: This study aimed to assess the significance of combined expression of interleukin-2 receptor (CD25) and the interleukin-3 receptor (CD123) in acute myeloid leukemia (AML) patients.
METHODS
: The expression of CD25 and CD123 on blast cells in bone marrow samples were identified by flowcytometry in 94 patients ( 60 years old) with de novo acute myeloid leukemia (AML) treated at the Mansoura University Oncology Center (MUOC).
RESULTS
: Of the 94 samples at diagnosis there were 17 (18.1%) CD25/CD123 (double positive) cases; 25 (26.6%) CD25/CD123 (single positive); 32 (34.0%) CD25/CD123 (single positive) cases; 20 (21.3%). CD25/CD123 (double negative). Most of the AML patients have double CD25/CD123 were significantly associated with poor and intermediate risk as compared to those associated with those in the good risk group ( 0.005). The lowest induction of remission was recorded in AML patients have double CD25/CD123 expression as compared to the remaining AML patient group. Study the effect of these biomarkers on the overall survival reveal that AML patients exhibited double CD25/CD123 expression had significantly shorter overall survival as compared to negative ones.
CONCLUSION:
Double CD25/CD123 co-expression in AML patients is a dismal prognostic marker and could be used as novel biomarker for risk stratification for AML patients.
In spite of the marked progress in our understanding the biology of acute myeloid leukemia (AML), their treatment represents a challenge for both hematologists and oncologists. Acute Myeloid Leukemia (AML) remains an incurable disease in most of the cases. AML was ranked as the 6th highest cancer-related death in male population (Cancer Facts and Figures 2014, American Cancer Society). Leukemia stem cells (LSC) are a subpopulation of leukemic cells responsible for the continued proliferation and propagation of bulk leukemic cells. Growing evidence support the notion that Leukemic stem cells (LSCs) are the seed source of disease relapse and treatment resistance. Among the markers mentioned for leukemic stem cells are CD123 and CD25 [1, 2].
CD25 is known as interleukin 2 (IL2) receptor alpha (IL2RA). IL-2 cytokine regulates cell proliferation, differentiation, survival and apoptosis [3]. CD123 is known as interleukin 3 receptor, alpha (IL-3R). IL3R is a heterodimeric cytokine receptor composed of the alpha unit and beta unit, which well be activated by ligand binding [4]. IL-3 is one of the prominent cytokines that controls proliferation, growth and differentiation of hematopoietic cells [5].
In acute myeloid leukemia (AML) with normal cytogenetics; recurrent genetic aberrations govern the prognostic stratification of that subgroup of patients. In the context of this evolving molecular risk assessment, antigen-expression profiles have been identified as surrogates for certain leukemic genotypes. Furthermore, a few single antigens per se have been found to be predictive of clinical response. In most cases, however, the prognostic power of antigens has not been disassociated from underlying genetic determinants [6].
Recently many authors [7, 8, 9] have shown that CD123 is unique marker of AML leukemic stem cells. Also, CD25 (IL-2 receptor-) was previously reported to be frequently expressed by AML blast cells [9, 10]. Therefore, the aim of this study was to determine the impact of CD25/CD123 co-expression on disease characteristics as well as patient’s outcome.
Methods
Patient samples
This study included 94 AML patients who were 60 years old at diagnosis was included in this study after wrote informed consent. The study was approved by the Institutional Revision Board (IRB) of Mansoura University. Diagnostic bone marrow and/or peripheral blood samples were taken from the all investigated patients. The patients were subjected to both morphological examination of the peripheral blood smear and bone marrow smear, immunophenotypic evaluation using antibodies panel included CD34PE (Clone8G12), MPOPE (clone 5B8) CD33PE (Clone D3HL60.251), CD13FITIC (Clone SJIDI), CD117PE (Clone 10uD2), HLADR Percep-Cy (Clone G4606); CD61FITC (VI-PL2), CD14APC (Clone rmC5-3), CD61FITC (clone HI-PL2); CD64PE (Clone22), Glycophorin FITC (Clone 11E4B-7-6) by flow cytometry. The included AML patients were followed up to 12 months or until death.
Inclusion criteria Age 18–60 years Primary AML before start of therapy Exclusion Criteria M3 variant Secondary AML
All of these patients received standard treatment consisting of two cycles of induction chemotherapy followed by either a third cycle, autologous or allogeneic stem cell transplantation, dependent on pre-treatment risk assessment.
