
Abstract
AIM:
To evaluate the usefulness of handheld ultrasound in comparison with high-end ultrasound for lesion evaluation before and after sclerotherapy in pediatric patients with venous malformations (VMs).
MATERIAL AND METHODS:
10 pediatric patients prior to and after sclerotherapy were scanned by an experienced examiner using handheld ultrasound (Vscan AirTM) and high-end ultrasound (LOGIQ E9/E10) as reference. Patients with associated venous thromboses and intralesional aneurysms had been excluded. Results were interpreted independently by two readers in consensus.
RESULTS:
10 patients (4-17 years; 10.0±4.32 years; female n = 6, male n = 4) with 10 VMs (4 of the head and neck region, 4 of the upper and 2 of the lower extremities) were examined. 7 phleboliths were detected. The average rating score achieved by the high-end device never was less than 4, by Vscan AirTM never less than 3. An exception was the assessment of AV fistulas. In comparison with the evaluation of variables examined, we found a significant difference between the high-end scanner and the handheld device regarding the achieved image quality.
CONCLUSION:
Vscan AirTM ultrasound device allows new possibilities for procedure planning and post-procedural control of pediatric patients with VMs.
Introduction
A vascular malformation is an abnormal, non-neoplastic development of blood and/or lymph vessels. According to the ISSVA classification (updated 2018), vascular malformations can be divided into four categories: simple, combined, of major named vessels and associated with other anomalies [1]. Venous malformations (VMs) are simple, slow flow malformations with an estimated prevalence of 1% [2]. Most frequent locations of VMs are the head and neck region and the extremities with 40% each [3]. Multifocal lesions in a child should raise suspicion of a syndromic form as around 90% of VMs are usually unifocal [4]. VMs can be divided into superficial and deep lesions, the latter involving the deep venous system. The sonographic appearances of VMs vary from masses with saccular cysts to tubular or spongiform (honeycomb) shape [2]. They may contain phleboliths and usually show internal venous slow flow. Many lesions show a low vascular densitiy [5]. Particularly superficial VMs with well-defined margins are suited for sonographic evaluation [6].
Although clinically not always apparent, VMs are present at birth and tend to grow in proportion with the somatic growth. They commonly become more symptomatic during puberty as sex hormones stimulate angiogenesis and proliferation [7]. VMs can be associated with pain, thrombosis, functional compromise, arthropathy in case of articular involvement and cosmetic problems, all potentially reducing quality of life. Furthermore, large lesions can be associated with a systemic coagulopathy [8].
Sclerotherapy is considered the most important active treatment option in adults as well as children [8–10]. The injected agent is supposed to shrink the lesion and to reduce symptoms, especially pain. Generally, VMs cannot be cured, and multiple treatments are often necessary. With contrast-enhanced magnetic resonance imaging (MRI) being the diagnostic gold standard, ultrasound is a widely used device for diagnosis, therapy planning, procedure guidance and post-procedural control.
Due to their body habitus, children are generally well suited for ultrasound as a diagnostic tool, and the use of Point of Care Ultrasound (POCUS) in pediatric medicine is widely accepted and further increasing [11, 12]. The use of hand-held ultrasound (HHU) for POCUS applications in pediatric medicine has been described [11, 13–15]. Lately, pocket ultrasound devices were used widely for POCUS in many medical facilities during the COVID-19 pandemic [16, 17]. Recent advances in ultrasound-related technology allow new areas of application for modern handheld ultrasound devices (HHUD) [18]. At our institution, we use a pocket-size wireless scanner, Vscan AirTM [19]. This device combines the linear and convex probes with high-resolution in a wireless transducer and enables wireless image transmission.
In this single center, retrospective clinical study we evaluated, whether HHU is comparable to standard cart-based ultrasound in assessing the VMs with B-Mode and Color-coded Doppler sonography (CCDS).
Material and methods
Consent for the use of Vscan AirTM in pediatric patients was approved by the local ethics committee (23-3347-104). All ultrasound examinations with the high-end device were part of the standard operating procedure pre- and post-sclerotherapy and served as reference.
