Effective biomarkers for prediction of recurrence of lung adenocarcinoma cancer (LADC) patients are needed to determine treatment strategies post-surgery to improve outcome.
OBJECTIVE:
This study evaluates the efficacy of carboxypeptidase E (CPE) mRNA including its splice isoforms, CPE-N, as a biomarker for predicting recurrence in adenocarcinoma patients.
METHODS:
RNA was extracted from resected tumors from 86 patients with different stages of non-small cell LADC. cDNA was synthesized and qRT-PCR carried out to determine the copy numbers of CPE/CPE-N mRNA. Patients were followed for 7 years post-tumor resection to determine recurrence and death.
RESULTS:
ROC curve analysis showed the overall AUC for CPE/CPE-N copy number was 0.563 in predicting recurrence and 0.562 in predicting death. Kaplan-Meier survival analysis showed statistical difference ( 0.018), indicating that patients with high CPE/CPE-N copy numbers had a shorter time of disease-free survival and also shorter time to death ( 0.035). Subgroup analyses showed that association of disease-free survival time with CPE/CPE-N copy number was stronger among stage I and II LADC patients ( 0.047).
CONCLUSIONS:
CPE/CPE-N mRNA is a potentially useful biomarker for predicting recurrence and death in LADC patients, especially in identifying patients at high risk of recurrence at early stages I and II.
Lung cancer is the leading cause of cancer death in both men and women, worldwide. In the United States, lung cancer currently accounts for 24% of cancer deaths and is on the rise [1]. According to the American Cancer Society’s estimates in USA, there will be about 235,760 (119,100 in men and 116,660 in women) new cases of lung cancer diagnosed in 2021 and 131,880 deaths, with the risk being much higher for smokers than non-smokers [2]. Lung cancer has been characterized into two main groups: small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC), each accounting for 13% and 84% respectively. NSCLC consists of three main subtypes based on histology: adenocarcinoma, squamous cell carcinoma and large cell carcinoma [3]. Depending on the stage of the disease, various types of treatments have been used. For lung adenocarcinoma (LADC), the most common is surgery followed by tyrosine kinase inhibitors (TKIs) target therapy and radiation therapy. Despite successful treatments, especially with improved drugs for TKIs therapy, some LADCs will recur, either locally, or as distant metastasis, which is the major cause of mortality [4]. Thus, identification of additional biological markers than epidermal growth factor receptor (EGFR) mutations that could predict future recurrence of the tumor is of extreme importance, as that will prompt more vigilant follow-up of high risk patients for early detection of recurrence which will improve outcome and survival.
Carboxypeptidase E (WT-CPE) and a 40 kD N-terminal truncated splice variant of CPE, (CPE-N, Accession # MT035840) are expressed in human cancer cells and have been reported to be a good prognostic biomarker for hepatocellular carcinoma (HCC) [5, 6], colorectal cancer [7], glioblastoma [8], and cervical cancer [9]. A study of 95 LADC patients showed that expression of CPE-N protein, a N-terminal truncated form of CPE, was specifically in the tumor and not in the pericarcinoma, and was associated with poor prognosis [10].
CPE was originally discovered as a prohormone processing enzyme and is expressed in endocrine organs and brain [11, 12], and thus its expression in endocrine and neuroendocrine tumors is not surprising. In cancer cell lines, overexpression of wild-type (WT) CPE has been demonstrated to enhance proliferation in a colorectal cancer cell line [13], and glioma cell lines [8]. Additionally, experiments where recombinant WT-CPE has been added to the culture media of HCC cells under hypoxic conditions have demonstrated that it functions as a survival factor through activating the ERK signaling pathway and enhancement of expression of the mitochondria pro-survival protein, BCL2 [14]. Secreted WT-CPE in media of glioblastoma cell lines [8] or addition of recombinant WT-CPE exogenously to, fibrosarcoma (HT1080) cells showed no effect on promoting cell migration or invasion [14]. However, N-terminal truncated forms of CPE, (CPE-N), when transfected into a HCC cell line [5], Panc-1 cells [15] and osteosarcoma Saos-2 cells [16], promoted migration and invasion, as well as proliferation. Treatment of various cancer cell lines, including those derived from pancreas [17], and osteosarcoma [18] with CPE siRNA that suppresses expression of both CPE-N and WT-CPE mRNA indiscriminately, inhibited proliferation and invasion. Thus loss-of-function and gain-of-function studies indicate that CPE promotes cell proliferation, migration and invasion to drive tumor growth and metastasis in different cancer types.
Quantitative RT-PCR, mRNA expression profiling and immunostaining studies have detected CPE expression in SCLC [19, 20] and NSCLC [21], including a subclass of LADC [22], although the exact form(s) of CPE mRNA and protein present in those tumors were not characterized. Here, we have evaluated whether CPE/CPE-N mRNA could serve as a biomarker for predicting recurrence and survival in LADC patients. We have analyzed a cohort of 86 LADC patients and determined the levels of CPE/CPE-N mRNA in the resected tumors. Our results indicate that high levels of CPE/CPE-N mRNA in LADC are significantly associated with recurrence and poor survival of patients at all stages of the disease.
