
Abstract
BACKGROUND:
Identification of molecular markers that reflect the characteristics of the tumor microenvironment (TME) may be beneficial to predict the prognosis of post-operative hepatocellular carcinoma (HCC) patients.
OBJECTIVE AND METHODS:
A total of 100 tissue samples from HCC patients were separately stained by immunohistochemistry to examine the expression levels of CD56, CD8
RESULTS:
Univariate and multivariate logistic analysis showed that FoxP3 was the independent factor associated with microvascular invasion (MVI), tumor size and envelop invasion; CD68 was associated with envelope invasion and AFP. Kaplan-Meier survival curves revealed that CD68 and FoxP3 expression were significantly associated with relapse free survival (RFS) of HCC patients (
CONCLUSIONS:
Our study indicated that CD68 and FoxP3 are associated with prognosis of HCC patients, and CD68 can be considered as a potential prognostic and predictive biomarker.
Introduction
Hepatocellular carcinoma (HCC), the majority of primary liver cancers (accounting for 75%–85%), is the sixth most common tumor and the fourth leading cause of cancer-related deaths worldwide, with about 841,000 new cases and 782,000 deaths annually [1]. The main risk factors associated with HCC are chronic infections with hepatitis B virus or hepatitis C virus, nonalcoholic fatty liver disease, and alcoholic liver disease [2]. Surgical resection is still the major radical treatment for patients with HCC, however, most patients develop tumor recurrence even metastasis after surgery, which results in poor prognosis and affects long-term survival [3]. It has been reported that the main mechanisms of recurrence include residual micro-lesions, hepatitis, immunosuppression, and microvascular invasion [4]. Therefore, identification of potential molecular markers involved in tumor recurrence could be beneficial to HCC patients.
The tumor microenvironment (TME) plays a vital role in tumor initiation, progression and metastasis, which consists of cancer cells, immune cells, vascular endothelial cells, fibroblasts, secreted cytokines/chemokines and other components [5]. The tumor microenvironment could be divided into immune microenvironment and non-immune microenvironment. TME could be involved in anti-tumor and pro-tumor effect. Natural killer (NK) cells and CD8
A lot of markers have been found to evaluate different types of immune cells. Recent studies showed that the level of active CD56
In this study, we examined the expression of CD56, CD8
Methods and materials
Patients with HCC
From January 2017 to July 2019, a total of 100 HCC patients who underwent tumor resection at Cancer Hospital of Shandong Province were included in this study. HCC was diagnosed according to the NCCN (National Comprehensive Cancer Network) guidelines. Main clinicopathologic information of the patient was summarized in Supplementary Table 1, including MVI, tumor number, satellite nodule, tumor size, envelope invasion, and AFP. AFP levels were determined by immunoenzymatic chemiluminescence (Roche Diagnostics, Germany). Paraffin embedded tissue samples for immunohistochemistry were used in this study. All the clinical tissue specimens were identified by using H&E staining in Department of Pathology. All of the patients were followed-up until June 2020. One patient died of postoperative complications. The clinicopathologic information and tumor tissue of this patient were analyzed, but the patient was excluded in survival analysis.
This study was approved by the medical ethics committee of Cancer Hospital of Shandong Province, and written informed consent was obtained from the participants.
Immunohistochemistry and scoring
Immunohistochemistry was performed on paraffin embedded tissue samples. Tissues were cut into 5
For CD68, FoxP3 and pan-Keratin, the staining intensity and proportion of positive cells were determined. Positive cells had light yellow or brown granules. Staining intensity was determined according to the staining characteristics of most cells (contrast to the background) and was scored as follows: no staining, 0 (None); light yellow, 1 (Weak); brown yellow, 2 (Moderate); brown, 3 (Strong). Five fields were randomly selected at a high magnification (200
Follow-up
Post-surgery follow-up was conducted through hospital-based follow-up visit and/or telephone. All the patients were followed-up until death or June 20, 2020. The postoperative surveillance program complied with a periodical routine follow-up at 3-month intervals for the first 2 years and at 6-month intervals thereafter. Each follow-up visit will include Alpha-fetoprotein (AFP), liver function, enhanced computed tomography (CT), and/or digital subtraction angiography (DSA). If the recurrence was suspicious by the above-mentioned examinations, enhanced magnetic resonance imaging (MRI) will be performed to confirm diagnosis. The recurrence of HCC was diagnosed based on typical imaging findings and/or continually increased serum AFP. Biopsies were undertaken to achieve histopathology or cytopathology evidence but were not necessarily for the assessment of recurrences.