Patient cohort
A total of 10 patients (4-17 years; 10±4.32 years; female n = 6, male n = 4) were included. All patients were presented at our Vascular Anomalies Center between October 2022 and March 2023. All patients were diagnosed with a VM based on a thorough clinical examination, conventional ultrasound and contrast-enhanced MRI. All cases were evaluated by a multidisciplinary team and recommendation for therapy was given at the vascular malformation board meeting (held once to twice a month) prior to sclerotherapy. All patients presented with symptomatic VMs. They received a timely MRI before sclerotherapy. All parents gave written informed consent for the intervention. Patients were treated by an experienced interventional radiologist (Head of Vascular Anomalies Center) with percutaneous injection of Aethoxysclerol (Fig. 1), and in one lesion with Bleomycin. Maximum one day before and after sclerotherapy, patients received ultrasound for procedure planning, to rule out adjacent acute thrombophlebitis and deep vein thrombosis and show distribution of the sclerosing agent. All lesions were examined with non-contrast, conventional, cart-based high-end ultrasound and HHU by a certified pediatric radiologist with more than 15 years of experience in sonography. After sclerotherapy, no serious complications occurred. All patients were discharged one or maximum two days after intervention in good general condition.
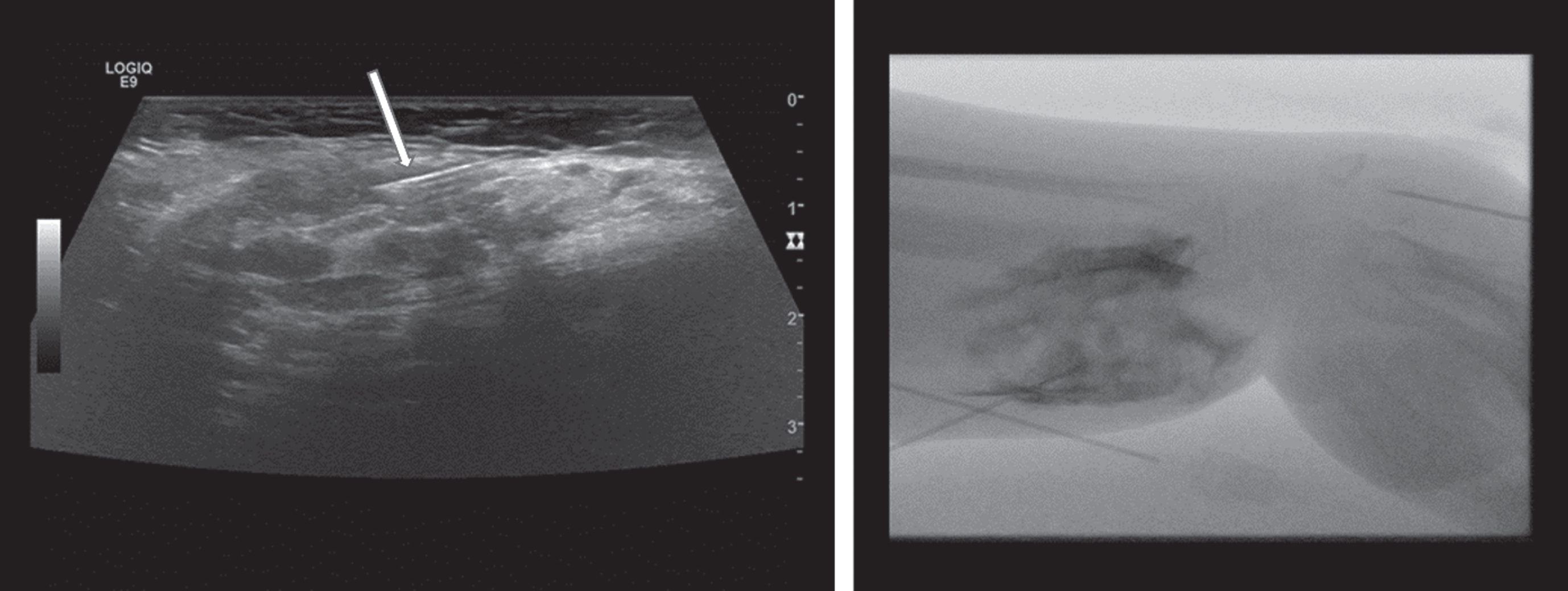
Sonographically guided percutaneous injection of gelified Aethoxysclerol (arrow pointing at needle) for treatment of upper extremity venous malformation in a 10-year-old girl (left). Distribution of sclerosing agent after sclerotherapy documented with Digital Subtraction Angiography (right).