Materials and methods
Study participants
All 145 patients gave their written informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki and the protocol was approved by the Ethics Committees. The lung adenocarcinoma (LADC) samples were collected under National Cheng Kung University (NCKU) IRB approved protocol BR-100-038. All these non-small cell LADC patients underwent surgical resection of the adenocarcinomas at NCKU hospital between 2003–2009. The patients had not been treated prior to tumor resection and did not receive postsurgery treatment. Clinical information was collected on age, sex, and tobacco smoking (Table S1). The tumor histological grading and staging were determined according to the 6 edition American Joint Committee on Cancer Staging Manual (Table S1). The subjects included patients with all stages of the disease and they were followed up ranging from 1 month to more than 7 years. The end of the follow-up period was April 2014 with the median follow-up of 47.8 months. Of the 145 participants recruited and followed up, 14 of the tumors did not have reliable CPE copy number measurements due to poor RNA quality, leaving the analysis sample size as 131 subjects. Of these 131 subjects, 45 samples did not have 18S RNA determination due to sample shortage, but the CPE copy numbers were within the range. Analyses were carried out, using the 86 samples that were normalized to 18S RNA. All tumor tissues had tumor % 60%. Individual covariates and outcome post-surgery (survival and tumor recurrence) were extracted from electronic medical records including age, gender, smoking (yes/no) and cancer stage.
Determination of CPE/CPE-N mRNA in resected lung tumors
Total RNA was extracted using TRIzol reagent (Invitrogen), and cDNA was made using a High Capacity cDNA Reverse Transcription Kit (Applied Biosystems). Real-time quantitative PCR (qPCR) were performed using an ABI PRISM 7500 Sequence Detector (Applied Biosystems) to determine CPE mRNA expression with a Fast SYBRxGreen Master Mix PCR kit (Applied Biosystems). Fluorescence signals were analyzed using SDS 1.9.1 software (Applied Biosystems). The primers for hCPE were Fwd: 5-ATGGCCGGGCATGAGGCG GC 3 and Rev: 5-GCTGCGCCCCACCGTGTAAA 3 [6] and 18S Fwd: 5-CTCTTAGCTGAGTGTCCC GC-3 and Rev: 5-CTGATCGTCTTCGAACCTCC-3 [6]. CPE/CPE-N mRNA copy numbers were determined by a standard curve method using known concentrations of a cDNA fragment containing hCPE 386-2460 nt as standard template. The copy numbers were then normalized to 18S RNA.
Since both WT-CPE and CPE-N promote tumorigenesis, we used primers which can cross prime both WT-CPE and CPE-N transcripts. We then characterized the CPE transcripts expressed in ten randomly selected adenocarcinomas in this study using agarose gels. Two forms of CPE-N mRNA and no WT-CPE mRNA was detected in these tumors (Fig. S1). If these 10 tumors are representative of the cohort, the copy numbers determined by qRT-PCR suggest mainly CPE-N mRNAs in these tumors. CPE-WT mRNA transcripts may be present in the other tumors not analyzed, and hence we refer to the copy numbers as CPE/CPE-N mRNA.
Statistical analysis
The descriptive statistics were tabulated for the analysis sample of 86 subjects. Two end points of interest, recurrence of lung cancer and death due to lung cancer were analyzed separately. We performed the receiver operating characteristic (ROC) analysis (Fig. S2) on the dichotomized recurrence and death status at the end of the study. The prediction accuracy of CPE/CPE-N copy number in continuous scale was evaluated by the ROC curve and its area (AUC) for dichotomized recurrence and death, respectively. To determine the optimal cutoff point of CPE/CPE-N copy number, we calculated the Youden’s index (sensitivity 1 specificity – 1) for three pre-specified thresholds: 10,000, 15,000, and 20,000, (Table S2) and chose the one that maximize the Youden’s index [23]. With the chosen optimal cutoff, the sensitivity, specificity and diagnostic odds ratio (OR) were then calculated for predicting recurrence and death. The analyses were performed in Stata 12.1.
Summary statistics of the study participants ( 86 lung adenocarcinoma patients)
Variable
Label
Summary statistics
Copy number
Median (1st and 3rd quartiles)
31212 (10208, 85280)
Follow-up (months)
Median (1st and 3rd quartiles)
43.5 (29.3, 62.2)
Age (years)
Mean (SD)
59.5 (10.6)
Recurrence
Yes
46 (53.5%)
No
40 (46.5%)
Death
Yes
31 (36.0%)
No
55 (64.0%)
Gender
Female
41 (47.7%)
Male
45 (52.3%)
Smoking
Yes
32 (37.2%)
No
54 (62.8%)
Cancer stage
I
44 (51.2%)
II
8 (9.3%)
III
27 (31.4%)
IV
7 (8.1%)
Since the timing of recurrence and death provided additional information about cancer progression, and patients had different lengths of follow-up, we performed survival analyses examining the association between CPE/CPE-N copy number and time to recurrence and death, respectively. For the time to recurrence analysis, patients who did not recur by the end of the follow-up were treated as “right censored”, i.e., their potential recurrence date would be after the end of the follow-up time. A total of 9 patients had died of lung cancer without documented recurrence date, and were “left censored”, i.e., their recurrence happened before their date of death. Kaplan-Meier curves for left and right censored data were estimated by nonparametric maximum likelihood estimation [24], implemented in R library (interval). Two Kaplan-Meier curves were plotted for subjects with high and low CPE/CPE-N copy numbers, and a permutation-based log rank test [24] was used to detect the difference between the two curves. In the time to death analysis, only right censoring occurred, and the estimation of Kaplan-Meier curves and log rank test were performed in R library (survival). Additional Kaplan-Meier plots were provided in the supplementary materials (Figs S3, S4) examining the association of time to recurrence and death in relation to individual covariates, such as age, gender, smoking and cancer stage. In order to explore the subgroups in which CPE/CPE-N copy number has a stronger association with time to recurrence and death, we repeated the survival analysis in stratified sample by individual covariates. A pre-specified significance level of 0.05 was used in this study.