The treatment strategy for recurrence mainly based on the comprehensive consideration of tumor characteristics, liver function and general condition. Local curative treatment consisted of transcatheter arterial chemoembolization (TACE) and radiofrequency ablation (RFA); systemic palliative treatment, such as molecular targeted therapy and chemotherapy was performed as alternative methods for recurrence treatment.
Relapse free survival (RFS) was defined from the date of surgery to the date of detected recurrence or last follow-up.
Survival analysis
Univariate Cox proportional hazards regression analysis were done to evaluate the association of each molecular markers or clinical parameters to overall patient survival. The
Comparisons of baseline immunology characteristics between the groups with different pathological factors
Comparisons of baseline immunology characteristics between the groups with different pathological factors
Variables are expressed as the mean
SPSS26.0 software was used for the statistical analysis. Continuous data were expressed as mean
Results
The association between clinicopathological factors and the six molecular markers in 100 HCC patients
According to the standard of staging system of liver cancer reported by NCCN and Guidelines for diagnosis and treatment of primary liver cancer in China, we just analyzed the main clinical pathological factors, including MVI, tumor number, satellite nodule, tumor size (
Representative immunohistochemical staining images of CD8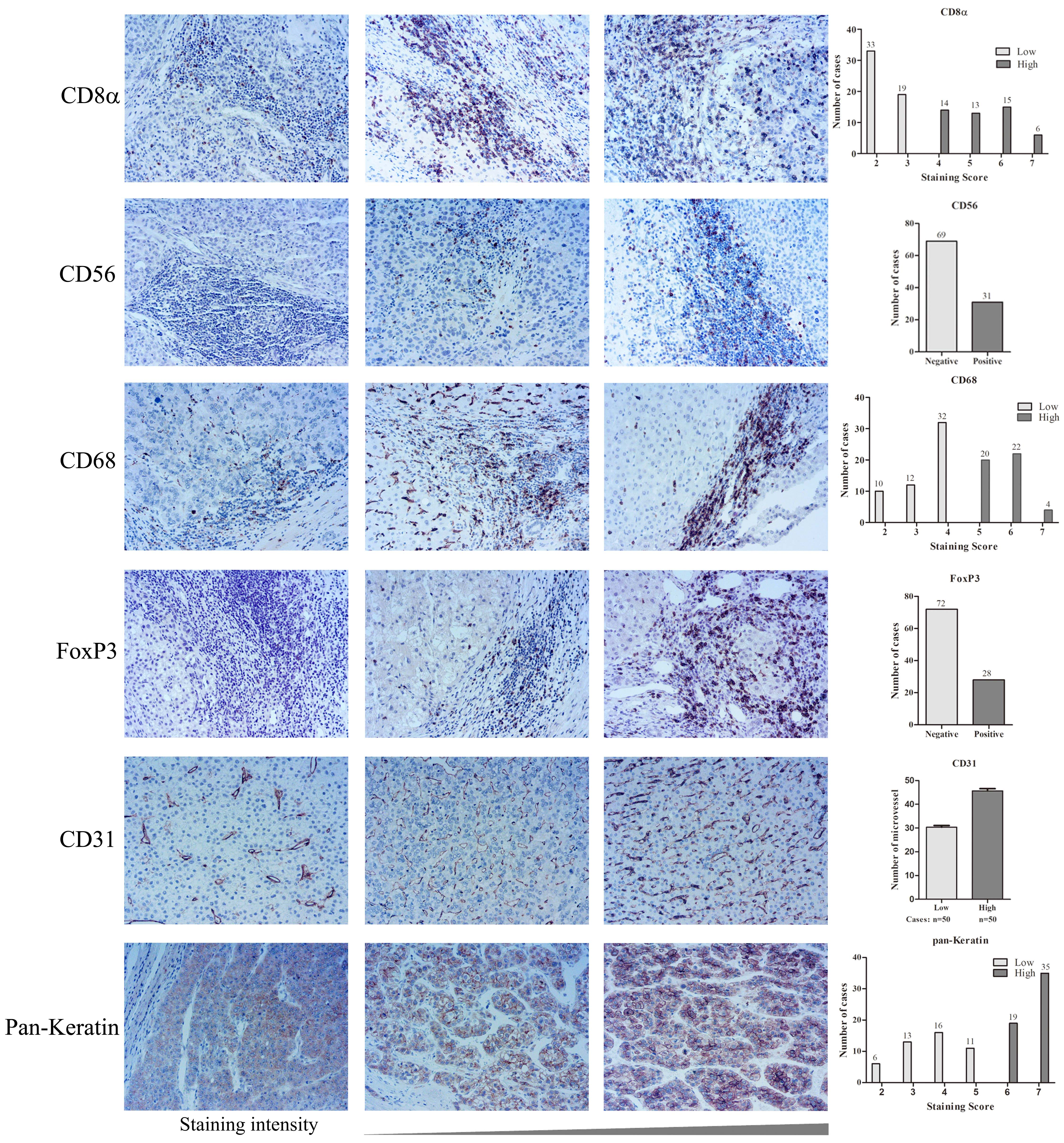
As shown in Table 1, the association between clinicopathological factors and the molecular markers were analyzed. We found that the expression of FoxP3, CD8
Univariate and multivariate logistic analysis of the six markers and pathology characters in 100 HCC patients
HR, hazard ratio; CI, confidence interval.
