
Abstract
OBJECTIVE:
Thrombosis represents one of the most feared complications of the COronaVIrus Disease-2019 (COVID-19). Although pulmonary embolism and deep venous thrombosis are the most described complications, some investigations reported thrombotic localization also in the splanchnic venous district.
METHODS:
We describe the case of a patient with SARS-CoV-2 infection presenting with abdominal pain and diagnosed with portal vein thrombosis. In addition, we shortly review available literature supporting the possible role of COVID-19 as leading cause of splanchnic venous thrombosis.
RESULTS:
After in-depth diagnostic workup, we excluded the commonest causes of portal thrombosis and concluded that SARS-CoV-2 infection represented the main explanation of this finding.
CONCLUSIONS:
Our study warns the clinicians to maintain a high index of suspicion for thrombosis in patients diagnosed with SARS-CoV-2 infection manifesting gastrointestinal symptoms. An appropriate diagnostic work-up could allow to obtain an early diagnosis and consequently improve the clinical outcome of patients.
Introduction
Systemic hypercoagulable state and coagulation disorders represent the hallmark of the COronaVIrus Disease-2019 (COVID-19) [1, 2]. This condition leads to the vessel occlusion in both arterial and venous districts [3, 4]. Although pulmonary embolism and deep venous thrombosis are the most described complication [5], some investigators had reported thrombotic localization also in the splanchnic venous district [6, 7].
In the present paper, we report the case of a patient with SARS-CoV-2 infection presenting with porto-mesenteric vein thrombosis, without pneumonia. In addition, we shortly review current literature supporting the possible role of COVID-19 as leading cause of splanchnic venous thrombosis.
Case description
In October 2020, a 58-year-old Asian man came to the Emergency Department of our Hospital for the appearance of fever and abdominal pain. He not referred diarrhea or vomit, nor respiratory symptoms. His medical history was unremarkable. He did not take any medications and not referred history of smoking or alcohol consumption. He underwent to the nasopharyngeal swab screening for the RNA detection of SARS-CoV-2, which resulted positive and was admitted to the Internal Medicine Unit in the COVID-19 section. On admission, the patient was eupnoic, oxygen saturation was 99%on air room. Physical examination showed abdominal distention, with tenderness on deep palpation in the epigastric region. Laboratory data blood tests revealed normal leukocyte and lymphocytic count, PT and aPTT in normal range, D-Dimer 2.16 mg/L (n.v. < 0.55), Fibrinogen 669 mg/dL (n.v. 150–400), C-reactive protein 6.11 mg/dL (n.v. < 0.5), ALT 25 U/L, AST 27 U/L, serum bilirubin 2.57 mg/dL, Lipase 32 U/L and Creatinine 0.86 mg/dL. Blood gas analysis showed pH 7.41, pO2 85 mmHg, pCO2 42 mmHg and HCO3– 27 mmol/L, P/F ratio 404. High resolution computed tomography (CT) didn’t show ground glass aspect or other sign of interstitial pneumonia. Abdominal ultrasound revealed normal liver and spleen structure, but absent anterograde flow in the portal vein consistent with thrombosis (PVT) (Fig. 1). Contrast enhanced abdominal CT, confirmed the portal vein occlusion extended to superior mesenteric vein with collateral vessels, duodenal wall alterations (Fig. 2 a, b) and a cephalo-pancreatic inhomogeneity. Echo-endoscopy confirmed PVT with intrahepatic and peri-coledocic collateral vessels without pancreas alteration (Fig. 3). No esophageal varices or other pathological findings were observed at the esophagogastroduodenoscopy. Neoplastic biomarkers (CA-19.9 and CEA) were in the normal range; hepatitis C serology was negative, whereas hepatitis B markers were positive (HBs Ag 249 U/L, HBV DNA 35 UI/ml, Ab anti HBs 2 mUI/ml, Ab anti HBc positive) and indicated a state of “inactive HBV carrier”. Thrombophilia screening (including JAK 2 mutation and lupus anticoagulant) was negative. The patient started Enoxaparin (8000 IU bid) for one month and subsequently he switches to Rivaroxaban 20 mg/die. No specific therapy is initiated for SARS-CoV-2 infection given the absence of respiratory symptoms.