Results
Characteristics of patient samples and expression of CPE/CPE-N mRNA in lung adenocarcinomas
Tumors were resected from patients diagnosed with adenocarcinomas and rapidly frozen. Total RNA was extracted from the resected adenocarcinomas and assayed for copy numbers of CPE/CPE-N mRNA by q-RT-PCR as described in methods. The copy numbers of CPE/CPE-N mRNA were then analyzed with respect to the pathological disease stage, gender, age, smoking status, tumor recurrence and death of the patients. Table 1 shows the characteristics of the analysis sample for the 86 lung adenocarcinoma (LADC) patients. The patients had an average age of 59.5 years, 41 (47.7.0%) were female, 54 (62.8%) were non-smokers, and 44 (51.2%) had stage I lung cancer. A total of 46 (53.5%) of the patients had recurrence, and 31 (36.0%) eventually died. The median CPE/CPE-N copy number was 31212. Kaplan-Meier plots (Figs S3, S4) examining the association of time to recurrence and death in relation to individual covariates, such as age, gender, smoking and cancer stage indicated a significant difference in stage but not age, gender or smoking.
CPE/CPE-N expression predicts recurrence and death in lung adenocarcinoma patients
ROC curve analysis of CPE/CPE-N copy numbers in resected adenocarcinoma tissue was carried out to predict recurrence and death in patients. The Youden’s index for CPE/CPE-N copy number at a cutoff of 10,000 is better for predicting both recurrence and death (Table S1). Therefore, we chose to dichotomize the copy number at 10,000 for the subsequent analyses, resulting