Both the high-end device and the mobile device were developed by the same manufacturer, therefore a comparability of the two systems can be assumed.
Examinations with high-end ultrasound
We used a linear multifrequency transducer (6-9 MHz/2-10 MHz, LOGIQ E9/E10, GE Healthcare, USA). If anatomically possible, the whole affected area was examined. Solely non-contrast ultrasound was performed. Images were stored in our Picture Archiving and Communication System (PACS).
First, VMs were depicted by B-mode. Lesion extent and morphology was assessed. The presence of phleboliths was noted. Intralesional aneurysms were ruled out by B-Mode and CCDS. Furthermore, for detecting possible arteriovenous (AV) fistulas, also Spectral Doppler was used. Draining deep veins were evaluated using B-Mode, intermittent compression sonography and CCDS. Acute thrombophlebitis adjacent to the lesions was ruled out using the same technique. The presence of thrombosis was ruled out pre- and post-sclerotherapy.
Examinations with Vscan AirTM
We used the linear probe (3-12 MHz) of the HHUD (Vscan AirTM, GE Healthcare, USA). The wireless scanner was Bluetooth LE 4.0-connected to a touchscreen tablet PC. A mobile iOS device was used on which the corresponding function app had been installed. The battery of the HHUD could be charged quickly on site with inductive charging. Battery capacity lasted for approximately 50 minutes‘ scan time, sufficient for the evaluation of one VM. The obtained images were saved anonymously and password-protected - in compliance with applicable data protection regulations - on the used mobile device.
The same examination procedure using the HHUD was performed, except using Spectral Doppler, as this is currently not available in Vscan AirTM (Table 1).
Different examination modes used for sonographic evaluation of venous malformations (1 = used, 0 = not used)
Different examination modes used for sonographic evaluation of venous malformations (1 = used, 0 = not used)
*Not in Vscan.
Image quality was assessed using a score of grade “0” to grade “5”: 0 = no evaluation possible (e.g., in case of patient movement or due to artifacts), 1 = no diagnostic evaluation possible, 2 = major limitations of diagnostic evaluation (no reliable assessment), 3 = proportionate limitations of diagnostic evaluation but sufficient for a reliable assessment (e.g. due to post-interventional edema), 4 = only mild limitations of diagnostic evaluation, 5 = excellent image quality without limitations.
Documentation of the results was done in a proprietary Excel spreadsheet.
Evaluation procedure
Data were evaluated and read in consensus off-line by two readers (one experienced with more than 3000 examinations/year, more than 30 years of experience in sonography, DEGUM III, the other with more than 500 examinations/year, more than 15 years of experience in sonography, certified pediatric radiologist) blinded to the examination date. Results of both techniques were compared.
Statistical analysis
The program IBS SPSS Statistics version 29.0.0.0 (241) was used for statistical analysis. The Gaussian distribution of the collected data was tested by Shapiro-Wilk test, and regarding the small number of cases additionally by histograms and Q-Q plot testing. In the absence of a normal distribution, a hypothesis test of the paired samples was carried out by a Wilcoxon test otherwise by a paired t-test.
Results
10 patients with 10 interventions of 10 VMs were included (Tables 2, 3). Body mass index was in the normal range (no child was found to be obese). No VM was characterized as syndromic. There were 4 VMs of the head and neck region, 4 of the upper extremities and 2 of the lower extremities. On prior MRI, only one VM showed strictly epifascial localization. One patient with facial VM showed also deeper parts in the oral cavity and pharynx, which were not reachable by both ultrasound methods and therefore excluded. One patient with extensive VM of the leg showed intraarticular involvement of the knee with pre-existing flexion contracture, therefore the popliteal vessels could not be assessed; femoral and lower leg veins showed to be normal.
