
Abstract
BACKGROUND:
Patients with microsatellite instability-high (MSI-H) colorectal cancer (CRC) generally have a better prognosis and a more effective immune response than patients with microsatellite stable (MSS) CRC. Moreover, activated platelets play a crucial role in modulating innate immune cells. Mean platelet volume (MPV) is an indicator of platelet activation. This study is to examine the association between MPV and MSI status in CRC.
METHODS:
We collected the clinical and pathological variables of 424 CRC patients diagnosed at the Harbin Medical University Cancer Hospital from January 2018 to December 2018. Associations between MPV levels and MSI status were examined. Propensity score matching (PSM) was performed to reduce the possibility of selection bias.
RESULTS:
424 CRC patients were divided into low-MPV group and high-MPV group according to the optimal cut-off value of MPV. 131 high-MPV patients were matched to low-MPV counterparts in a 1:1 ratio by propensity score matching. As MPV levels increased, the percentage of patients with MSI-H reduced. Furthermore, compared with MSS group, the MSI-H group had a significantly lower MPV levels (
CONCLUSION:
Lower MPV is associated with MSI-H subtype of CRC. Further study on MPV in MSI-H CRC is warranted.

Introduction
Colorectal cancer (CRC) was the third most diagnosed form of cancer and the fourth leading cause of cancer-related deaths globally [1]. So far, there are still no effective methods to treat advanced and metastatic CRC because of unavoidable drug tolerance [2]. Approximately 15% of CRC develop through the microsatellite instability (MSI) pathway [3]. MSI is caused by the accumulation of frameshift mutations in target gene due to a failure of the mismatch repair system [4]. MSI CRCs had increased lymphocytic infiltration, pronounced peritumoral lymphoid reaction, poorer response to chemotherapeutic drugs, and highly upregulated expression of various immunological checkpoints molecules [5].
Platelet has an essential role in cancer progression and metastasis [6]. Platelets-tumor cell interactions and stimulated signaling pathways have been identified as fundamental determinants of cancer metastasis [7, 8]. There is plenty of evidence to suggest that increased platelets are associated with a poor prognosis in various types of cancer, such as pancreatic cancer, gastric cancer, colorectal cancer, endometrial cancer, and ovarian cancer [9, 10, 11, 12, 13]. Mean platelet volume (MPV) is an index of activated platelets and is linked to different inflammatory conditions in CRC patients [14, 15, 16]. Moreover, altered MPV levels were associated with poor prognosis in CRC [17, 18]. The aim of this study was to investigate the relationship between platelet indices and MSI status in CRC patients.
Methods
Study population
424 CRC patients treated from January 2018 to December 2018 in the Department of Colorectal Medicine, Harbin Medical University Cancer Hospital, were enrolled in this study. The inclusion criteria were as follows: diagnosed with pathologically confirmed CRC, no prior history of chemotherapy or radiotherapy; and had complete laboratory data. The patients with infection, hematological disorders, hypertension, diabetes mellitus, and anti-platelet medication were excluded. The following clinicopathological information was collected from the medical records of patients: age, gender, body mass index (BMI), carcinoembryonic antigen (CEA), smoking status, drinking status, creatinine, white blood cells (WBC), haemoglobin, platelet count, tumor location, tumor size, histological type, histological grade, T classification, lymph node metastasis, and distant metastasis. The TNM stage was classified based on the 8th edition of the American Joint Committee on Cancer (AJCC) cancer staging system.
The Institutional Review Board of Harbin Medical University Cancer Hospital approved this study. Informed consent was submitted by all subjects when they enrolled.
The characteristics of CRC patients according to MPV levels before propensity score matching
The characteristics of CRC patients according to MPV levels before propensity score matching
Data are presented as means (SD) or median (interquartile range) or percentage. BMI, body mass index; CEA, carcinoembryonic antigen; WBC, white blood cells; MPV, mean platelet volume; PDW, platelet distribution width.