in 19 LADC subjects with low copy number and 65 with high copy number. The overall AUC for CPE/CPE-N copy number is 0.563 in predicting recurrence and 0.562 in predicting death (Table 2). The diagnostic OR (Table 2) is significant for recurrence (OR: 3.00, 95% confidence interval [CI]: 1.07–8.44), and for death (OR: 4.54, 95% CI: 1.22–16.95).
Sensitivity, specificity, diagnostic odds ratio, and area under ROC curve (AUC) for CPE/CPE-N copy number in predicting recurrence and death
Sens (%)
Spec (%)
OR (95% CI)
AUC
Recurrence
84.8
35.0
3.00 (1.07, 8.44)
0.563
Death
90.3
32.7
4.54 (1.22, 16.95)
0.562
Cutoff for CPE copy number is 10,000.
Association between expression of CPE/CPE-N mRNA in lung adenocarcinoma tissue and survival
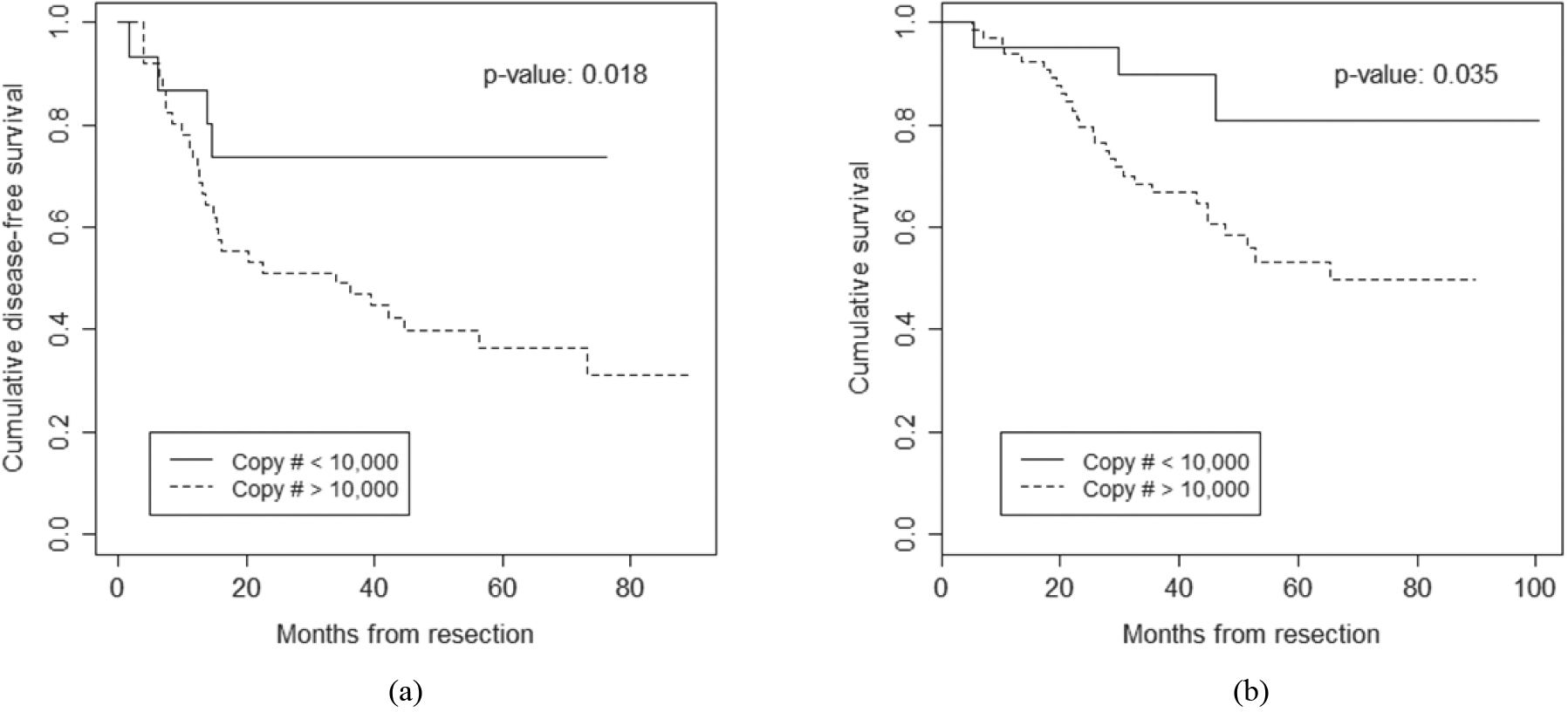
The association between tumor CPE/CPE-N mRNA expression and survival of the 86 LADC patients were analyzed with Kaplan-Meier survival analysis. Figure 1a shows the survival curves of time-to-recurrence for patients with high and low copy numbers. The difference is statistically significant (-value: 0.018), indicating that LADC patients with high CPE/CPE-N copy number had a shorter time of disease-free survival. Similarly, Fig. 1b shows that patients with high CPE/CPE-N copy numbers also had a significantly shorter time to death with a p-value of 0.035.
Subgroup analysis for time to recurrence and time to death
Stratification variable
Label
-value for recurrence
-value for death
Stage
I and II
0.047
0.138
III and IV
0.519
0.337
Smoking
Yes
0.452
0.763
No
0.024
0.011
Age
60
0.073
0.067