Demographic data of the studied cohort; VM = venous malformation f = female, m = male
Demographic data of the studied cohort; VM = venous malformation f = female, m = male
Mean and Median of the demographic data of the studied cohort; SD = Standard deviation, Q = quartile
Using B-Mode, we found slightly to moderately reduced quality of HHU compared to conventional high-end ultrasound (median 4.00 points with Vscan AirTM vs. 5.00 with the high-end device, Table 4).
Comparison of the evaluation score of the Vscan AirTM Device and the high-end Device, related to the evaluation criteria of the individual variables examined; Q = quartile
It was possible to determine extent and structure of sonographically accessible parts of lesions with no significant quality restriction (Fig. 2). HHU showed excellent image quality in superficial parts of VMs; deeper parts however showed limitations due to depth blur. AV fistulas could not be safely excluded by using B-Mode and Color-flow imaging with the HHUD alone, as there was no possibility for assessment with quantitative flow measurement (Table 5).
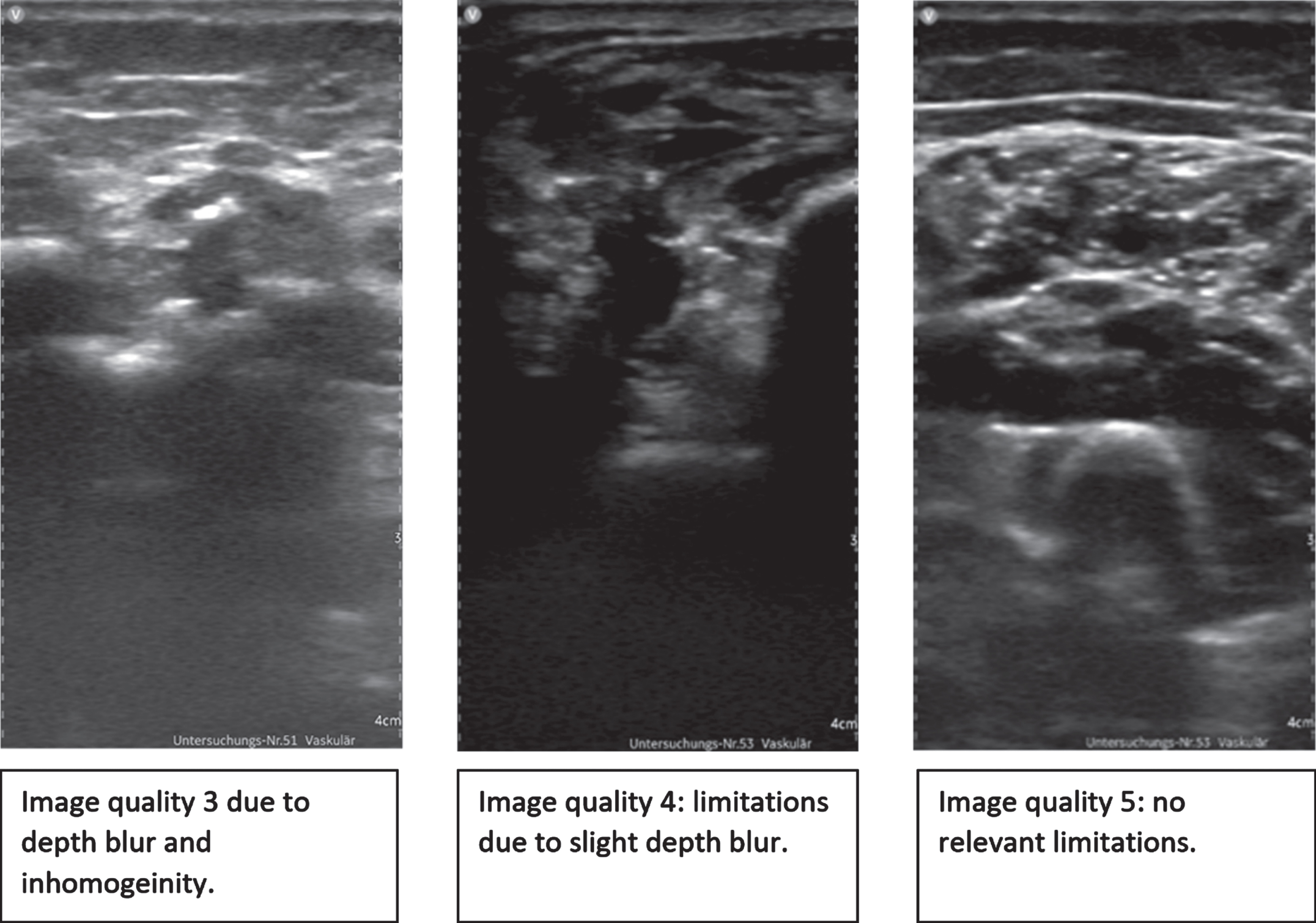
Illustration of image quality using the Vscan AirTM linear probe for VM assessment.
