
Abstract
BACKGROUND:
Lymphocyte-to-C-reactive protein ratio (LCR) has been used as a post-surgical prognostic biomarker in patients with gastric and colorectal cancer. However, its relationship with early postoperative complications in these patients is unknown. In this study, we aimed to reveal the relationship between LCR and postoperative complications.
METHODS:
Eighty-one patients operated for stomach and colorectal cancer between January 2020 and August 2020 were prospectively analyzed. On preoperative and postoperative days 1, 3 and 5, other inflammatory parameters, mainly LCR, neutrophil lymphocyte ratio (NLR), were recorded. The patients were divided into two groups according to Clavien-Dindo classification as stage III and higher complications major, stage I-II/non-complication minor.
RESULTS:
Fifty seven patients were operated for colorectal cancer, 24 patients for gastric cancer. The mean age of the patients was 65.6
CONCLUSION:
Among different inflammatory markers, postoperative LCR is a safe and effective predictor of postoperative complications, especially after gastric and colorectal cancer surgery on day 5.
Introduction
Among major abdominal oncological surgeries, surgery for stomach and colorectal cancer is among the most frequently performed operations today. Despite recent advances in advanced surgical techniques, perioperative care, and the quality of nutritional support, it is natural to see life-threatening complications in cases where these major resection and reconstruction procedures are performed. As a matter of fact, postoperative complication rates after gastric and colorectal surgery were reported as 46% and 40%, respectively [1, 2]. Serious postoperative complications such as anastomotic leak, surgical site infection, sepsis and multiple organ failure do not have specific early signs and symptoms, these patients can be diagnosed late [3]. When postoperative complications are added to the inflammatory response that occurs after surgery, the inflammatory response increases even more [4]. This response can be predicted by biomarkers that can help surgeons monitor patients and diagnose life-threatening complications early.
In previous studies, various systemic inflammatory markers have been shown to be independent pretictors for postoperative complications in different types of surgery [4, 5, 6, 7]. However, a limited number of studies were associated with inflammatory markers and postoperative complications after gastric and colorectal cancer surgery [1, 6, 8]. Additionally, it has been reported that as the level of inflammation gets more severe, the decrease in the number of lymphocytes increases significantly in addition to neutrophilia [9].
NLR correlates with the severity of systemic inflammation and show the severity the disease for different diseases in many studies [10, 11, 12]. Recent articles have shown that NLR may be associated with postoperative complications after major abdominal oncologic surgery [13, 14].
Lymphocyte-C-reactive protein ratio (LCR) has come to the fore in recently, and it has been shown to be associated with the severity of systemic inflammation [15]. It has also been shown that it can be used to predict the prognosis of the disease in some types of cancer [16, 17]. In a recent study, low LCR and high NLR levels predicted poor prognosis and high in-hospital mortality in patients with coronavirus disease 2019 (COVID 19) [18].
The purpose of this study is to investigate the correlation and predictive value of LCR, a new biomarker, between complications that may develop after gastric and colorectal cancer surgeries. As far as we know, this study may be the first study on LCR in this area in the English literature.
Matherial and methods
Design
This prospective observational study was performed in the general surgery clinic of Tokat Gaziosmanpaşa University (TOGU) education and research center. Patients who underwent elective, potentially curative resection for histologically confirmed gastric and colorectal cancer between January 2020 and August 2020 were included. Complete data were available for 81 patients. The work permit was approved by the TOGU medical school ethics committee (20-KAEK-189) and informed consent was obtained from all patients.
Patients
Demographic data of the patients (age, gender), primary disease, American Society of Anesthesiologists (ASA) classification, preoperative body mass index (BMI), operation details (operation time, intraoperative complication, blood transfusion), type of surgery (subtotal-total gastrectomy, right hemicolectomy, left hemicolectomy, low anterior resection, abdominoperineal resection, total colectomy) and postoperative complications were prospectively collected in a database, anonymized, and then analyzed.