60
0.117
0.308
Gender
Female
0.033
0.020
Male
0.198
0.435
Testing if copy number predicts time to recurrence among stratified groups using permutation-based log rank test. Testing if copy number predicts time to death among stratified groups using log rank test.
Survival curves by CPE/CPE-N copy number at cutoff 10,000 for (a) time to recurrence and (b) time to death in patients with lung adenocarcinoma.
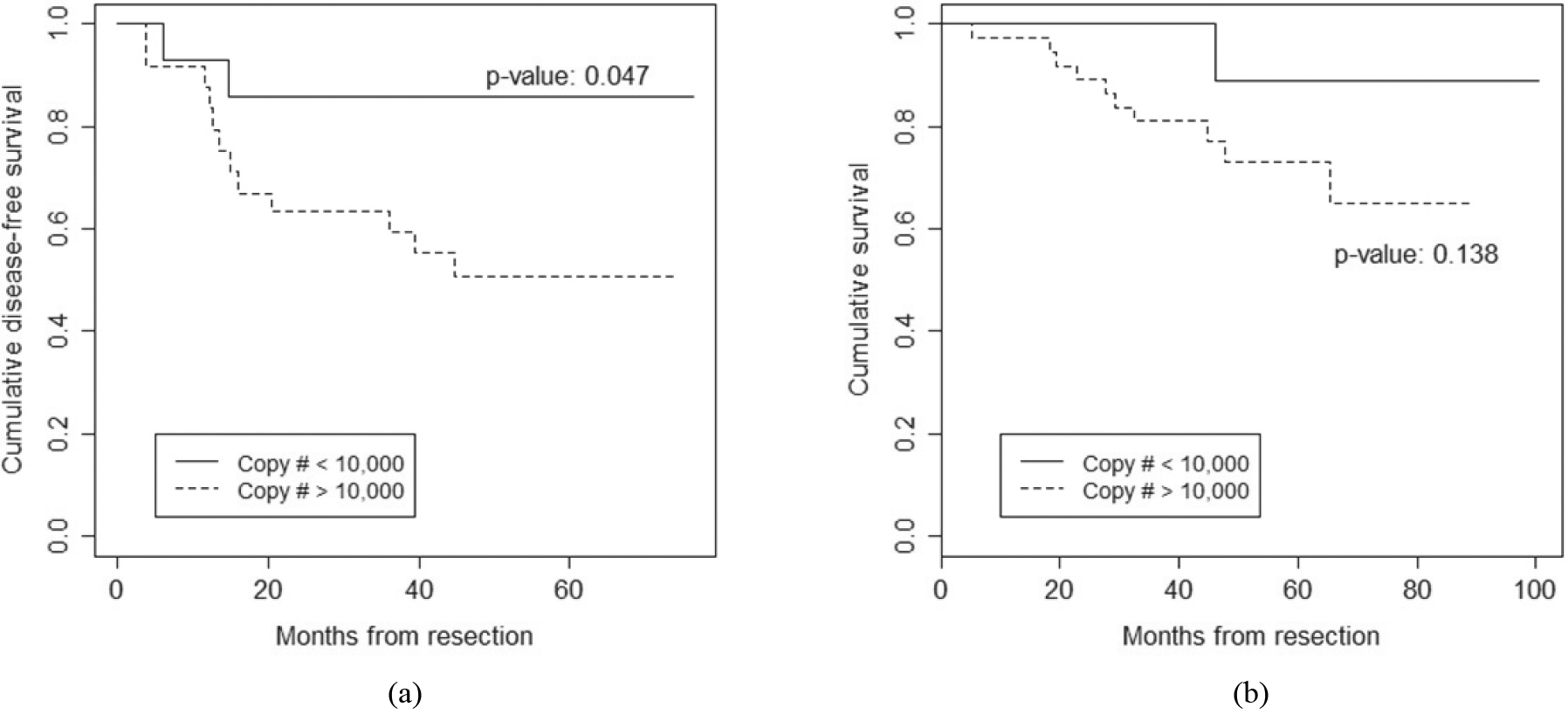
Survival curves by CPE/CPE-N copy number at cutoff 10,000 for (a) time to recurrence and (b) time to death among Stage I and II patients with lung adenocarcinoma.
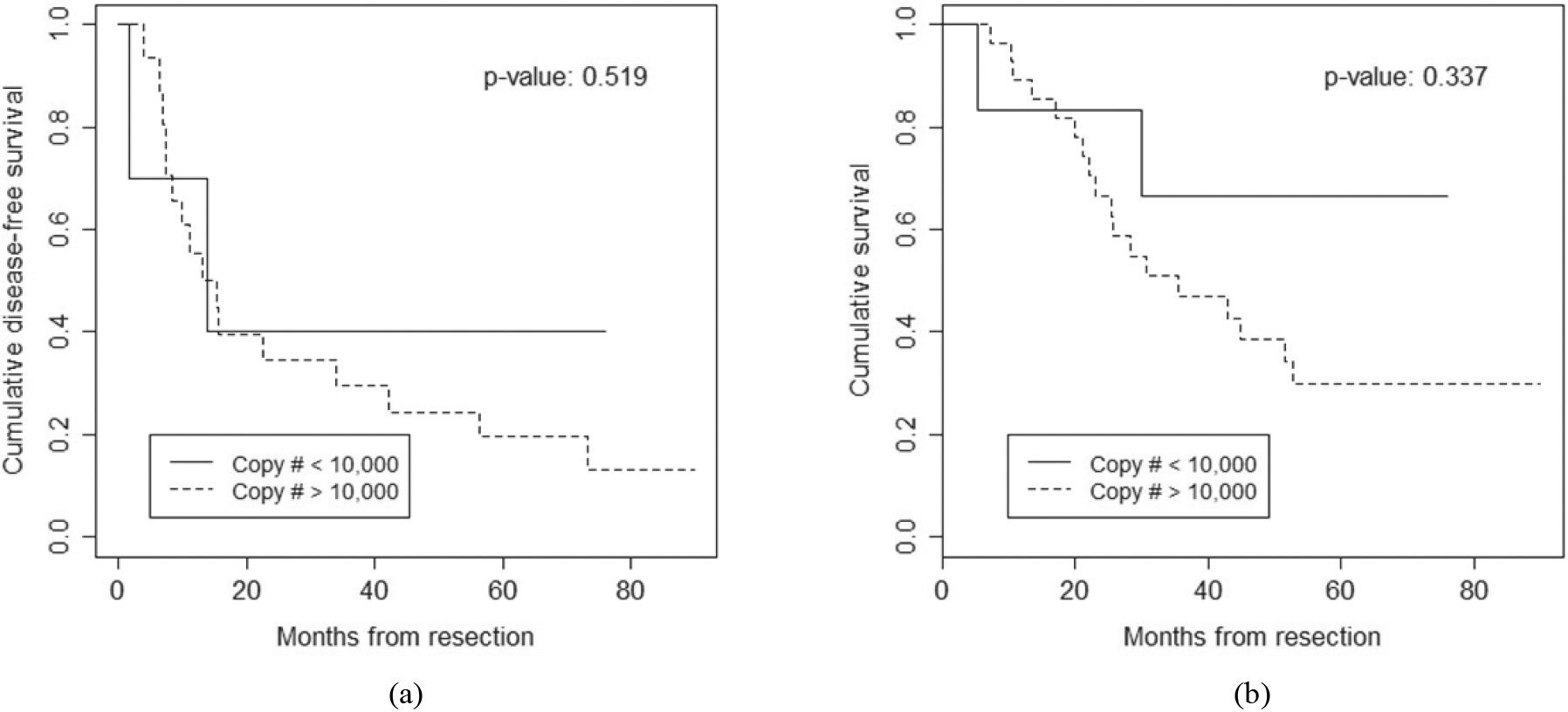
In the subgroup analyses (Table 3 and Fig. 2, Table S3), we found that the association of disease-free survival time with CPE/CPE-N copy number was particularly strong among stage I and II patients with LADC (p-value 0.047 for recurrence) but association with death did not reach significance (-value 0.138). The association with survival did not reach significance for Stage III and IV patients (Table 3 and Fig. 3) due to two possible reasons. First, fewer patients were at Stage III or IV, limiting the statistical power to detect differences. Second, the advanced stage of LADC has poor prognosis, and with most patients having died shortly after surgery, it is difficult for any biomarker to pick out any differences in survival time. CPE/CPE-N copy number was also predictive for recurrence and death among non-smokers (-values: 0.024 and 0.011 respectively) and females (-values 0.033 and 0.020 respectively) (Table 3).