Cytogenetic analysis
Analysis of conventional karyotyping was done on bone marrow aspiration samples by staining the cells in the metaphase by using standard banding techniques which was obtained in unstimulated culture. FISH techniques was used to detect t (8; 21); inv 16; t (16; 16), abnormality in chromosome 5, 7, trisomy 8; or 11q23. PCR techniques was used for detection of t (9; 22). Patients with regular translocation: t (8; 21), abnormal (16) was stratified in favorable risk category. On the other hand patients with normal karyotype, numerical or structural deletion of chromosome 7 or 5, trisomy 8, t (9; 22), 11q23 rearrangements, and other chromosome abnormalities were pooled together as intermediate/poor-risk category [11, 12]. The study has been approved by Mansoura faculty of medicine local ethics committee and that it conforms to the provisions of the Declaration of Helsinki.
Flow cytometric determination of CD25/CD123 cell antigen expression
Whole fresh bone marrow cells collected in EDTA ( 10/tube) were incubated with combinations of monoclonal antibodies (MoAbs) at room temperature for 15 min. Erythrocytes were then lysed in 2 mL FACSTM lysing solution (Becton Dickinson, San Diego, CA, USA). Cells were consequently washed twice by phosphate buffered saline (PBS) and analyzed by 8-color flow cytometry using a FACS Calibur flow cytometer with CellQuest software (Becton Dickinson; USA) [13].
The gating of the leukemic blast cells was based on their CD45APC (Clone LOPC-21) expression and side scatter (SSC). Expression of CD25 PE (Clone 3C7), CD123 FITC (Clone 5B11) on gated leukemic myeloblasts were assessed. At least 10,000 events/tube were measured. Threshold for positivity were based on isotype negative controls. The positivity was defined when CD25 and CD123 expression 20% above the isotypic control. The blast cells were analyzed using one – step acquisition procedure. Expression of CD25 and CD123 was reported as percentage of antibody-binding leukemic myeloblasts [14].
AML patient’s characteristics
Item
No (%)
Sex
Male
54
(57.4%)
Female
40
(42.6%)
FAB subtypes
M0
3
(3.2%)
M1
15
(14.9%)
M2
17
(18.0%)
M4
35
(37.2%)
M5
13
(13.8%)
M6
8
(8.5%)
M7
3
(3.2%)
Blood blast cells % median (range)
32
(5–92%)
Bone marrow blasts% median (range)
55
(24–92%)
Cytogenetic
Favorable (good)
35
(37.2%)
Unfavorable (poor/intermediate risk)
59
(62.8%)
Induction of remission
Responder
55
(58.5%)
Non-responder
39
(42.5%)
CD25 expression
Positive
25
(26.6%)
CD123 expression
Positive
32
(34.0%)
Combined CD25/CD123 expression
Positive
17
(18.1%)
Negative for CD25; CD123 or both
77
(81.9 %)
Deaths
Survived
55
(58.5%)
Died
49
(41.5%)
Statistical analysis
Patient data were compared using the Fisher exact test if they were categorical and Wilcoxon rank sum tests if they were continuous. Overall survival (OS) was defined as time from randomization to death from any cause. OS probabilities were estimated by use of the Kaplan-Meier method, and statistical significance of associations was assessed with the log-rank test.
The percentages of antigen expressing blast cells or density of expression (for CD25, CD123) were considered continuous variables and compared with the nonparametric Wilcoxon rank sum test. The significant level was considered if 0.05.
Results
The AML patient’s characteristics is shown in Table 1. Of the 94 samples at diagnosis there were 17 (18,1%) CD25/CD123 (double positive) cases; 25 (26.6%) CD25 CD123 (single positive); 32 (34.0%) CD25/CD123 (single positive) cases; 20 (21.3%). CD25/CD123 (double negative). Figure 1A showed the gating on the AML blasts using CD45 and side scatter; the blast cells are negative for CD45. The flowcytometry results of three AML cases are shown in Fig. 1B and D; Fig. 1B illustrate AML case that is single positive for CD123; Fig. 1C showed AML case single positive for CD25 and Fig. 1D is the result of AML case double positive for CD25/CD123 expression.