The operation decision was made by the weekly multidisciplinary tumor council in our clinic. Operations were performed using a laparoscopic and open approach. A drainage tube was placed in the abdomen in all operations. Mechanical bowel cleansing was routinely applied to patients undergoing colorectal resection. All patients were administered pre-prophylactic antibiotics (1 g cefazolin intravenously) 30 min before the operation and as an additional dose to patients whose operation time exceeded 3 hours. All patients were taken to the postoperative intensive care unit. Patients in good general condition were transferred to the general surgery service the next day. All patients were administered postoperative antibiotics (2nd or 3rd generation cephalosporin and metranidazole, intravenous for colorectal cancer patients) and low molecular weight heparin. Routine D2 lymph node dissection was performed in patients undergoing gastrectomy. Routine mesocolic and mesorecral excision was performed in patients who underwent colorectal surgery.
Our exclusion criteria were patients under the age of 18, patients who were considered unresectable during surgery, emergency operated patients, patients with acute liver and kidney failure and cirrhosis, and ongoing infections before surgery.
Comparison of baseline characteristics between research groups
Comparison of baseline characteristics between research groups
Comparison of laboratory values, NLR and LCR values of patients according to complication status
Most of the patients were treated according to our postoperative clinical management. On postoperative 1st day, patients were mobilized according to their general condition and urinary catheters were removed. Patients were allowed to take water on the second postoperative day. If their general condition was good, a soft diet was started on the 2nd and 3rd days. Then, drainage tubes were removed. The patient was discharged on the 6th or 7th postoperative days with the decision of the surgeon who operated.
Blood sample analysis
Blood samples were taken on the preoperative and postoperative 1st, 3rd and 5th days. Neutrophil, lymphocyte, platelet, white blood cell (WBC) counts, C-reactive protein (CRP) level, neutrophil lymphocyte ratio (NLR) and lymphocyte to CRP ratio (LCR) were recorded in the prospective database. LCR was calculated as Lymphocyte (number/microliter)/CRP (mg/liter), and NLR as Neutrophil (number/microliter)/ lymphocyte (number/microliter).
Evaluation of postoperative complications