Overview presentation of detected diagnoses in the studied cohort; 0 = No, 1 = Yes, X = no diagnosis possible with Vscan AirTM because of no possibility for flow measurement
In seven VMs, at least one phlebolith was found, with no differences between the two scanners (Fig. 3).
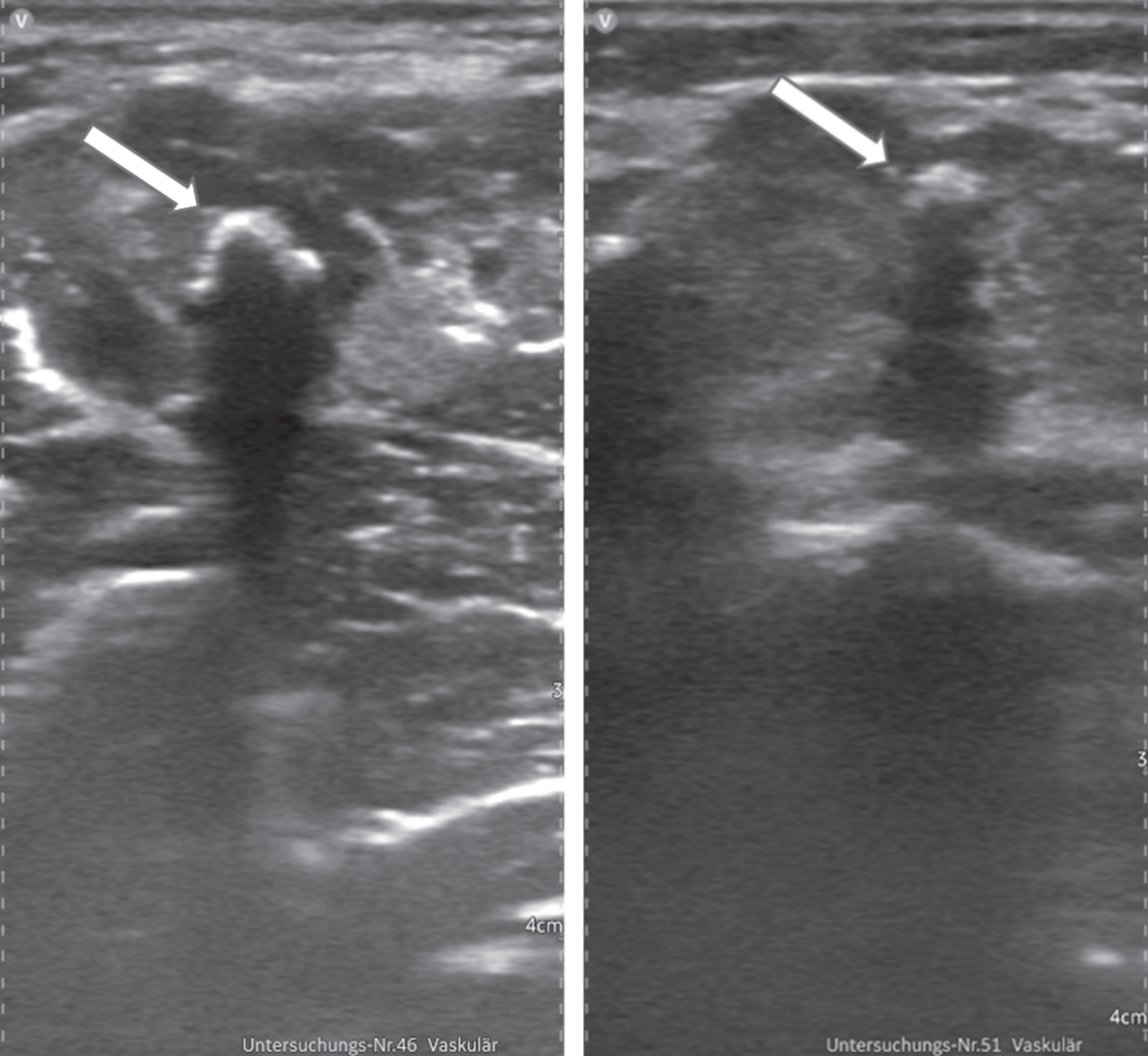
Excellent depiction of phleboliths (arrows) with Vscan AirTM.