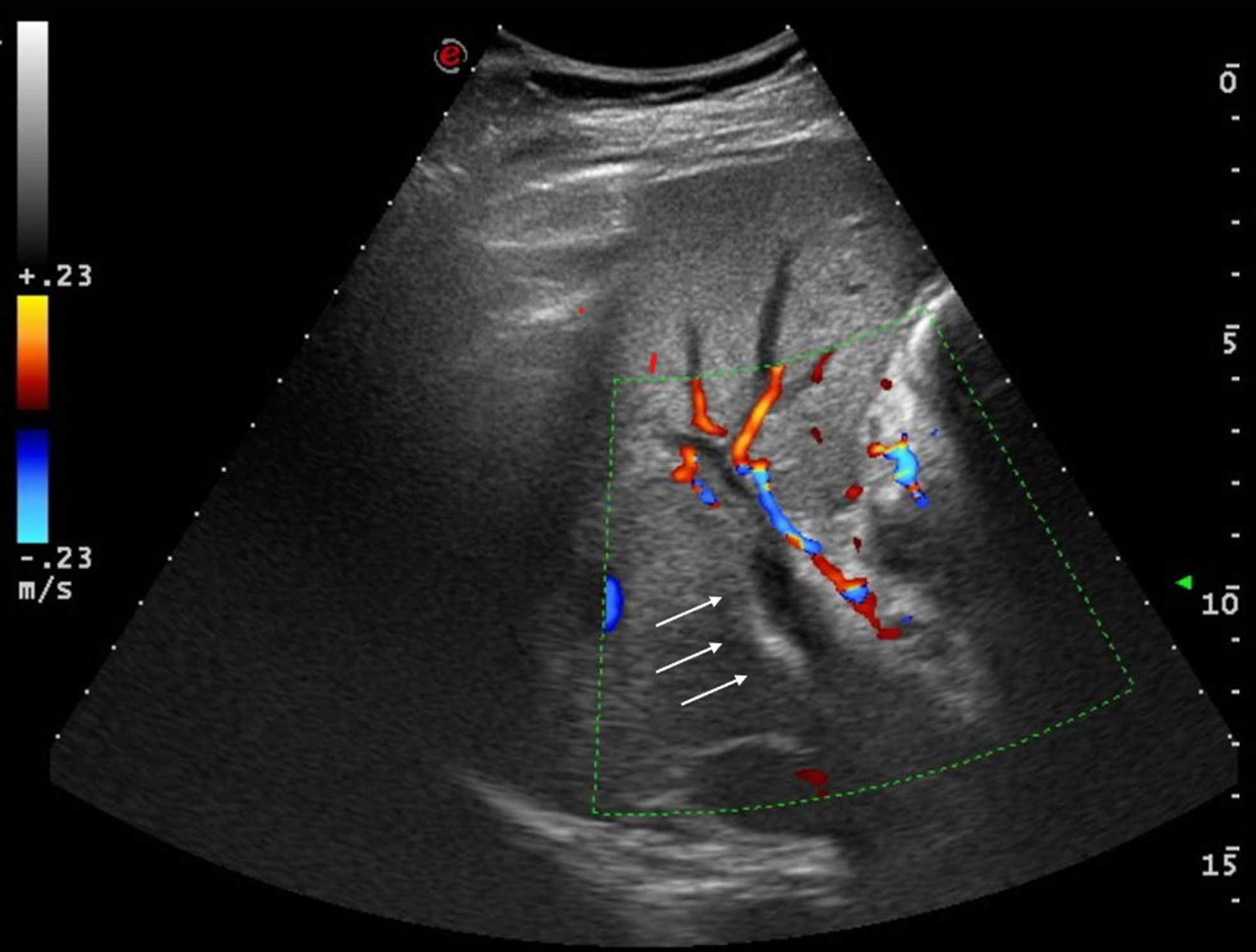
Abdominal ultrasound showing portal vein thrombosis.
