
Abstract
BACKGROUND:
The prognostic value of D-dimers concentration in portal blood in patients with pancreatic cancer has been established in several studies. Thyroid hormones and their receptors, especially T3 also seems to have a specific role in process of neoplasia and metastatic spread.
OBJECTIVE:
The aim of the study was to look for changes of thyroid hormones concentration between portal and peripheral blood.
METHODS:
We included prospectively 8 patients with pancreatic cancer, without liver dysfunction, qualified to surgical treatment. D-dimers, THS, fT3, fT4 concentration was determined in blood samples from portal and peripheral vein taken intraoperatively.
RESULTS:
The difference and quotient of portal and peripheral concentration of D-dimers, THS, fT3 and fT4 was calculated (D-dimer-; THS-; fT3-; fT4-d and -q). The level of D-dimers measured in portal blood was
CONCLUSIONS:
We suggest that fT3 or its receptors can influence progression of pancreatic malignancies. The results of this study are also a new evidence that both fT3 and portal D-dimers are biologically linked to intensity of local neoplastic process. Nevertheless, deeper knowledge about portal circulation probably constitute missing part in understanding nature of pancreatic neoplasia. Investigations both on larger group and in the field of basic sciences are needed.
Background
L-thyroxine (T4), main thyroid hormone and its most important metabolite, 3,3’,5-Triiodo-L-thyronine (T3) influence many cell processes. Blood carries those hydrophobic particles bound to special proteins (proteins thyroxine binding globulin (TBG), transthyretin (TTR), albumin or apolipoprotein B100), so only a part of whole T3 and T4 is detectable as free (fT3, fT4) [1] and has a possibility to go through the cell membrane to react with its nuclear receptor (thyroid hormone receptors, TRs) [2].
Many studies investigated probable link between hyperthyroidism history and cancer. Moeller and Fuhrer review [3] cites studies which proved statistical connection between occurrence and course of cancer and hyperthyroidism (ovarian, prostate, breast cancer or general cancer incidence) [4, 5, 6, 7], as well as longer survival among the patients who developed hypothyroidism as side effect of standard treatment (astrocytoma, head and neck cancers) [8, 9]. Thyroid hormones and their receptors, especially T3 also seems to have a specific role in process of neoplasia and metastatic spread [10, 11, 12, 13, 14, 15].
There is not many information about portal blood substance concentrations. Thyroid hormones concentration measured in portal blood of healthy organism should presumably be equal to peripheral norms [16]. The prognostic value of D-dimers concentration in portal blood in patients with pancreatic cancer has been established in several studies [17, 18, 19].