No aneurysms were detected in or in the proximity of the VMs. No patient was found to have associated deep vein thrombosis (DVT) or acute thrombophlebitis prior to or after sclerotherapy. A total of at least 3 points were scored in the evaluation of thrombosis/thrombophlebitis (Fig. 4) and detection of intralesional aneurysms by the HHUD.
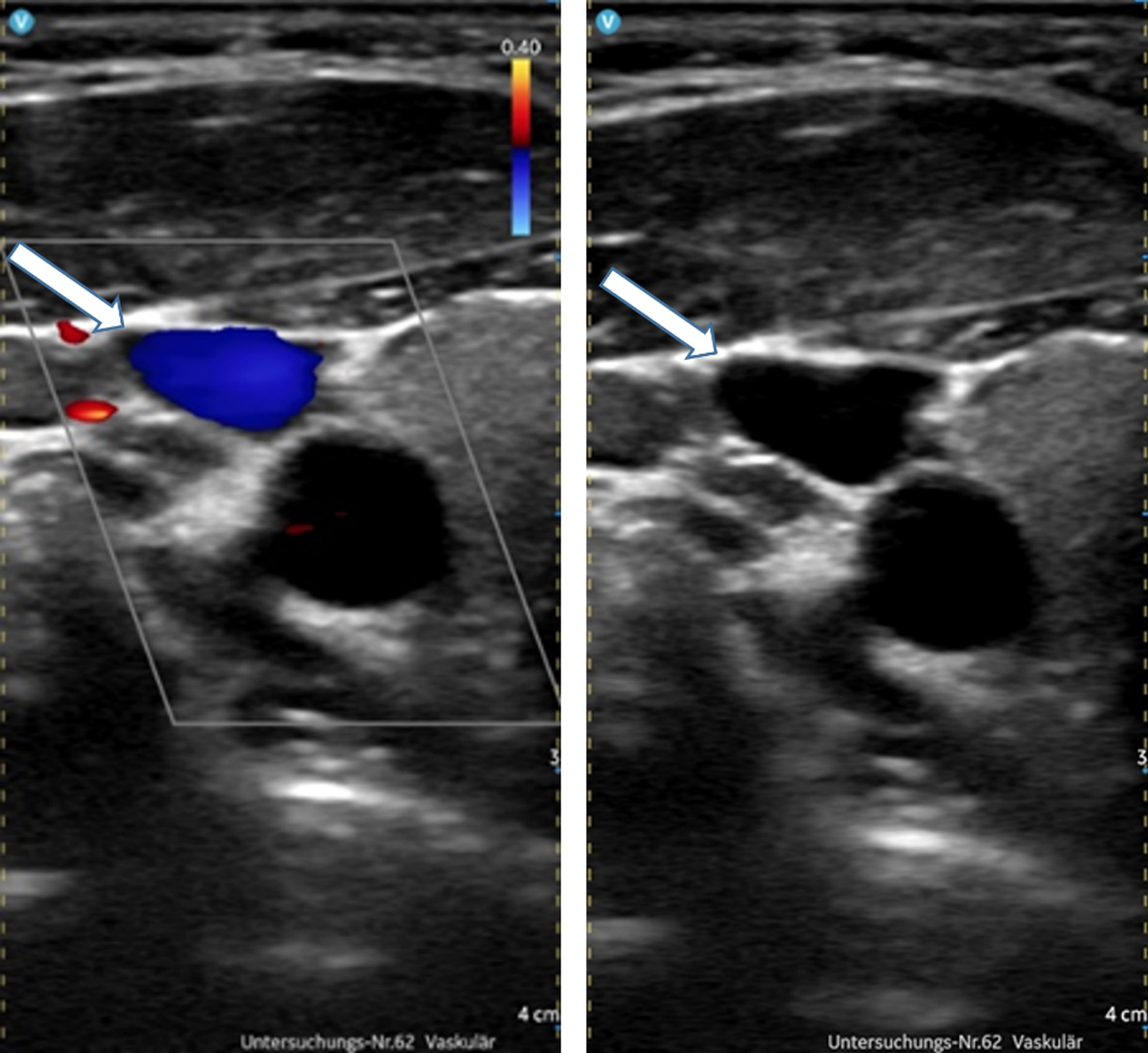
