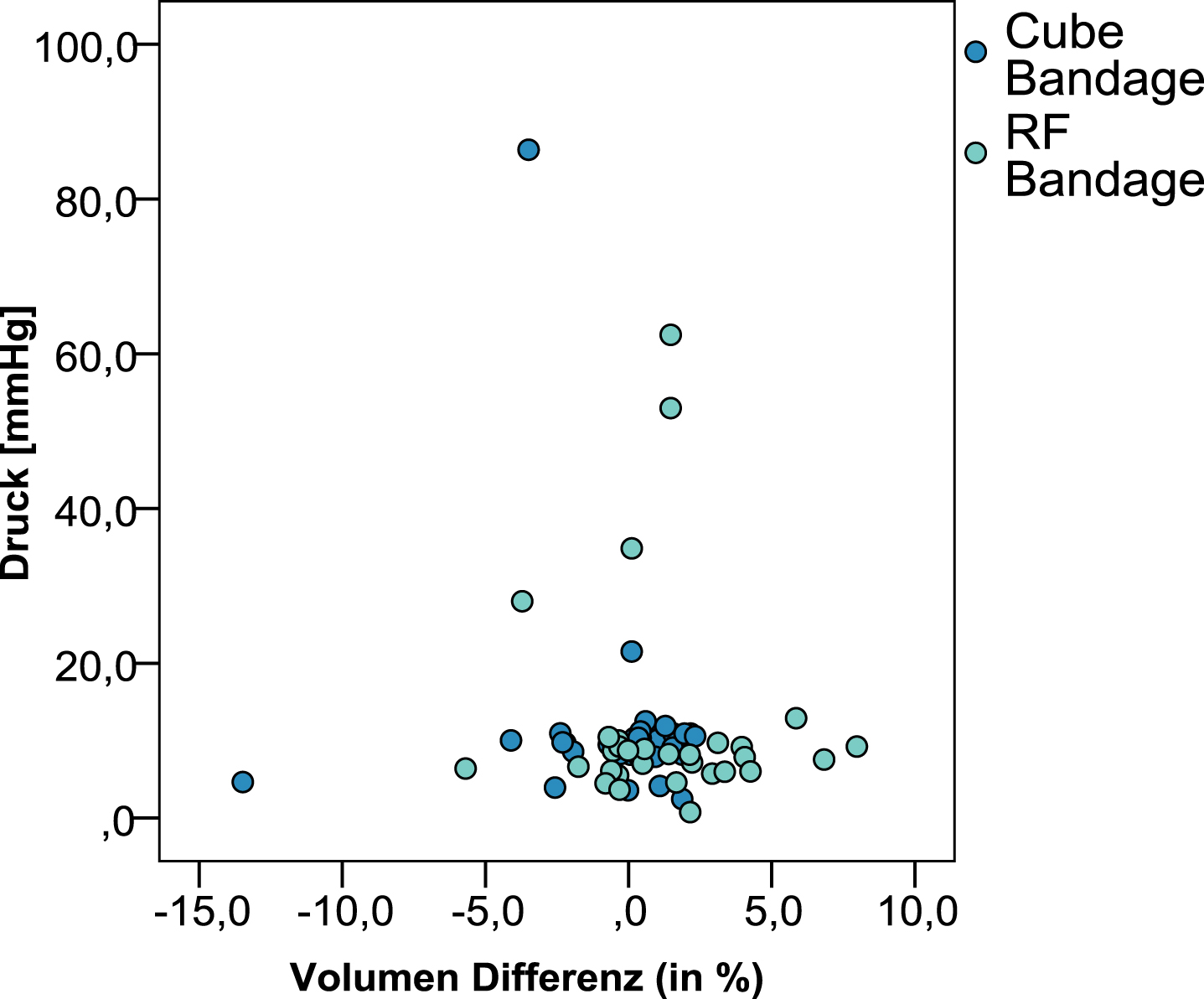
Scatter plot showing the relationship between volume difference (in %) and pressure [mmHg] for compression A and B.