Material and methods
This single centre clinical preliminary study comprised patients with pancreatic malignancy (adenocarcinoma ductale,
Results
Detailed characteristics of patients is presented in Table 1. Concentration of TSH, fT4 and fT3 was within normal range in all patients except two measurements in two separate patients (fT3 3,84; TSH 7,32), which we found clinically not significant.
Patients characteristics
Patients characteristics
We divided all subjects into 2 groups according to portal D-dimer concentration. The level of D-dimers measured in portal blood was
Peripheral fT3 concentration in patients with low and high portal D-dimers concentration.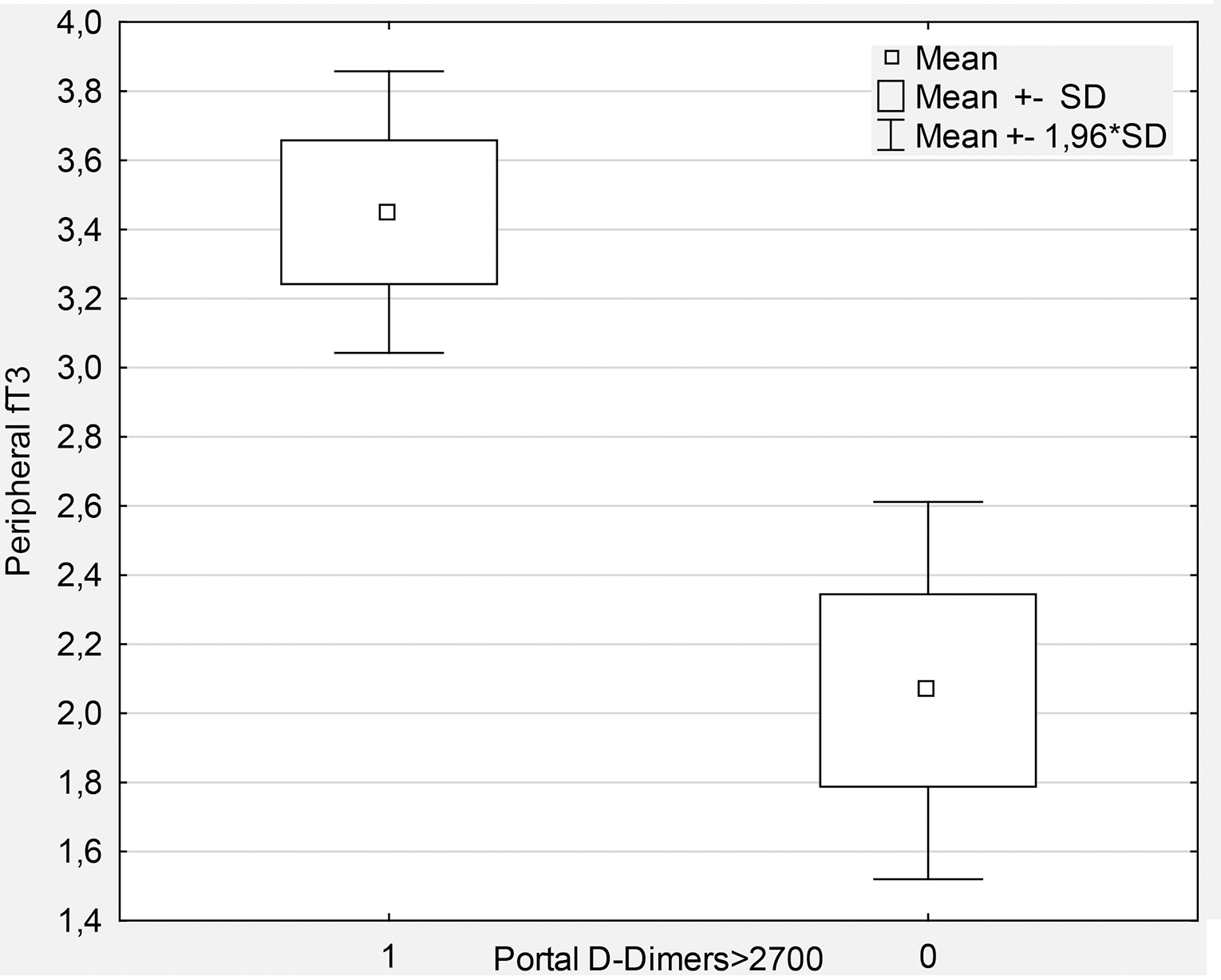
The difference between portal and peripheral concentration of THS, fT3 and fT4 was calculated using two formulas: subtraction (portal minus peripheral level of hormone) and division (portal divided by peripheral level of hormone): THS-; fT3-; fT4-d or -q, respectively. Pearson’s correlation analysis revealed that both fT3-diff and fT3-quot statistically significantly correlate with portal D-dimers level, D-dimers-d and -q, but not with peripheral level of D-dimers concentration (fT3-d
The level of fT3 in a blood sample is a reflection of an equilibrium between many mechanisms of its elevating and lowering. A few most important are: T3 production in thyroid gland and thanks to tissue deiodinases activity, T3 binding by serum proteins and use of T3 in target tissues. Thyroid hormones are necessary for many physiological processes to proceed, including influence on appropriate cell growth [37].
D-dimer diff vs. fT3 diff Pearson’s 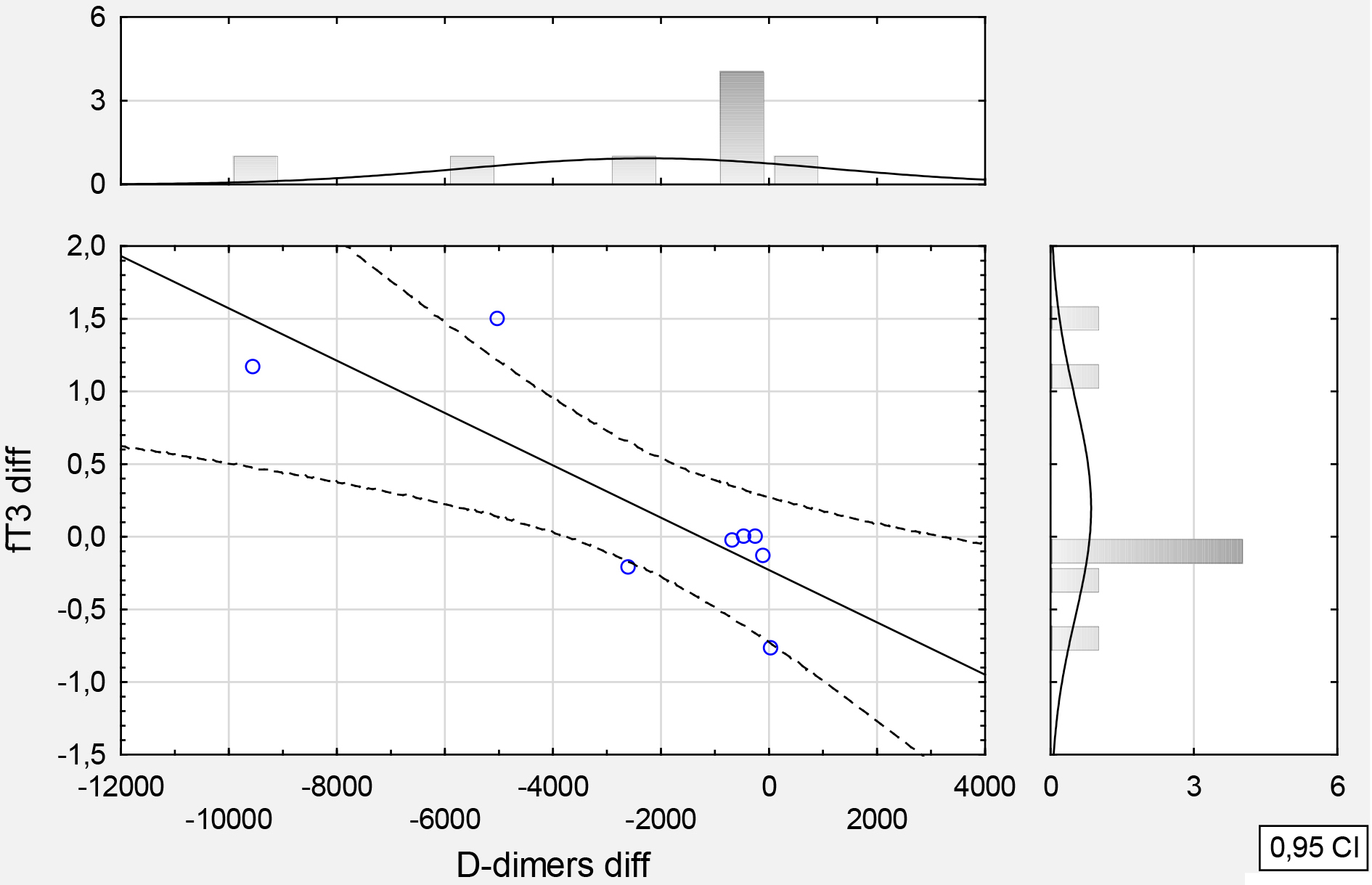
Changes of serum thyroid hormones concentration accompanying different cancer were widely described in world literature so far [4, 5, 6, 7, 8, 9]. Except statistical relation between hypothyroidism and cancer history in some patient population there are two phenomena deserving of attention: consumptive hypothyroidism and low T3 syndrome. Consumptive hypothyroidism was initially considered as paraneoplastic syndrome remarkably linked to hepatic vascular tumours occurring mainly in children due to hyperactivation of tissue deiodinase type 3 (D3) that turns T4 and T3 into its inactive products reverse T3 (rT3) and diiodothyronine (T2) [20, 21, 22]. In 2005 Ruppe et al. described first known case of consumptive hypothyroidism in adult patient 13-year history of difficult to treat hypothyroidism, finally diagnosed with malignant nonvascular cancer [23], which definitely indicates that D3 hyperactivation is not an exclusive feature of one neoplasm. On the other hand low T3 syndrome, defined as low serum fT3 level without increase of fT4 and