Relation between CD25 and CD123 expression and AML induction of remission response and cytogenetic grade
The number of AML patients have either single CD25, or CD123, or double CD25CD123 were significantly higher among poor risk and intermediate risk cytogenetically group as compared to those with good cytogenetic group ( 0.01). Regarding the induction of remission response there were significant difference between AML cases have single CD25, CD123, or double CD25/CD123 as compared to those negatively expressed those biomarkers ( 0.01) (Table 2).
Impact of single CD25, CD123 and double CD25/CD123 expression on the induction of remission response as well as cytogenetic grade
CD25 expression
CD123 expression
CD25/CD123 expression
Negative for all
positive ( 25)
positive ( 32)
positive ( 17)
( 20)
Induction of remission
Responder ( 55)
8/25 (32%)
19/32 (59.3%)
8/17 (47%)
20/20 (100%)
Non-responder ( 39)
17/25 (68%)
13/32 (40.7%)
9/17 (53%)
0 (0.0%)
value
0.01
Cytogenetics
Good ( 35)
7/25 (28%)
10/32 (31.3%)
2/17 (11.8%)
16/20 (80%)
Intermediate/poor ( 59)
18/25 (72%)
22/32 (68.7%)
15/17 (88.2%)
4/20 (20%)
value
0.01
The Cox proportional hazards of CD25/CD123 co-expression on AML survival
We tested the impact of age; WBCs count; Cytogenetic grade and CD25/CD123 co-expression on the AML patients’ survival by univariate analysis and the significant parameter in univariate analysis were included in multivariate analysis. Univariate analysis showed significant effect of the age, Cytogenetic grade, and CD25/CD123 co-expression. In multivariate analysis only CD25/CD123 co-expression and Cytogenetic grade continues to have significant odds ratios (Table 3). The hazard ratio for CD25/CD123 co-expression was 3.13 (95% CI 1.5–16.7) and for cytogenetic grade was 52.62 (95% CI 6.9–96.9) (Table 3).
Cox proportional hazards of age, WBCs, Cytogenetic grade, and CD25/CD123 co-expression on AML patient’s survival
Parameters
Univariate analysis
Multivariate analysis
HR (95% CI)
-value
HR (95% CI)
-value
Age/years
0.039
1.04
(1.002–1.79)
0.038
1.11
(0.98–1.26)
0.077
WBCs 10/L
0.934
0.393
(0.152–1.016
0.054
0.9
(0.072–14.6)
0.753
C25/CD123 co-expression
3.62
27.5
(4.8–58.1)
0.001
3.13
(1.5–16.7)
0.011
Cytogenetic grade
3.716
41.08
(8.19–205)
0.001
52.62