Table 2 shows the change in oxygen saturation on the triceps surae muscle from time t0 to time t6 for the compression A, B, and C. There is a slight decrease in average oxygen saturation over the 6 hours of intervention. However, the decrease in oxygen saturation is not statistically significant. Measured points at musculus quadriceps femoris and tuberositas tibiae showed no significant changes in oxygen saturation over the duration of the examination (t0-t6).
Comparison of oxygen saturation at the triceps surae muscle at t0 and t6 of compression A, B, C, and results of the Wilcoxon test
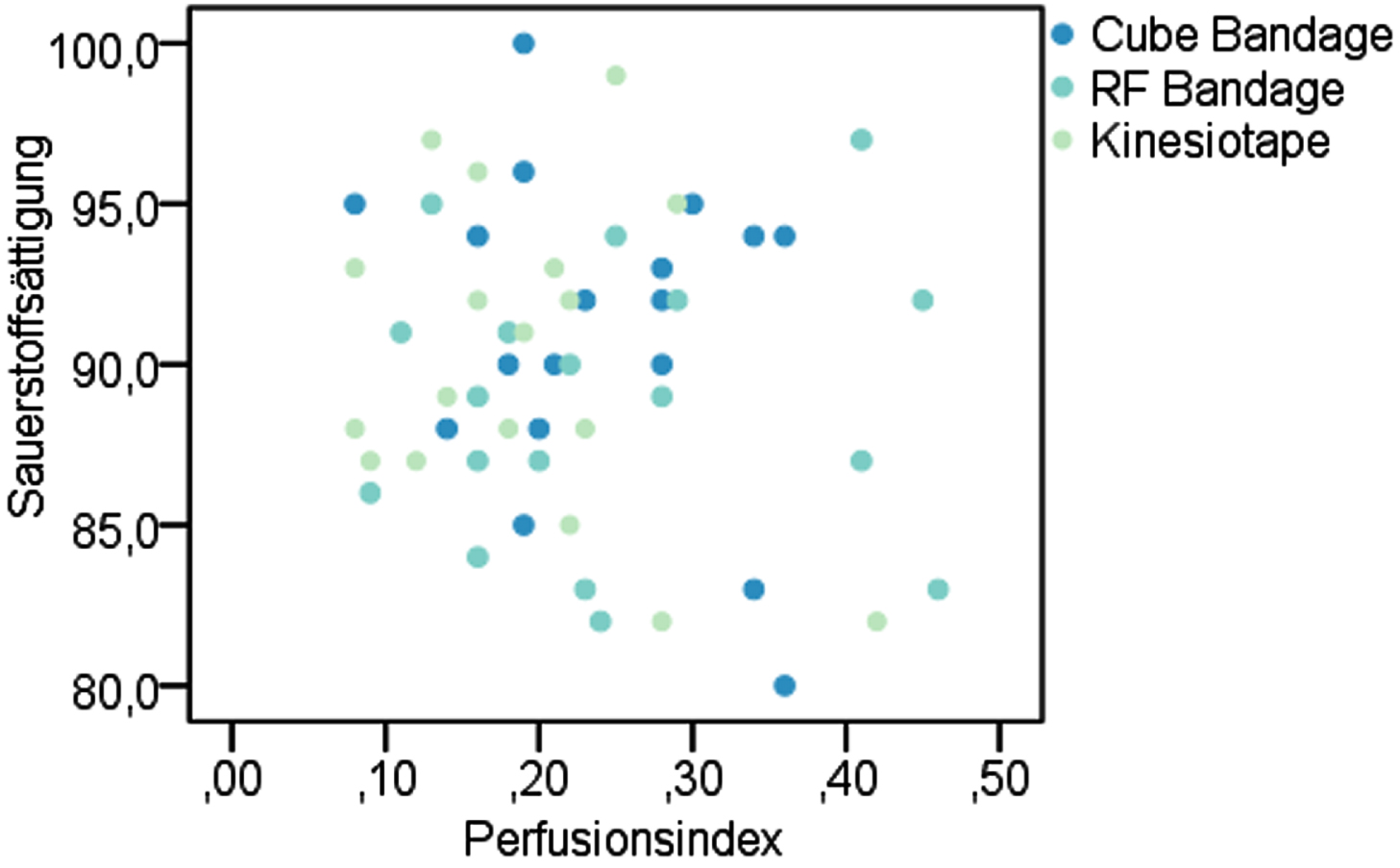
Scatter plots to show the correlation of oxygen saturation with perfusion index at the muculus triceps surae at t6 after intervention.