TSH serum levels [24], although occurs in many sever diseases like septic shock, multiple trauma, burn [25, 26, 27], constitute also independent predictor of poor outcome in neoplastic diseases, eg. diffuse large B cell lymphoma, chronic lymphocytic leukemia, lung cancer or in patients undergoing brain tumour surgery [28, 29, 30]. Duyu et al. described low T3 syndrome in children diagnosed with cancer (not liver haemangioma); they found that 10.6% of whole tested population fulfilled also criterium of rT3 level increase and what is worth noting, incidence of low T3 syndrome was independent of stage of disease [31]. The dynamics of thyroid gland disfunction in natural course of sarcoma was describe using experimental rat model; changes were notable from the first days of tumour growth, developing liver metastases was associated with TSH increase and fT3 drop which transformed into full low T3/low T4 syndrome while lung metastatic spread occurred [32]. Rodriguez-Molinero et al. reported two cases of patients diagnosed with breast and pancreatic cancer treated experimentally with methimazole and increasing doses of liothyronine, in order to reduce endogenous T4, as there are some preclinical evidences that T4 promote tumour growth while T3 demonstrate some antineoplastic properties [33, 34, 35, 36]. They observed inverse relationship between serum fT3 and Ca 19-3 levels and postulated this observation to be a sign of direct biochemical response to exogenous L-T3. Study of Moriggi at al. [37] showed that after exposing cell line on T3 in hPANC-1 (cell line from ductal adenocarcinoma) the presence of
We suggest that fT3 or its receptors can influence progression of pancreatic malignancies. The results of this study are also a new evidence that both fT3 and portal D-dimers are biologically linked to intensity of local neoplastic process and promoting metastasizing. Taking into consideration extremely small number of patients enrolled into this study the laboratory error or coincidence should possibility should not be excluded. Nevertheless, deeper knowledge about portal circulation probably constitute missing part in understanding nature of pancreatic neoplasia. Investigations both on larger group and in the field of basic sciences are needed.
Limitations of the study
Number of subjects constitute main, impossible to overlook limitation of this study. Despite the fact, that this is preliminary study, small group does not allow to be sure that observed dependence is not a simple coincidence. In the light of final study hypothesis not involving into protocol the measurements of thyroid hormones binded forms’ concentration seems to be the second major limitation.
Footnotes
Conflict of interest
The author(s) declare that they have no competing interests.