A blood sample was obtained after overnight fasting. Routine blood tests were conducted in the hospital’s clinical laboratory. WBC, haemoglobin, and platelet indices were measured by an autoanalyzer (Sysmex XE-2100, Kobe, Japan). The whole blood samples were collected in EDTA-containing tubes, and were processed within 30 minutes after blood collection. The inter- and intra-assays coefficients of variation (CVs) of all these assays were below 5%.
MSI analysis
DNA was obtained from fresh-frozen tumor tissue samples. MSI was assessed using polymerase chain reaction with primers amplifying the microsatellite markers, including BAT25, BAT26, NR-21, NR-24, and NR-27. MSI was graded as high (MSI-H) if at least three markers out of five were unstable, whereas MSS was defined as stable (MSS) if there were less than three unstable markers. There were no samples with only two unstable markers.
Statistical analysis
Continuous variables were presented as means
Results
In total, 424 CRC patients were included for the present analysis. There were 242 (57.1%) men and 182 (42.9%) women. The mean ages were 60.9
The optimal cut-off value of MPV was identified using the ROC curve analysis for MSI-H status. The cut-off value for MPV was 10.7 fL (Fig. 1). CRC patients in this study were divided into 2 groups: patients with MPV
The ROC curve for MPV.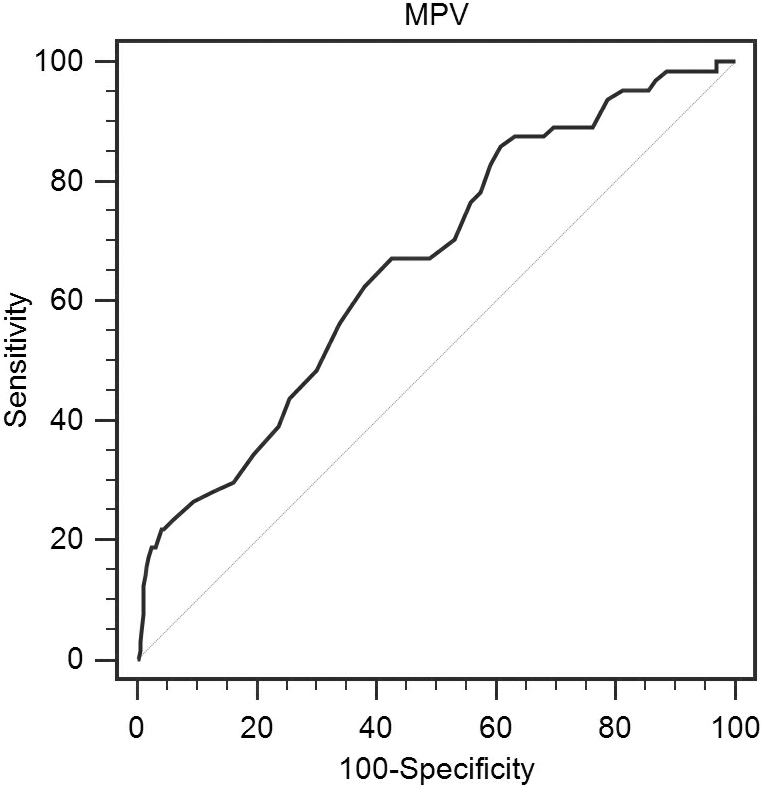
All patients’ characteristics are shown in Table 1. There were significant differences in gender, drinking status, WBC, platelet count, PDW, tumor size, tumor location, mucinous morphology, T classification, lymph node metastasis, clinical stage, and MSI-H status between the two groups. However, age, BMI, smoking status, haemoglobin, CEA, histological grade, and distant metastasis had no difference between the two groups.
After propensity score matching, 131 patients were selected. There were no significant differences in age, gender, BMI, smoking status, drinking status, WBC, haemoglobin, CEA, tumor size, tumor location, histological grade, mucinous morphology, T classification, lymph node metastasis, distant metastasis, and clinical stage between the two groups. However, PDW levels and percentage of MSI-H had significant difference.