Univariate and multivariate logistic analysis were performed to further understand the relationship between the molecular markers and clinicopathological factors as shown in Table 2. Univariate analysis showed FoxP3 (HR
In this cohort, recurrence was observed in 55/99 patients (55.6%) in total. The cumulative 1-, 2-, 3-, 4-year RFS rates of the 99 patients were 50.7%, 25.3%, 25.3% and 8.4%, respectively. Among the 55 recurrent patients, 47 had recurrence in the first year. To explore the prognostic values of the six molecular markers and main clinicopathological factors, we used Kaplan-Meier survival curves for relapse free survival (RFS) analysis in this cohort As shown in Fig. 2, our result revealed that CD68 and FoxP3 showed significant relationships with RFS in HCC patients (
Kaplan-Meier curves for RFS in patients with HCC according to the level of CD8
Univariate and multivariate survival analysis of RFS in HCC patients
HR, hazard ratio; CI, confidence interval.
Univariate and multivariate survival analysis were used to analyze the prognostic values of the six markers and clinicopathological factors in HCC patients. As shown in Table 3, the analysis was divided into three sections. Among the clinicopathological factors listed above, univariate analysis revealed that tumor number (HR
Based on the analysis of the two sections above, we included the clinicopathological factors and molecular markers whose
Univariate and multivariate survival analysis of RFS in 28 HCC patients without postoperative TACE
HR, hazard ratio; CI, confidence interval.
Receiver operating characteristic curve analysis for predicting the RFS of HCC patients. ROC curves for the combination of tumor number and MVI, and the combination of tumor number, MVI and CD68, respectively. The sensitivity, specificity and AUC were indicated below the ROC graph.