Survival curves by CPE/CPE-N copy number at cutoff 10,000 for (a) time to recurrence and (b) time to death among Stage III and IV patients with lung adenocarcinoma.
Discussion
Our previous study quantifying CPE/CPE-N mRNA levels by qRT-PCR in primary HCC tumors (T), versus surrounding tissue (N) revealed that a ratio of T/N 2 predicted future development of recurrence [6]. In another large study of 219 colorectal cancer patients, high levels of CPE-N mRNA expression were closely correlated with tumor differentiation, recurrence and lymph node metastasis [7]. More recently, it has been reported that overexpression of CPE/CPE-N protein detected both in the nuclei and cytoplasm is correlated with pelvic lymph node metastasis and poor prognosis in patients with early-stage cervical cancer [9]. These clinical studies indicated that CPE/CPE-N is a potentially powerful prognostic biomarker for predicting recurrence and metastasis in many cancer types. Here, we have evaluated whether CPE/CPE-N mRNA, could be a useful prognostic biomarker for predicting recurrence and death in lung adenocarcinoma patients. In this study, we showed that in NSCLC of the adenocarcinoma subtype, high levels of CPE/CPE-N mRNA expression predicted recurrence and death in these patients. This is consistent with a mRNA expression profiling study which revealed that high CPE mRNA expression in a subclass of lung adenocarcinoma indicated poor prognosis [22]. Our study in lung adenocarcinoma patients revealed a sensitivity of 84.8% for CPE/CPE-N mRNA as a biomarker for predicting recurrence, and 90.3% for predicting death. The specificity for this biomarker for predicting recurrence and death was 35.0% and 32.7% respectively. Thus our data indicate that CPE/CPE-N mRNA is a potentially useful prognostic biomarker with high sensitivity for lung adenocarcinoma patients. Our study with up to 7-year follow-up of patients post-operatively corroborates and extends a previous small study done by another group showing that patients with adenocarcinoma expressing CPE-N proteins which included several immunostained bands smaller in size than WT-CPE, versus those without CPE-N expression analyzed by Western blot, had a significantly higher recurrence and metastasis rate over a 3 year follow-up period post-operatively [10]. Subsequently, the same group demonstrated that immunostaining intensity of nuclear CPE in 195 lung adenocarcinoma clinical samples increased with increasing TNM stage I, II, III, although no other analysis was done [25]. There are no specific antibodies that would cross react with CPE-N specifically and not WT-CPE. Hence the nuclear CPE immunostaining in the those LADC samples likely represents CPE-N since subcellular fractionation followed by Western blot, and transfection studies in the literature on different cancer cell lines have specifically shown localization of CPE-N in both cytoplasm and nucleus, while WT-CPE is only in the cytoplasm [5, 15]. Thus scoring nuclear CPE immunostaining in tissue microarray and paraffin sections for quantifying CPE-N expression, can apparently provide an indication of poor prognosis, if immunostaining of nuclear CPE in the tumor is intense. However, for the purpose of biomarker development, our study using a CPE/CPE-N mRNA PCR assay provides a more quantitative high throughput measurement than immunohistochemistry. The combination of both the CPE/CPE-N mRNA PCR assay and scoring of nuclear CPE immunostaining intensity could render CPE a very useful biomarker for predicting recurrence, metastasis and death in LADC.