Image quality 5. Exclusion of thrombosis of right jugular vein (arrows) with Vscan AirTM using B-mode (right picture) and CCDS (left) with no relevant limitations.
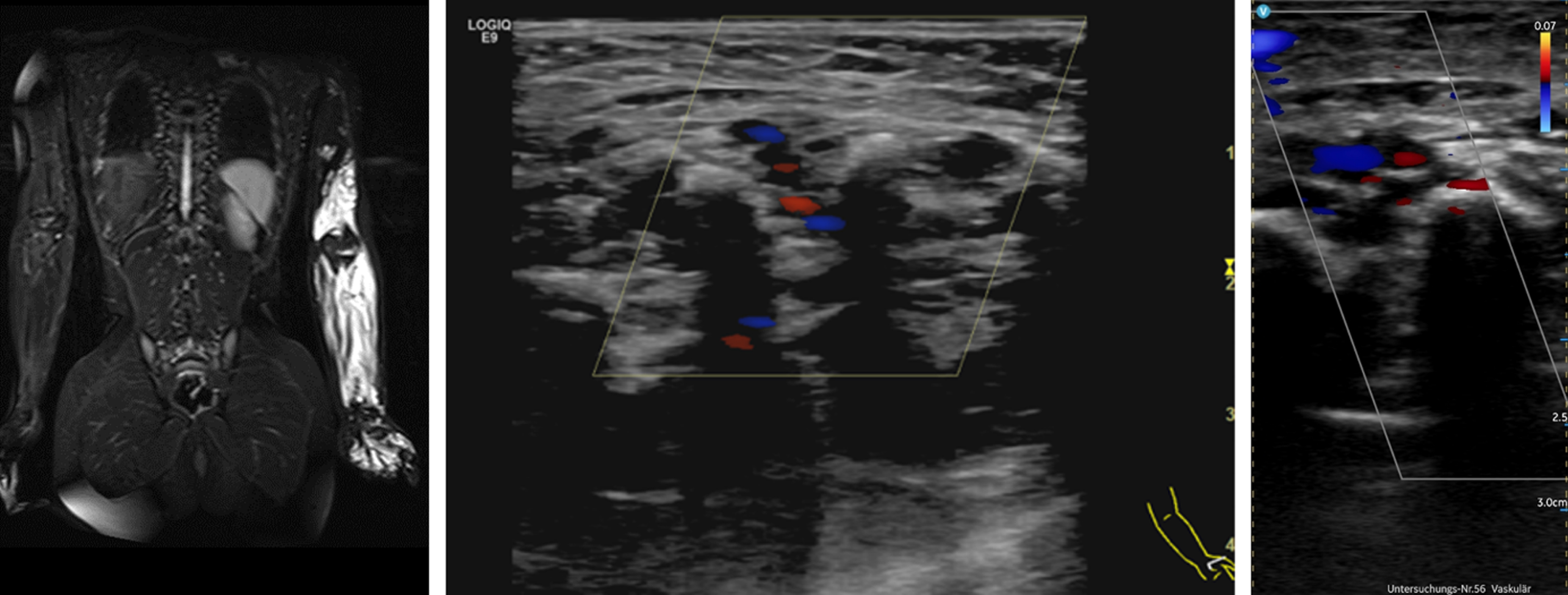
HHU showed to be inferior to conventional high-end ultrasound in detecting internal flow, especially in small slow-flow vessels (Fig. 5). Motion artifacts showed more often than with high-end ultrasound (Fig. 6).