The characteristics of CRC patients according to MPV levels after propensity score matching
Table 3 summarizes the clinicopathological characteristics of CRC patients according to MSI status. With regard to age, gender, smoking status, drinking status, CEA, haemoglobin, platelet count, and creatinine levels, there was no difference between the two groups. Higher BMI and PDW levels were found in the MSI-H group than in the MSS group. Moreover, there were significantly positive correlations between MSI-H status and proximal tumor, larger tumor size, mucinous morphology, T classification, distant metastasis, and clinical stage. However, no correlation was observed between MSI-H and lymph node metastasis. WBC, poorly differentiated, lymph node metastasis showed weak correlations. The MPV values in two groups were showed in Fig. 2. Compared to MSS group, MPV levels were significantly reduced in MSI-H group.
Correlations between clinicopathological features and MSI status in CRC after propensity score matching
The MPV values in MSI-H and MSS group.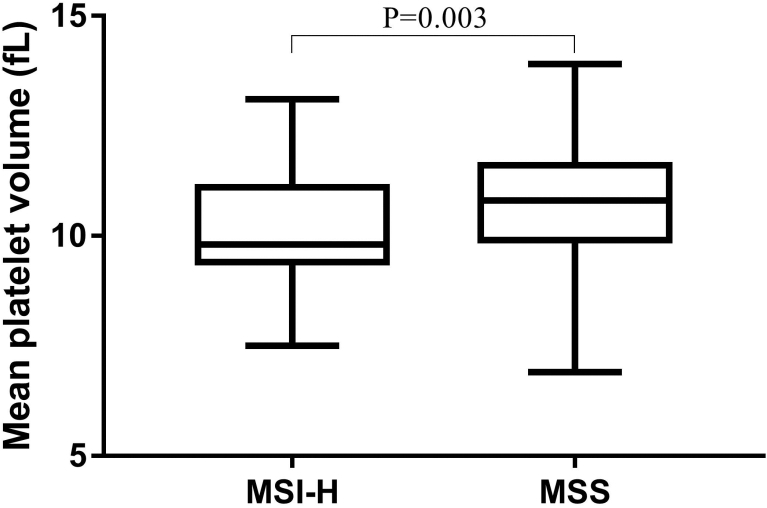
The prevalence of MSI-H was calculated by the quartiles of MPV. The MPV quartiles were quartile 1 (Q1) (
Logistic regression analysis to evaluate the associations between MSI status and clinical factors
The percentages of CRC patients with MSI-H according to quartiles of MPV.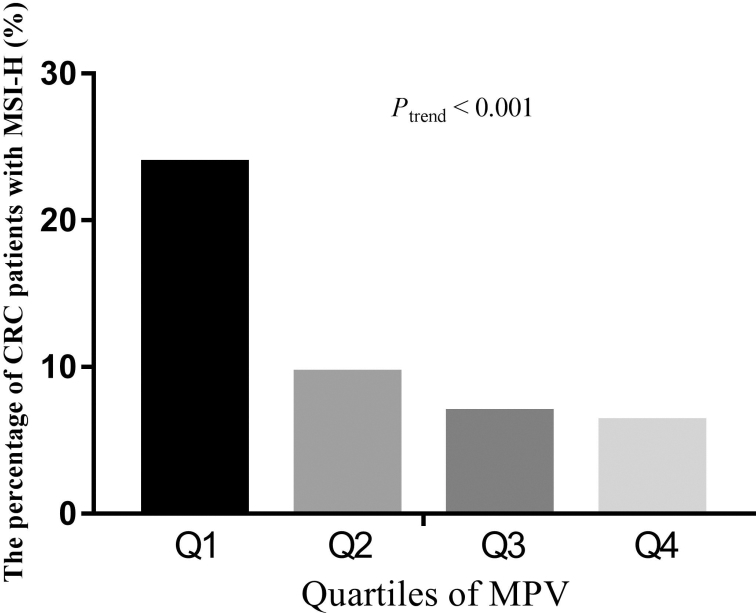
Logistic regression analysis was used to evaluate the risk factors for MSI-H in Table 4. Eleven variables, including BMI, WBC, MPV, PDW, tumor location, tumor size, histological type, histological grade, T classification, lymph node metastasis, and tumor stage were entered into the original model. The results revealed that BMI, WBC, MPV, tumor location, tumor size, and histological grade were significantly associated with MSI-H status after propensity score matching. Notably, MPV was found to be a new risk facor for MSI-H both before propensity score matching and after propensity score matching.