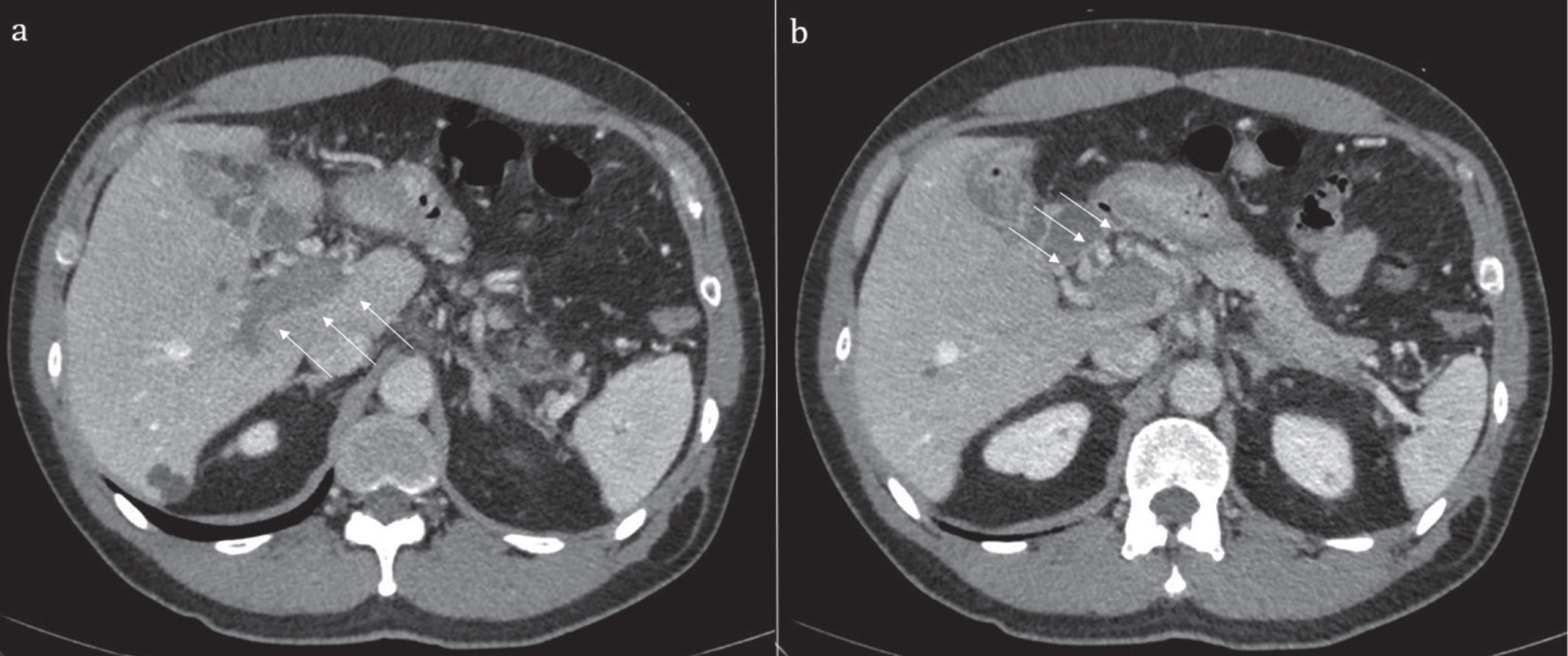
Contrast enhanced computed tomography showing portal vein thrombosis (a) and collateral vessels (b).