VM of lower lip in 7-year-old girl (arrow). Restricted depiction of intralesional flow shown with Vscan AirTM (right image) compared to high-end ultrasound (middle).
Extensive upper extremity VM of 9-year-old boy. CCDS with Vscan AirTM (right) showing limitations due to motion artifacts.
VMs are the most common vascular anomalies referred for intervention [20]. Sclerotherapy is a well-established treatment option for symptomatic VMs. Evaluation of the lesions prior to treatment and post-procedural assessment with ultrasound are standard of care at our institution. Particularly children with in general lower body fat than adults and better accessibility of deeper body parts due to their anatomy are suited for sonographic evaluation.
Recent advances in ultrasound technology have made HHUD more versatile and easier to use than ever [21, 22]. They are mobile and ubiquitously applicable scanners. HHUD are much easier to disinfect than cart-based devices, advantageous not only when dealing with COVID-patients. Therefore, HHUD are increasingly utilized for POCUS in many different settings in adults as well as children, for example in perioperative or outpatient care. New IT solutions for data transfer and storage and artificial intelligence (AI)-based optimization of image quality are helping to push the boundaries. Furthermore, we consider HHU very useful for bed-side education at our institution [17].
To the best of our knowledge, this pilot study is the first study to evaluate the periprocedural use of HHU in children and adolescents with symptomatic VMs. Data indicate that the use of Vscan AirTM allows pre-procedural assessment of VMs with sufficient diagnostic quality, including the exclusion of associated venous thromboses. Image quality using B-mode of Vscan AirTM has not fallen below 3. However, we do not recommend using HHU as sole device in diagnosing malformations, as there are important limitations: Detection of intralesional flow especially of small slow-flow vessels showed to be inferior using HHU compared to high-end ultrasound equipped with more powerful Color-coded Mode and other possibilities, especially Spectral Doppler. The study indicates that the exclusion of AV-fistulas cannot be made reliably using HHU alone. Also, deep parts of lesions seem to be better depicted with high-end ultrasound; the use of HHU for deeper body parts especially in overweight adolescents should be carefully considered. Patients of our study showed no VM of the trunc; therefore, we could not assess deeper intrathoracic or intra-abdominal lesions.
An important issue is a reliable and safe data storage infrastructure. Currently, there is no possibility for data transfer from Vscan AirTM to the PACS at our institution, therefore its current use is limited to an ,,add-on“-device.
Nevertheless, we consider the aim of HHU not to replace high-end ultrasound, but to perform a focused and quick examination sufficient to answer specific questions, for example in peri-procedural care. HHU can be used bedside and integrated in daily patient management. Furthermore, we found the pocket-sized scanners being well tolerated by our pediatric patients, probably because of their small size and the children‘s familiarity with smartphones and tablets, as described before [13].
Limitations
This pilot study is limited by the small number of patients. It is a single-center study and retrospective. Our results may not be generalizable to all pediatric patients. Due to the technical equipment of the Vscan AirTM, only a comparison of the B-scan and CF-Mode with the high-end device could be performed. An extension of the Vscan AirTM to include a Spectral Doppler mode for flow assessment would be a useful addition here, which would be in line with other studies [18].
Conclusion
Our first experience with the new HHUD at our institution for procedure planning and post-procedural control of pediatric patients with symptomatic VMs is promising. Further studies with greater patient numbers need to be conducted. We expect future HHUD to be equipped with a sound Doppler examination technique, allowing better diagnostic value in the future.
Conflicts of interests
The authors have no potential conflicts of interest to declare.