Postoperative complications include surgery (presence of intrabadominal abscess, anastomotic leak, wound site infection, bleeding, ileus, pancreatitis, pancreatic fistula) and non-surgical (pneumonia, atelectasis, acute myocardial infarction, urinary tract infection, line infection, acute renal failure, pulmonary embolism, etc.) were defined as complications. Clavien-Dindo classification system was used for the classification of all postoperative complications. The patients were divided into two groups as postoperative major (more than stage III according to Clavien-Dindo classification) and minor complications (stage I/II or no complications). Mortality was defined as death within 30 days from the date of surgery.
a. Line chart for preoperative and postoperative changes in NLR in patients with major complications versus minor or uncomplicated patients. The X-axis shows NLR measurements obtained at different times. The Y-axis shows the mean of the NLR values. NLR preop: NLR-preop is the mean of NLR values measured before surgery from patients. NLR 1: NLR value measured at the 1st hour. NLR 3: NLR value measured at the 3rd hour. NLR 5: NLR value measured at the 5th hour. b. Line chart for preoperative and postoperative changes in LCR in patients with major complications versus minor or uncomplicated patients. The X-axis shows LCR measurements obtained at different times. The Y-axis shows the mean of the LCR values. NLR preop: NLR-preop is the average of LCR values measured before surgery from patients. LCR 1: LCR value measured at the 1st hour. LCR 3: LCR value measured at the 3rd hour. LCR 5: LCR value measured at the 5th hour.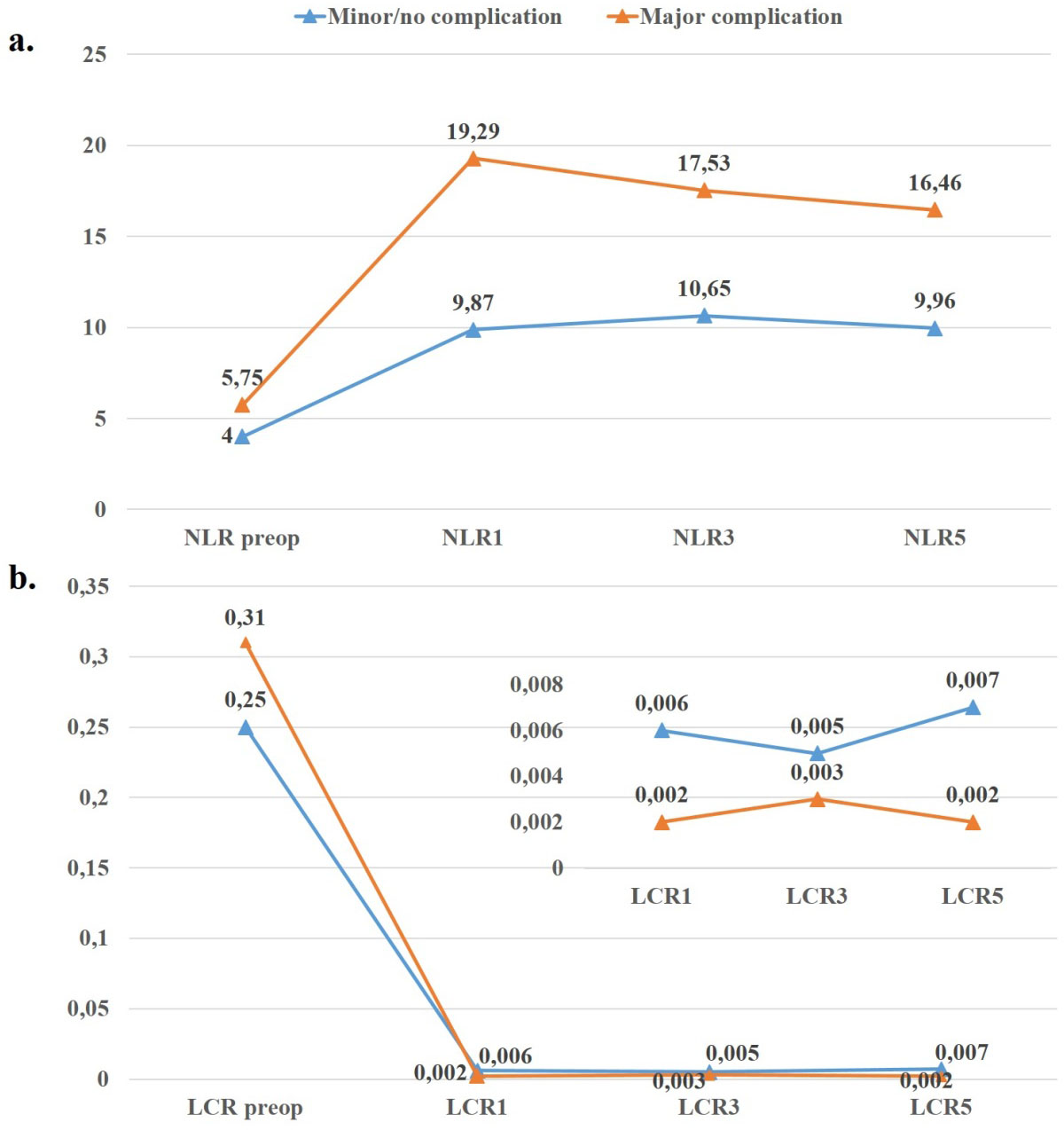
Statistical analysis was carry outby using SPSS (Version 22,0, SPSS Inc., Chicago, IL, USA) software. Descriptive statistics were presented as mean
Results
A total of 81 patients were included in the study. The clinical characteristics of the study population and the comparison of the characteristics and clinical features between the patients who did not develop complications (no) and/or developed minor complications and the patient groups who developed major complications are presented in Table 1.
34.6% (
Age, operation time and hospital stay was significantly different among the study groups (
ROC (Receiver Operating Characteristic) analysis results for LCR, and NLR values with sensitivity, specificity, positive-negative predictive values and likelihood ratio (
) values
ROC (Receiver Operating Characteristic) analysis results for LCR, and NLR values with sensitivity, specificity, positive-negative predictive values and likelihood ratio (
LCR: Lymphocyte to C-reactive protein (CRP) ratio, NLR: Neutrophil to lymphocyte ratio, AUC: Area under the ROC curve, CI: Confidence interval, PPV: Positive predictive values, NPV: Negative predictive values, LR: Likelihood ratio.