(6.9–96.9)
0.001
Showed the flowcytometry gating for blast cells; CD25 and CD123 expression. a. Showed gating on the blast cells population using CD45 and side scatter; b. AML case single positive for CD123; c. AML case single positive for CD25; d. AML a case double positive for CD25 and CD123.
Impact of CD25 and CD123 expression on AML patients overall survival (OS) and disease free survival (DFS)
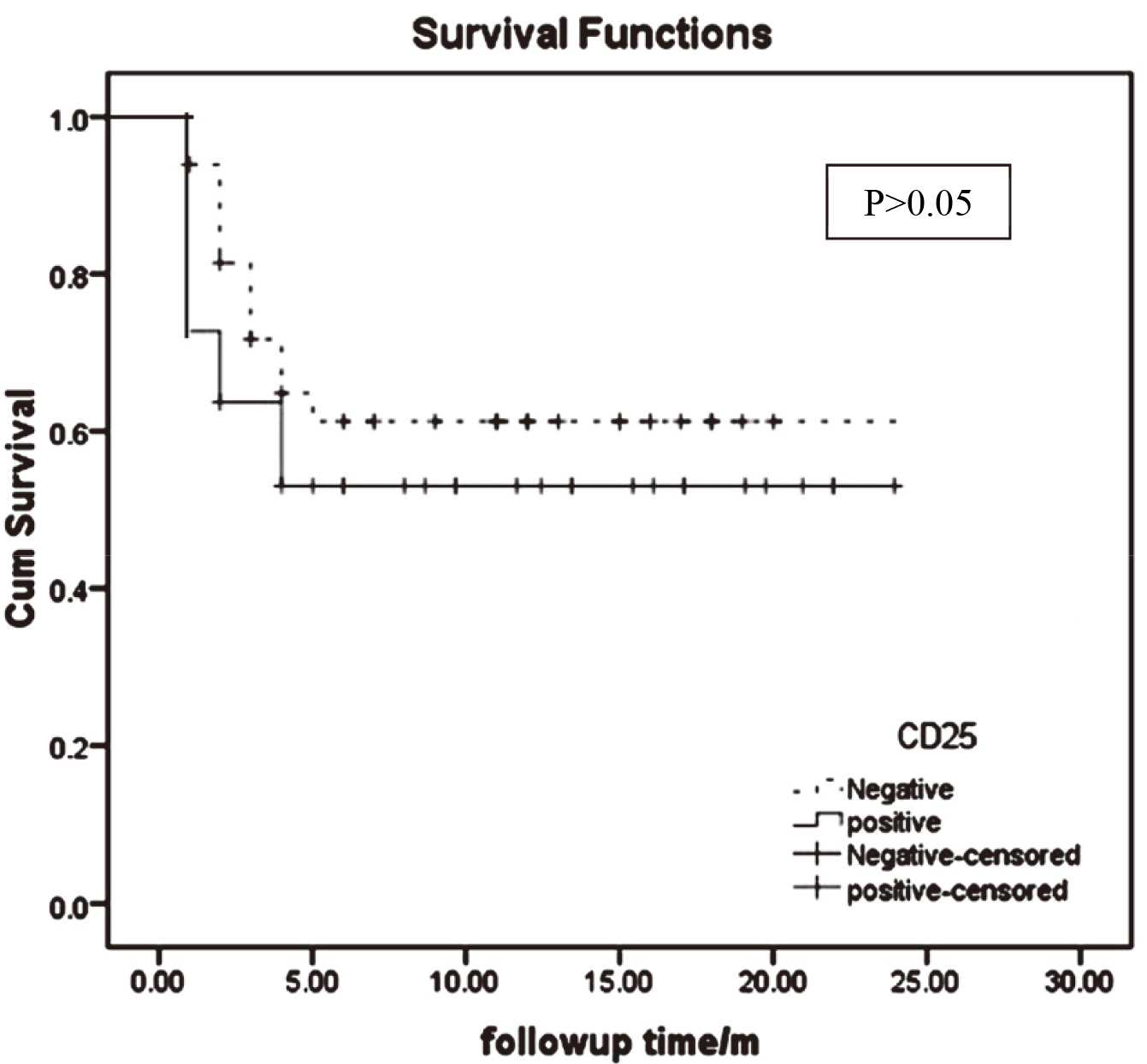
Study the effect of the expression of these biological markers (CD25CD123) on the overall survival reveal that AML patients exhibited double CD25CD123 co-expression had significantly shorter overall survival as compared to the remaining group (Figs 2–4). Likewise, AML patients harbored positive co-expression of CD25 and CD123 had the shortest disease survival as compared to those lacking co-expression ( 0.002) (Fig. 5).
Kaplan-Meier curve showed the impact of single CD25 expression in AML. It is evident that there is no significant difference between the 2 groups ( 0.05).
Kaplan-Meier curve showed the impact of single CD123 expression in AML. It is evident that there is no significant difference between the 2 groups ( 0.05).
Kaplan-Meier curve showed the impact of CD25/CD123 co-expression on AML patients’ overall survival. It is clear that the AML group showed double positive expression of CD25/CD123 co-expression had bad impact on AML survival as compared to those lack positive co-expression ( 0.01).
Impact CD25/CD123 co-expression on AML patients’ disease-free survival. There is significant difference ( 0.002).
Discussion
CD25 positive expression was identified in 25/94 patients (26.7%). Similar finding was reported by Miltiades et al. [15] who studied CD25 expression in myelodysplastic syndrome AML blasts and reported that CD25 positive expression was detected in 14 patients (17%) at diagnosis. Moreover, Cerny et al. [10] found that the positive expression of CD25 at diagnosis was a strong predictor of treatment failure (induction failure and relapse). Also, Khasawneh and Abdel-Wahab [16] concluded that the determination of CD25 expression status improves prognostic risk classification in AML independent of established biomarkers and could be predict patient responses and minimal residual disease.