A statistically significant difference in oxygen saturation between A and B, as well as B and C at time t6 on the triceps surae muscle could not be detected. Compression A showed a statistically significant difference in oxygen saturation with an average of 91.9 (±3.6) % compared to C with 89.6 (±5.6) % (p = 0.020) Wilcoxon-Test. The perfusion index changed at the location of the triceps surae muscle between t0 and t6. For B (t0 0.21 (±0.12); t6 0.23 (±0.12) p = 0.286) and C (t0 0.2 (±0.1); t6 0.25 (±0.09) p = 0.081) there was a slight mean increase in the perfusion index over the 6 hours of intervention, while A (t0 0.23 (±0.16); t6 0.23 (±0.16) P = 0.731) remained at the same level. There were no statistically significant differences. The measurements of the tuberositas tibiae showed no significant changes.
No statistically significant correlation could be shown between oxygen saturation and perfusion index. Correlation coefficient between perfusion index and oxygen saturation at the measured location over the mucusulus triceps surae was: Compression A: –0.126, p = 0.549, B: –0.129 p = 0.529.
A comparison of the temperatures measured at the different measurement sites showed a statistically significant difference at the triceps surae muscle between A and B (p = 0.026). The mean temperature at this point under compression A was 29.5°C (±1) and compression B 28.8°C (±1).
No statistically significant temperature differences were detectable at the quadriceps femoris and tibial tuberosity. No statistical correlation could be shown between volume difference and temperature (rank correlation (Spearman)).
The range of motion of the knee joint was slightly reduced in the intervention group (right leg) compared to the control group (left leg) in all groups A, B and, C (p = 0.671).
The study’s primary finding demonstrates that application of higher level of compression (A) on the lower limb leads to a significant decrease in edema formation in the lower limb, which is consistent with our hypothesis and the existing literature. Similar findings were made by Sugahara et al. [10]. Belczak et al. [11] also found that compression on the lower limb with 20–30 mmHg reduced edema formation significantly in comparison with compression between 15–20 mmHg. This is also consistent with our findings. Mosti et al. [12] showed that compression with a strong inelastic bandage in comparison to an elastic stocking made only a small difference in edema reduction. Similar findings were made by Partsch et al. [13]. He was able to show that there was an upper limit beyond which a further increase in applied compression pressure was counterproductive. The maximum effective limit of pressure for the lower leg was suggested to be around 50–60 mmHg [13]. This apparent threshold of applied pressure, above which compression becomes counterproductive and tends to contribute to edema formation, could not be shown in our study. One reason for this could be that the compression garments used exerted much less pressure on the lower extremity than in the above-mentioned studies.
In contrast to the novel high-end compression garments A, the application of standard compression garment (B) and kinesio tape (C) resulted in an increase in edema formation. In addition, the use of kinesio tape even led to an increase in edema compared to the untreated control group. Boguszewski et al. [14] came to different results in their study. They evaluated the effectiveness of kinesiology taping as an aid to rehabilitation following knee trauma and observed a faster reduction of edema and therefore improvement in the range of motion in patients treated with kinesio tape. A possible reason for the contrary findings may be that injured subjects (knee trauma) were included in the study by Boguszewski et al. [14], as opposed to the healthy subjects in our study. It must be assumed that traumatised tissue has a different tendency to develop swelling and edema compared to non-traumatised tissue.