In our analysis of the time to recurrence, one of the most important findings of this study is that high CPE/CPE-N mRNA copy numbers ( 10000) predicted recurrence in the cohort of patients with stage I and II adenocarcinoma, with most recurrence within 20 months after resection (Fig. 1a, 2). Currently, there are no good prognostic biomarker that could identify high risk stage I and II lung adenocarcinoma patients. Thus, CPE/CPE-N mRNA is potentially a useful molecular biomarker with high sensitivity for early diagnosis of high risk patients who would rapidly develop recurrence, even though the histopathology of their tumor based on staging (I and II) would have indicated good prognosis. Such knowledge would help prompt more frequent follow up for these high risk patients and determine the strategies for treatment post-surgery that would improve outcome. There are a number of molecular biomarkers for NSCLC using microarray and proteomics technology to identify genetic mutations (for review see [26]. These include K-ras, p53, EGFR [27, 28, 29]; hypermethylation of genes (e.g. aberrant p16 methylation) [30]; or increased or decreased expression of proteins (e.g. hsp70 and Rab37, CYP3A4 and CYP3A5) [31, 32] that characterizes aggressive tumors and poor prognosis, but they do not predict recurrence of Stage I or Stage II patients. Additionally, serum/plasma biomarkers for NSCLC have also been reported such as GM2-activator protein [33], plasma D-dimer [34] and mRNA-21 [35]. Bioinformatic analyses of databases have identified IncRNAs as potential predictive biomarkers of lung adenocarcinoma [36]. As well, circulating microRNAs and circRNA, free or in exososomes, ctDNA and circulating tumor cells are emerging as possible biomarkers in diagnosis and quantification of lung cancer burden [37, 38]. However, none of these potential biomarkers have been translated to clinical use yet. As commonly seen in biomarker research, one biomarker alone may not produce high enough prediction accuracy; therefore, larger-scale future research is warranted in combining CPE/CPE-N mRNA and protein with other existing and novel biomarkers, as well as other risk factors, to improve the risk prediction model of adenocarcinoma recurrence and death.
Subgroup analysis showed another interesting finding in that females with high copy numbers of CPE/CPE-N mRNA were associated with higher recurrence and death. Furthermore, non-smokers that have copy numbers of CPE/CPE-N above the cutoff of 10,000 were also highly associated with recurrence and death. The correlation may be due in part to the fact that the female lung cancer patients were mostly non-smoking patients in our recruited Asian patient cohort. We should emphasize that the subgroup analyses were based on relatively small sample size, and mostly exploratory and hypotheses-generating. Larger studies are needed to replicate and to confirm these findings, so that they could be translated into the population level. Nevertheless, these findings motivate further investigations into the relationship between CPE/CPE-N mRNA and cancer progression among women, non-smokers and early and late stage patients with lung adenocarcinoma.
In conclusion, we have provided evidence that CPE/CPE-N mRNA is a potential candidate biomar-ker for predicting recurrence and death in lung adenocarcinoma patients, and is especially clinically useful for identifying high risk patients very early when the disease is at stage I and II. Moreover, non-smokers are also at high risk of recurrence and death when the CPE/CPE-N mRNA levels are high. Of particular significance is that this study has set the stage for future large scale exploration to confirm the potential utility of CPE/CPE-N mRNA as a biomarker to select early stage lung adenocarcinoma patients for adjuvant chemotherapy or extended adjuvant therapy post surgery.
Author contributions
Conception: YPL, Y-CW.
Interpretation or analysis of data: I-YK, DL, W-WL, YPL, Y-CW.
Preparation of the mauscript: I-YK, DL, YPL, Y-CW.
Revision for important intellectual content: I-YK, DL, YPL, Y-CW.
Supervision: YPL, Y-CW.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/CBM-210206.
sj-docx-1-cbm-10.3233_CBM-210206.docx - Supplemental material
This research was supported by the Taiwan Ministry and Science Technology (#102-2627-B-006-010) and the Intramural Research Program of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), National Institutes of Health, USA. We thank Drs. S. Murthy and N. Cawley (NICHD) for their help in data processing.
Conflict of interest
The authors declare no conflict of interest.
References
1.
SiegelR.L.MillerK.D. and JemalA., Cancer statistics, 2019, CA Cancer J Clin69 (2019), 7–34.
2.
American Cancer Society link: https://www.cancer.org/cancer/lung-cancer/about/key-statistics.html.
3.
PikorL.A. et al., Genetic alterations defining NSCLC subtypes and their therapeutic implications, Lung Cancer82 (2013), 179–189.
4.
SiJ. et al., Shisa3 brakes resistance to EGFR-TKIs in lung adenocarcinoma by suppressing cancer stem cell properties, J Exp Clin Cancer Res38 (2019), 481.
5.
YangX. et al., A novel 40kDa N-terminal truncated carboxypeptidase E splice variant: cloning, cDNA sequence analysis and role in regulation of metastatic genes in human cancers, Genes Cancer10 (2019), 160–170.
6.
HuangS.F. et al., Carboxypeptidase E is a prediction marker for tumor recurrence in early-stage hepatocellular carcinoma, Tumour Biol37 (2016), 9745–9753.
7.
ZhouK. et al., Overexpression of CPE-DeltaN predicts poor prognosis in colorectal cancer patients, Tumour Biol34 (2013), 3691–3699.
8.
HoringE. et al., The “go or grow” potential of gliomas is linked to the neuropeptide processing enzyme carboxypeptidase E and mediated by metabolic stress, Acta Neuropathol124 (2012), 83–97.
9.
ShenH.W. et al., CPE overexpression is correlated with pelvic lymph node metastasis and poor prognosis in patients with early-stage cervical cancer, Arch Gynecol Obstet294 (2016), 333–342.
10.
SunJ. et al., N-terminal truncated carboxypeptidase E expression is associated with poor prognosis of lung adenocarcinoma, Oncol Lett12 (2016), 4659–4664.
11.
FrickerL.D., Carboxypeptidase E, Annu Rev Physiol50 (1988), 309–321.
12.