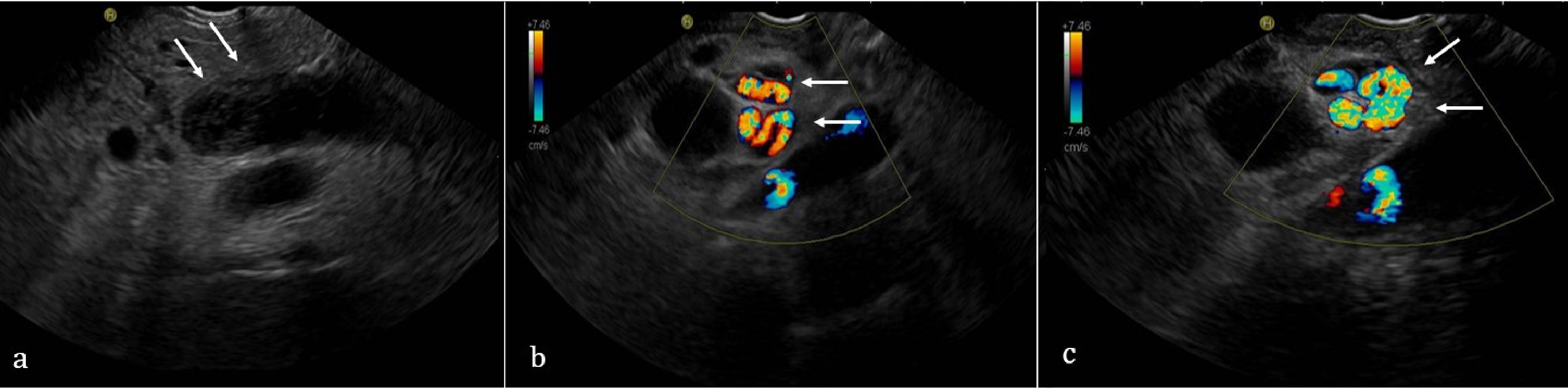
Echo-endoscopy showing portal vein thrombosis (a) and collateral vessels (b and c).
Three months later, the patient came to our attention for an ambulatory follow up visit. He referred well-being and good adherence at the anticoagulant therapy. He underwent contrast enhanced ultrasound (CEUS) of abdomen showing portal cavernoma with a normal blood flow; patency of the right, left and intrahepatic portal branches; peri-gastric collateral vessels. We decided to continue the anticoagulant therapy for another three months.
In the present paper, we described the case of a patient diagnosed with SARS-CoV-2 infection presenting with portal vein thrombosis but without pneumonia. COVID-19 typically presents with flu-like symptoms such as cough and sore throat but it can progress to interstitial pneumonia, bronchitis, and acute respiratory distress syndrome. Besides pulmonary complications, COVID-19 is characterized by a prothrombotic milieu leading to thrombosis in various vascular district [1]. The exact mechanisms of these disorders are not fully elucidated, but it seems that COVID-induced coagulopathy might be the consequence of a complex interplay between systemic inflammation, thrombosis, and endothelial dysfunction. The combination of these factors might be at the basis of the pro-coagulative state observed during SARS-CoV-2 infection [8, 9]. Pulmonary embolism and deep venous thrombosis are the most described thrombotic complications. A recent meta-analysis found a cumulative in-hospital rate of acute pulmonary embolism in general wards of 14.7%. Higher rates were described in intensive care unit patients, with a pooled cumulative incidence rate of 23.4%[5].
Accumulating evidence from clinical case reports suggested that thrombotic manifestation might also develop into unusual sites such as portal and mesenteric vein [6]. Usually, PVT is observed in advanced chronic liver disease (cirrhosis, liver malignancy), whereas in normal liver, PVT is mainly the consequence of the combination between local and systemic prothrombotic factors such as abdominal inflammatory processes, thrombophilia, and JAK 2 positive mielo-proliferative neoplasm [10]. The gastrointestinal system is involved in the COVID-19 often in association with respiratory complications; indeed SARS-CoV-2 can infect intestinal epithelial cells through the angiotensin-converting enzyme 2 receptors. Furthermore, SARS-CoV-2 RNA has been detected in feces of infected patients [11]. Abdominal pain, nausea, vomiting, diarrhea and elevated transaminases are the commonest signs. Of note, in rare cases the gastrointestinal involvement in COVID-19 is characterized by thrombotic complications in both arterial and venous splanchnic district [6, 7]. Below, we reviewed current literature about this topic, focalizing on thrombotic complications in the venous district.