The biological role of CD25 expression in AML remains unknown and the effect of IL-2 on the proliferative status of CD25 blasts is also controversial [17]. CD25 may impart environmental signals, whereas high plasma levels of enzymatically cleaved, soluble CD25 in AML may suppress the antitumor response via competition with the lymphocyte surface CD25 for IL-2 and have long been shown to be associated both with the burden and severity of the disease [15, 18]. CD25 expression on AML cells may control cell-to-cell interactions or represents a specific stage of differentiation and maturation of myeloid progenitors, or a chemo resistant state. IL2 increases survival and chemotherapy resistance in CD25 chronic lymphocytic leukemia in vitro [19]. The poor prognostic relevance of CD25 expression in adult ALL patients were independent of the presence or absence of BCR/ABL [20, 21].
In the present study, positive expression of CD123 was detected in 32/94 of AML patients (34.0%). CD123 was described to be a marker of leukemic stem cells (CD34CD123 cells) [22]. Chávez-González et al. [23] detected an increased frequency of CD96 and CD123 cells within the CD34 cell population from pediatric AML. Our study supports the notion that expression of such antigens should be explored for their use as markers for diagnosis and prognosis.
In our study, the CD25CD123 co-expression was detected in 17/94 (18.1%). The number of AML patients have double CD25/CD123 expression was significantly higher among cytogenetically poor risk and intermediate risk group as compared to those in the good cytogenetic group ( 0.001, 0.02, 0.005 respectively). This finding points out for the poor prognostic relevance of positive of CD25/CD123 co-expression.
Regarding the induction of remission response in the present study; there were significant difference between AML cases have CD25, or CD123, or those double CD25/CD123 as compared to those have negative expression of those markers. This finding come in parallel with that reported by Thol et al. [24] and Hou et al. [25]; they observed that CD25 expression was associated with a reduced response to induction chemotherapy, irrespective of the dose of daunorubicin.
Study the effect of these markers on the overall survival reveal that, only AML patient’s subgroup exhibited double CD25/CD123 had significantly shorter overall survival. The poor outcome of CD25 AML patients has been attributed to the chemo resistant properties of the LSC-like, CD25 myeloblasts, a fact illustrated on the higher rates of both induction failure [14] and relapse. Moreover, it was reported that the presence of more than 1% of CD34/CD38/CD123 cells had a negative impact on disease-free survival and overall survival [9, 26].
The effect of IL-3R expression in leukemic stem cells (LSCs) was explored in many studies [8, 9]. An initial study by Jordan and coworkers [7] provided evidence that CD34/CD38 purified leukemic cells, enriched in LSCs, overexpress in the majority of AMLs CD123. CD123/CD34 leukemic cells were able to initiate a leukemic process when transplanted into immunodeficient mice [8]. The CD123 was then used in other studies as a marker to isolate LSC populations from AML samples and to provide a characterization of these cells and it was shown that these cells display a constitutive activation of NF-kB [8].
The poor outcome of CD25 AML patients has been attributed to the chemo resistant properties of the LSC-like, CD25 myeloblasts, a fact illustrated on the higher rates of both induction failure [14] and relapse [10, 17]. In a recent study, Zeijlemaker et al. [27] studied the impact of LSC (CD34/CD38) on the AML patients’ outcome and demonstrating that LSC strongly improves prognostic impact of MRD detection, identifying a patient subgroup with an almost 100% treatment failure probability, and recommended LSC measurement incorporation in future AML risk schemes. Different mechanisms may contribute to the resistance of LSCs to current therapies. LSCs express drug efflux proteins that lead to multidrug resistance. In addition, most cytotoxic drugs and irradiation depend on cell division in order to induce cell death but LSCs are largely quiescent. Many stem cell characteristics including quiescence are determined by interactions with the niche [28, 29]. The limitation of our study is the low number of the AML patients.
Conclusions
CD25/CD123 double expression had bad impact on AML patient’s outcome. Determination of CD25CD123 expression in AML patients at diagnosis could be used for prognostic stratification for those patients.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
References
1.
EhningerA.KramerM.RölligC.ThiedeC.BornhäuserM.von BoninM.WermkeM.FeldmannA.BachmannM.EhningerG. and U Oelschlägel on behalf of the Study Alliance Leukemia, Distribution and levels of cell surface expression of CD33 and CD123 in acute myeloid leukemia, Blood Cancer J4(6) (2014), e218.