a. ROC (Receiver Operating Characteristic) curves for LCR1 values b. ROC (Receiver Operating Characteristic) curves for NLR3 values c. ROC (Receiver Operating Characteristic) curves for NLR5 values.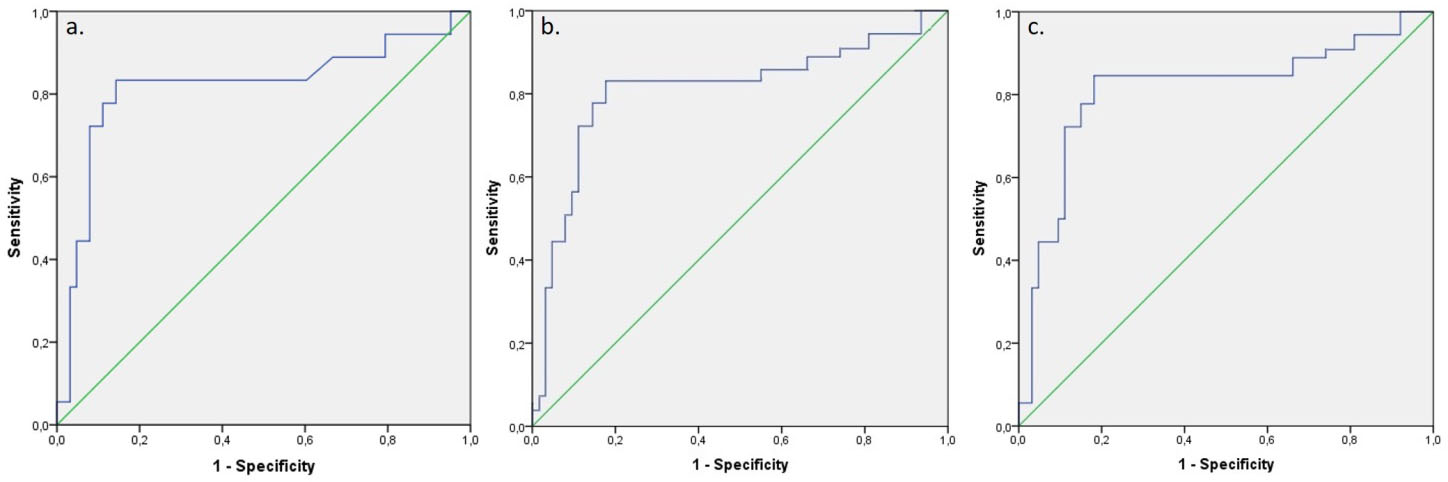
The number of overall and major complications were 32 (39.5%) and 18 (22.2%), respectively. Major complications included anastomosis-related complications in 6 patients, intra-abdominal abscess and related complications in 3 patients, pancreatic fistula in 2 patients, intestinal obstruction in 1 patient, wound evisceration in 1 patient, stoma necrosis in 1, and cardiopulmonary complications in 4 patients. The mean day of onset of major complications was 6.3 days on average. Eight of these patients were operated under general anesthesia again. Other patients were managed with percutaneous drainage and medical treatment methods. 2 patients died due to multiple organ failure after anastomotic leak, despite all interventions. The death days of these patients were 8 and 11 days postoperatively.
Comparison of laboratory values, LCR calculated at different time points, and other inflammatory factors between the major and minor/no groups are presented in Table 2.
There was no statistically significant difference only in pre-op values for lymphocyte (lym), CRP, neutrophil (neu), LCR, and NLR between the groups (respectively,
Wbc 1st day measurements were significantly different between groups (
ROC (Receiver Operating Characteristic) analysis results and sensitivity, selectivity, positive-negative predictive values and likelihood ratio (
Univariate regression analysis results to determine the effect of age, gender, LCR and NLR values on complication prediction
Reference value for LCR1
Because of the ROC analysis, all of the LCR parameters calculated at 3 times were found to be significant at the good level in distinguishing the complication level (0.8
The results of the Univariate regression analysis was performed to determine the OR values in the complication estimation are given in Table 4.
Since there was a correlation between variables found to be significant in the univariate model, it could not be established in the multivariate model, no multivariate model could be established. According to the univariate model results, the OR for the age variable was found to be 1.08 (CI 95%: 1.02–1.12). OR for LCR1, LCR3 and LCR 5 variants was 4.62 (95% CI: 1.9–10.9), 3.99 (95% CI: 1.42–9.8) and 4.80 (95% CI: 2.1–11.8), respectively. The OR for NLR1, NLR3, and NLR 5 variables was found to be 3.87 (95% CI: 1.29–9.07), 2.86 (95% CI: 1.09–7.08), and 3.71 (95% CI: 1.13–8.53), respectively (Table 4).