Szczesny et al. [15] have shown that local inflammatory reaction at the site of injury leads to cytokine signalling to the regional lymph nodes, which leads to changes in the lymphatic system of the lower limb. We could not detect any change in microcirculation, and thus in perfusion of the tissue, either in correlation with compression pressure or within the two types of compression garments examined. Similar findings have been made by Banjeree et al [16]. He showed that kinesio tape does lead to a decrease in microcirculation. Further, he suggested in his study that kinesio-tape even leads to an increase in edema-formation as seen in our study. It has been recognised, that measuring the microcirculation can lead to several challenges methodological challenges, including controlling of applied pressure of the probe to avoid artefacts and temperature of the laboratory [17]. For this reason, the measurements of the microcirculation at times t0 and t6 were carried out in a laboratory in a clinic, which is air-conditioned and tempered at 21°C, in order to exclude measurement inaccuracies due to temperature differences.
In contrast to the applied kinesio tape (C) and the standard compression garment (B), the high-end compression garment (A) led to a reduction of edema. Similar findings were described by Aguilar-Ferrandiz et al. [18]. Aguilar-Ferrandiz et al showed in a randomized controlled trial that mixed kinesio taping-compression treatment improved peripheral venous flow and reduced edema as well as pain.
However, it is uncertain whether kinesio tape may only have a placebo effect on the reduction of pain. In the case of our examined compression garments, it is possible that the reduction of edema achieved with compression A was only because the compression pressure applied to the tissue was higher in comparison to garment B.
It is also important to note that many studies describe an improvement in range of motion through compression due to the reduction of edema and thus reduced soft tissue inhibition. However, our study showed different results. Both of the compression garments examined and the kinesio tape led to a reduction in range of motion. Even compression A, which led to a reduction in edema, did not lead to an improvement in range of motion measured by the commonly used neutral zero method. It is possible that the degree of change in swelling was not sufficient to affect mobility.
This investigation, like others, has limitations. First, we only assessed two different types of compression garments without great variance in compression pressure, which might have led to only small changes in microcirculation and edema reduction. Secondly, none of the patients examined were injured or had lymphatic disease, circumstances which could have otherwise led to greater formation of edema and therefore more drastic changes under compression.
Conclusion
Our findings could have significant implications for clinical practice within the field of sports medicine, as they demonstrate that the frequently used kinesio tape has no proven benefit in edema prevention. The study also shows that compression garments play an essential role in the prevention of edema formation, and that the degree of edema reduction depends on the degree of compression. Higher level of compressiom led to a higher rate of edema reduction. This is particularly important for patients with chronic venous insufficiency, post-trauma, or lymphedema, as the compression pressure is of relevant significance.
It is important to note that healthy subjects, with no lymphatic or venous conditions, are expected to show significantly less edema formation than individuals with existing preconditions. Nevertheless, there was an advantage of the compression garment (A).
It is possible that, for example, in high-performance athletes, could show a more pronounced change in edema formation under compression therapy.
Author contributions
Conceptualization,, Taeger, Diesch; methodology and examination, Kammermeier, Diesch; Schiltz, validation, Prantl, Kammermeier, Taeger, Diesch; formal analysis, Diesch, Kammermeier; investigation, Kammermeier Diesch; resources, Taeger, Diesch, Schiltz; data curation, Kammermeier, Diesch; writing—original draft preparation, Diesch; writing—review and editing, Prantl, Diesch, Taeger, Schiltz; visualization, Diesch; supervision, Prantl, Taeger, Diesch; project administration, Diesch, Taeger.
All authors have read and agreed to the published version of the manuscript.
Conflict of interest
There are no existing conflicts of interest.
Funding
This study received external funding from the company Cube. The compression garments were provided by the Company Cube. A study contract with the company Cube was signed through the University Hospital Regensburg. This relationship was reviewed by the University of Regensburg and concluded not to be relevant for the study’s outcome. All authors declare no conflict of interest.