Additionally, to exclude the influence of postoperative adjuvant therapy on TME, we also did stratification analysis in 28 HCC patients with no postoperative treatment to further identify the prognostic values of the six markers at baseline. As shown in Table 4, the results of univariate analysis showed that only the expression of CD31 (HR
As early recurrence is significantly associated with survival, we wanted to predict early recurrence with those highrisk factors identified above. Multivariate analysis revealed that tumor number, MVI classification and the expression level of CD68 were the independent predictive factor associated with RFS. Then, discriminative power of these three factors in predicting early-recurrence was evaluated by using the ROC curve. As shown in Fig. 3, the ROC curve of the two clinical pathological factors (tumor number and MVI) showed an AUC of 0.788 (85.42% sensitivity and 63.64% specificity). However, the ROC curve of the combination of tumor number, MVI and CD68 showed an AUC of 0.823 (68.75% sensitivity and 86.36% specificity). These results indicated that the combination of clinical pathological factors and the molecular markers was more accurate as a predictive indicator to evaluate the prognosis of HCC patients.
Discussion
The tumor microenvironment, especially the non-cancer cells, significantly influences tumor growth and survival and is closely related to clinical outcomes. To identify the immunologic cellular characteristics of TME may provide new perspective on the treatment of HCC [21]. In the present study, we assessed the expression of CD56, CD8
Forkhead box (Fox) proteins constitute a huge family of transcriptional regulators, and the roles of Fox proteins in tumorigenesis and cancer progression have been intensively studied [22]. A variety of Fox family members can be used as prognostic markers, such as FoxQ1 in breast cancer [23], FoxL1 in osteosarcoma [24, 25] and FoxO1 in epithelial ovarian cancer [26]. FoxP3 has been reported to act as a tumor suppressor in HCC. Shi et al. reported that higher expression of FoxP3 was related to better survival and lower recurrence risk. Moreover, FoxP3 may suppress tumor progression via the TGF-
CD31 is a reliable marker for endothelial cells, which could involve in vascular development and maintain vascular endothelial barrier function [32, 33]. In this study, we found that CD31 expression was associated with MVI presence and RFS in HCC patients without any postoperative adjuvant therapy. Previous study showed that CD31 expression was associated with a poor survival in HCC patients [18], which was consistent with our result. Furthermore, we found that CD8
CD68 is widely accepted as a cell surface marker of macrophage. In this work, we found CD68 expression was an independent risk factor for AFP, and the higher AFP level was associated with shorter RFS in HCC patients. AFP is commonly considered as a prognostic factor of HCC [37]. When the clinicopathological factors and the 6 molecular biomarkers are included in the multivariate analysis, the results showed that CD68 expression was an independent prognostic factors of RFS in HCC patients, which was consistent with the study that reported previously [13]. Moreover, we found that CD56 expression was associated with tumor size. It has been reported that active CD56
The limitation of our work is that we just detected the expression of these markers in the resected tumor tissue but did not follow the subtype of these immune cells. As we known, different subtypes of the immune cells can perform different or even opposite functions. Further studies are required to determine the function of the dominant subtype of the immune cells in HCC.
In summary, our study found that CD68 and FoxP3 showed significant relationships with RFS of HCC patients. Tumor number, MVI classification and the expression level of CD68 were the independent predictive factors associated with RFS. The classifier established by the combination of tumor number, MVI and CD68 was higher than that of just tumor number and MVI. All these suggest that the characteristics of TME are associated with prognosis of HCC patients.
Author contributions
Conception: Mei Liu.
Interpretation or analysis of data: Liming Wang.
Preparation of the manuscript: Shuwen Kuang, Mei Liu, Liming Wang, Jibing Liu.
Revision for important intellectual content: Jibing Liu, Yiling Zheng, Liming Wang.
Supervision: Jibing Liu, Mei Liu.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/CBM-203003.
sj-docx-1-cbm-10.3233_CBM-203003.docx - Supplemental material
Supplemental material, sj-docx-1-cbm-10.3233_CBM-203003.docx
Footnotes
Acknowledgments
This work was supported by Beijing Municipal Science and Technology Project (Z181100001718191), National Natural Science Foundation (81641113).
Conflict of interest
There are no conflicts to disclose.