In our study, we found that MPV levels were significantly reduced in MSI-H CRC patients compared with those in MSS patients. In addition, MPV levels were strongly associated with MSI-H status after controlling for potential confounders in the logistic regression analysis.
Platelets in tumor microenvironment play a vital role in tumor development and metastasis [19]. A growing body of evidence supports the association between platelets activation and CRC [20]. Platelet-derived growth factor-D promotes CRC cell migration, invasion and proliferation [21]. Moreover, higher serum platelet-derived growth factor-AA predicts CRC liver metastasis [22]. In addition, platelet-derived endothelial cell growth factor inhibitor augments radiotherapeutic efficacy for CRC [23]. A previous report confirmed that extract of caulis spatholobi, a platelet inhibitor, efficiently suppresses the invasion and metastasis of CRC by targeting tumor cell-induced platelet aggregation [24]. However, these parameters reflecting platelets activation were not routinely measured in clinical practice. MPV is available in routine blood test and does not increase the cost of diagnosis. Furthermore, long-term use of aspirin have a chemo-preventive effect against CRC [25, 26].
The detailed mechanisms of MPV in MSI-H CRC were not well defined. Reduced MPV maybe result from an enhanced consumption of large platelets in inflammatory states [27]. Previous studies revealed that MSI-H status was associated with local and systemic inflammation in CRC [28, 29]. The difference of MPV in different CRC subtypes supports the crucial roles that platelets play on immune cells. Platelet interactions with neutrophils are initially mediated by P-selectin and P-selectin glycoprotein ligand-1, and subsequently interactions with platelet-borne GPIb induce neutrophils to secrete soluble factors and active microparticles, enhancing and facilitating their immune functions [30]. Platelets also synergize with neutrophils to promote monocyte recruitment through heteromers of platelet-derived CCL5 and neutrophil-derived alpha-defensin [31].
In line with our results, previous reports revealed that the CD8 T effector gene signature was markedly upregulated in MSI-H tumors compared with MSS counterpart [32]. Furthermore, CD8(+) cytotoxic T lymphocytes led to enhanced platelet destruction in immune thrombocytopenia [33]. In our study, we confirmed that activated platelets are involved in MSI-H CRC subtypes using a simple indicator of platelet activation. MPV is available in routine blood test and widely used in clinical practice. Thus, elucidating the precise mechanisms of MPV involved in MSI-H CRCs is essential for the development of an effective therapeutic strategy in CRC patients.
There are several limitations to our current study: First, the study was the lack of a mechanistic explanation. Second, the study is carried out in a single center. Third, the findings of this retrospective study from Chinese patients may not be generalizable to other ethnic groups.
In conclusion, lower MPV is associated with MSI-H subtype of CRC. Further study on MPV in MSI-H CRC is warranted.
Footnotes
Acknowledgments
This study was supported by the Fundamental Research Funds for the Provincial Universities (No. 2018-KYYWF-0537).
Conflict of interest
The authors declare that they have no conflicts of interest.
Author contributions
Conception: W W, GY W, RT W, and ZY L
Interpretation or analysis of data: W W, GY W, S F, BB Z, RT W, and ZY L
Preparation of the manuscript: W W and GY W
Revision for important intelectual content: S F, BB Z, ZY L, and RT W
Supervision: ZY L and RT W