Table 1 summarizes all available cases of porto-mesenteric vein thrombosis in the course of COVID-19. Although a definite conclusion cannot to be drawn, these evidences allow us to make some considerations. First, splanchnic thrombosis doesn’t seem to have specific gender or age predilection. Males are slightly more affected than females, whereas age ranges from 22 to 79 years with a median of 46 years. Second, unspecific symptoms such as abdominal pain (with or without fever) and vomit are the commonest modalities of presentation, but some patients experienced severe gastrointestinal complications. Third, portal vein represents the more involved site of thrombosis, sometimes isolated and in other cases associated with mesenteric veins thrombosis (7 isolated PVT, 6 PVT with mesenteric veins, 3 only mesenteric veins). Only a few studies performed the thrombophilia screening (including JAK2 mutation) and, except for the lupus anticoagulant positivity in two cases, none other alteration were found. The clinical consequences of thrombosis as well as treatment are heterogeneous. The most not developed signs of gastro-intestinal ischemia so that they could effectively managed with conservative therapy (heparin, warfarin or new oral anticoagulants). In more severe cases, patients need emergent surgical intervention since they developed gastro-intestinal ischemia. In these last cases patients had the worse outcome, with prolonged hospitalization or death.
Summary of current reports describing splanchnic vein thrombosis in patients with COVID-19
The mechanism of this unusual localization is difficult to understand and far to the aim of this paper. However, we can propose some mechanistic hypotheses. In a recent paper, Sonzogni et al. described the liver histological findings in COVID-19, such as: microvascular alterations, increased number of portal vein branches associated with lumen dilatation, partial or complete luminal thrombosis of the portal and sinusoidal vessels, and fibrosis of portal tract [28]. Liver and pulmonary microvascular alterations were also described by Jung et al, through the use of CEUS, in patients with severe COVID-19 [29, 30]. On these bases, we can speculate that systemic inflammation and local microvascular alterations could favor thrombotic complications in main venous districts.
In our clinical case, an interesting point needing to be highlighted is the absence of any pulmonary involvement. Indeed, the patient didn’t need supplemental oxygen therapy; furthermore, the chest CT not showed typical alterations. In our opinion this represents an important finding since it demonstrates that COVID-19-induced hypercoagulability (and possibly endothelial damage as well) can occur in all vascular districts, regardless of respiratory involvement and its severity. SARS-CoV-2 has a broad spectrum of organotropism beyond the respiratory tract, and it is possible than in some subjects the endothelium-tropism is more pronounced.
The major strength of the present work is the wealth of clinical information available. Indeed, we adopted a comprehensive diagnostic work-up allowing us to exclude the most common causes of portal thrombosis (such as hepatic cirrhosis, neoplastic diseases, thrombophilia disorder). So, we can affirm with reasonable certainty that SARS-CoV-2 infection is the main cause of portal thrombosis in our patient.
In conclusion, we described the case of COVID-19 related portal vein thrombosis in a patient free of respiratory involvement. In our opinion, this manuscript contains two main messages. First, it highlights the multifaceted modalities of presentation of COVID-19, beyond interstitial pneumonia. Second, it invites the clinicians to maintain a high index of suspicion for thrombosis in patients diagnosed with SARS-CoV-2 infection manifesting gastrointestinal symptoms. An appropriate diagnostic work-up could allow to obtain an early diagnosis and consequently improve the clinical outcome of patients.
Footnotes
Acknowledgments
None.
Conflict of interest
None declared.