This study is the first to our knowledge to investigate the use of LCR to predict postoperative surgical complications in the early period in patients with confirmed gastric and colorectal carcinoma undergoing resection in a surgical oncology clinic in a peripheral tertiary research hospital. The early postoperative low LCR rate was demonstrated as an independent predictor of a major postoperative event.
Several studies conducted inrecently revealed between postoperative complications after gastric and colorectal surgery and inflammatory markers such as CRP, NLR, procalcitonin, and interlocin-6 [4, 19, 20]. However, none of these inflammatory markers have been proven to be the gold standard. In our study, we used LCR, which has recently been used as a new biomarker. Additionally, we examined different inflammatory biomarkers previously used.
It has been stated in the last few studies that LCR can be used as a prognostic inflammatory marker in gastric, colorectal and hepatobiliary cancers. Cheng et al. [16] investigated the prognostic predictive value of LCR in 607 gastric cancer patients who underwent radical gastrectomy. Preoperative low LCR patients experienced more postoperative complications than patients with high LCR (20.4% vs 12.1%,
In our previous study, we reported that LCR was statistically significantly lower in the group that underwent intestinal resection in patients with strangulated abdominal wall hernia compared to the group that did not. If the LCR score was less than 0.0204, its sensitivity in the diagnosis of strangulated hernia was 80% (58%–92%) and its selectivity was 80.2% (70%–87%). We demonstrated that preoperative low LCR can act as an inflammatory biomarker to predict the need for bowel resection in patients with incarcerated hernias. In addition, LCR coronavirus disease 2019 (COVID-19) has been involved in pandemic studies caused by the new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), it has been reported that LCR can be used as an indicator of systemic inflammation caused by the cytokine storm [22]. The meta-analysis of Lagunas-Rangel et al., In which they looked at six studies, concluded that the decline in LCR may be related to the severity of COVID-19 [18].
In our study, low LCR rates were found to be significant at all postoperative times as an indicator of major complications that may develop in postoperative period. On the postoperative 5th day, we found that the cut-off value of LCR was 0.0034, with 88.8% (71.9–94.8) sensitivity and 85.7% (73.6–95.4) specificity associated with the development of postoperative major complications.
The relationship of postoperative high NLR level in predicting complications after gastrointestinal surgery has been demonstrated in several studies. Cook et al. [23]. Prospectively studied patients who underwent elective colorectal resection. He associated patients with an NLR
The weakness of this study is that it investigated two organ cancer surgeries because of the partial heterogeneity of the patients in the study population. We wanted to show that the LCR level is not specific to a particular organ or type of surgery. Additionally, our study was not designed to compare different surgical techniques. Future studies may compare different surgical techniques (laparoscopic versus open surgery, different anastomosis techniques) and anesthesia methods. The sample size in our study was not large enough. The results of this study can be repeated by obtaining more samples with a multi-center randomized controlled studies. Additionally, most of the previous studies were retrospective studies, and serious complications were likely to be overlooked. The strength of our study is that it is prospective. Therefore, we think that the types of complications and data collection methods are more controlled.
As a result; LCR appears to be a simple, useful and cost-effective biomarker for major abdominal oncologic post-surgical complications such as gastric and colorectal cancer. Although its place in routine clinical practice is not yet established, it can provide physicians with a good tool to identify high-risk surgery patients. To our knowledge, this is the first study of LCR to classify postoperative complications by degree. This study demonstrates that postoperative low LCR is an independent predictor of major surgical complications. In the coming years, we think that the identification and clinical application of predictive biomarkers will become routine to support and improve existing risk assessment procedures.
Funding
This research received no grant from any funding agency in the public, commercial or not-for-profit organisations.
Authors contributions
Conception: MY.
Interpretation or analysis of data: MY., BK
Preparation of the manuscript: MY.
Revision for important intellectual content: MY., BK
Supervision: MY.
Footnotes
Conflict of interest
The authors declare that they have no competing interests.