HookV.Y. and LohY.P., Carboxypeptidase B-like converting enzyme activity in secretory granules of rat pituitary, Proc Natl Acad Sci USA81 (1984), 2776–2780.
13.
LiangX.H. et al., Upregulation of CPE promotes cell proliferation and tumorigenicity in colorectal cancer, BMC Cancer13 (2013), 412.
14.
MurthyS.R. et al., Carboxypeptidase E promotes cancer cell survival, but inhibits migration and invasion, Cancer letters341 (2013), 204–213.
15.
HareendranS. et al., Carboxypeptidase E-N Promotes Proliferation and Invasion of Pancreatic Cancer Cells via Upregulation of CXCR2 Gene Expression, Int J Mol Sci20 (2019), 5725.
16.
FanS. et al., Carboxypeptidase E-DeltaN promotes migration, invasion and epithelial-mesenchymal transition of human osteosarcoma cell lines through the Wnt/beta-catenin pathway, Biochem Cell Biol97(4) (2019), 446–453.
17.
LiuA. et al., Downregulation of CPE regulates cell proliferation and chemosensitivity in pancreatic cancer, Tumour Biol35 (2014), 12459–12465.
18.
FanS. et al., Silencing of carboxypeptidase E inhibits cell proliferation, tumorigenicity, and metastasis of osteosarcoma cells, Onco Targets Ther9 (2016), 2795–2803.
19.
HeP. et al., Identification of carboxypeptidase E and gamma-glutamyl hydrolase as biomarkers for pulmonary neuroendocrine tumors by cDNA microarray, Hum Pathol35 (2004), 1196–1209.
20.
NorthW.G. and DuJ., Key peptide processing enzymes are expressed by a variant form of small-cell carcinoma of the lung, Peptides19 (1998), 1743–1747.
21.
KrajnikM. et al., Enkephalin, its precursor, processing enzymes, and receptor as part of a local opioid network throughout the respiratory system of lung cancer patients, Hum Pathol41 (2010), 632–642.
22.
BhattacharjeeA. et al., Classification of human lung carcinomas by mRNA expression profiling reveals distinct adenocarcinoma subclasses, Proc Natl Acad Sci U S A98 (2001), 13790–13795.
23.
GreinerM.PfeifferD. and SmithR.D., Principles and practical application of the receiver-operating characteristic analysis for diagnostic tests, Prev Vet Med45 (2000), 23–41.
24.
FayM.P. and ShawP.A., Exact and Asymptotic Weighted Logrank Tests for Interval Censored Data: The interval R package, Journal of Statistical Software36(2) (2010), i02.
25.
SunJ. et al., N-terminal truncated carboxypeptidase E represses E-cadherin expression in lung cancer by stabilizing the Snail-HDAC complex, Am J Cancer Res10 (2020), 925–938.
26.
SearsC.R. and MazzoneP.J., Biomarkers in Lung Cancer, Clin Chest Med41 (2020), 115–127.
27.
VanMeterA.J. et al., Laser capture microdissection and protein microarray analysis of human non-small cell lung cancer: differential epidermal growth factor receptor (EGPR) phosphorylation events associated with mutated EGFR compared with wild type, Mol Cell Proteomics7 (2008), 1902–1924.
28.
SchneiderP.M. et al., Multiple molecular marker testing (p53, C-Ki-ras, c-erbB-2) improves estimation of prognosis in potentially curative resected non-small cell lung cancer, Br J Cancer83 (2000), 473–479.
29.
HerbstR.S. et al., Lung cancer, N Engl J Med359 (2008), 1367–1380.
30.
YangY.C. et al., DNMT3B overexpression by deregulation of FOXO3a-mediated transcription repression and MDM2 overexpression in lung cancer, J Thorac Oncol9 (2014), 1305–1315.
31.
QixingM. et al., The expression levels of CYP3A4 and CYP3A5 serve as potential prognostic biomarkers in lung adenocarcinoma, Tumour Biol39 (2017), 1010428317698340.
32.
TsaiC.H. et al., Small GTPase Rab37 targets tissue inhibitor of metalloproteinase 1 for exocytosis and thus suppresses tumour metastasis, Nat Commun5 (2014), 4804.
33.
PotprommaneeL. et al., GM2-activator protein: a new biomarker for lung cancer, J Thorac Oncol10 (2015), 102–109.
34.
WangY. and WangZ., Predictive value of plasma D-dimer levels in patients with advanced non-small-cell lung cancer, Onco Targets Ther8 (2015), 805–808.
35.
TangD. et al., Identification of plasma microRNAs as novel noninvasive biomarkers for early detection of lung cancer, Eur J Cancer Prev22 (2013), 540–548.
36.
JinD. et al., Identification of Three lncRNAs as Potential Predictive Biomarkers of Lung Adenocarcinoma, Biomed Res Int2020 (2020), 7573689.
37.
Blandin KnightS. et al., Progress and prospects of early detection in lung cancer, Open Biol7 (2017), 170070.
38.
Pedraz-ValduncielC. and RosellR., Defining the landscape of circRNAs in non-small cell lung cancer and their potential as liquid biopsy biomarkers: A complete review including current methods, Extracell Vesicles Circ Nucleic Acids2 (2021), 179–201.