2.
AllanJ.RobozG.AskinG.RitchieE.ScanduraJ.ChristosP.HassaneD. and GuzmanM., CD25 expression and outcomes in older patients with acute myelogenous leukemia treated with plerixafor and decitabine, Leuk Lymphoma59 (2018), 821–828.
3.
DriesenJ.PopovA. and SchultzeJ.L., CD25 as an immune regulatory molecule expressed on myeloid dendritic cells, Immunobiology213 (2008), 849–858.
4.
TestaU.PelosiE. and FrankelA., CD123 is a membrane biomarker and a therapeutic target in hematologic malignancies, Biomarker Res2 (2014), 4.
5.
ThomasD.VadasM. and LopezA., Regulation of hematopoiesis by growth factors – emerging insights and therapies, Expert Opin Biol Ther4 (2004), 869–879.
6.
GönenM.SunZ.FigueroaM.A.PatelJ.P.Abdel-WahebO.RacevskisJ.KetterlingR.P.FernandezH.RoweJ.M.TallmanM.S.MelnickA.LevineR.L. and PaiettaE., CD25 expression status improves prognostic risk classification in AML independent of established biomarkers: ECOG phase 3 trial, E1900, Blood120(11) (2012), 2297–2306.
7.
JordanC.T.UpchurchD.SzilvassyS.J.GuzmanM.L.HowardD.S.PettigrewA.L.MeyerroseT.RossiR.GrimesB.RizzieriD.A.LugerS.M. and PhillipsG.L., The interleukin-3 receptor alpha is a unique marker for human acute myelogenous leukemic stem cells, Leukemia14(10) (2000), 1777–1784.
8.
GuzmanM.L.NeeringS.J.UpchurchD.GrimesB.HowardD.S.RizzieriD.A.LugerS.M. and JordanC.T., Nuclear factor-kappa B is constitutively activated in primitive acute human acute myelogenous leukemia cells, Blood98 (2001), 2301–2307.
9.
VergezF.GreenA.S.TamburiniJ.SarryJ.E.GaillardB.Cornillet-LefebvreP.PannetierM.NeyretA.ChapuisN.IfrahN.DreyfusF.ManentiS.DemurC.DelabesseE.LacombeC.MayeuxP.BouscaryD.RecherC. and BardetV., High levels of CD34+CD38low/-CD123+ blasts are predictive of an adverse outcome in acute myeloid leukemia: A Groupe Ouest-Est des Leucemies Aigues et Maladies du Sang (GOELAMS) study, Haematologica96 (2011), 1792–1798.
10.
CernyJ.YuM.RamanathanH.RaffelG.D.WalshW.V.FortierN.ShanahanL.O’RourkeE.BednarikJ.BartonB.Kroll-DesrosiersA.HaoS.WodaB.HutchinsonL.EvensA.M.RosmarinA.G. and NathR., Expression of CD25 independently predicts early treatment failure of acute myeloid leukaemia (AML), Br J Hematol160(2) (2013), 262–266.
11.
SlovakM.L.KopeckyK.J.CassilethP.A.HarringtonD.H.TheilK.S.MohamedA.PaiettaE.WillmanC.L.HeadD.R.RoweJ.M.FormanS.J. and AppelbaumF.R., Karyotypic analysis predicts outcome of pre remission and post remission therapy in adult acute myeloid leukemia: A Southwest Oncology Group/Eastern Cooperative Oncology Group Study, Blood96(13) (2000), 4075–4083.
12.
StasiR.Del PoetaG.MasiM.TribaltoM.VendittiA.PapaG.NicolettiB.VernoleP.TedeschiB.DelarocheI.MingarelliR. and DallapiccolaB., Incidence of chromosome abnormalities and clinical significance of karyotype in de novo acute myeloid leukemia, Cancer Genet Cytogenet67 (1993), 28–34.
13.
AngeliniD.F.OttoneT.GuerreraG.LavorgnaS.CittadiniM.BuccisanoF.De BardiM.GarganoF.MaurilloL.DivonaM.NogueraN.I.ConsalvoM.I.BorsellinoG.BernardiG.AmadoriS.VendittiA.BattistiniL. and Lo-CocoF., A leukemia-associated CD34/CD123/CD25/CD99+ immunophenotype identifies FLT3-mutated clones in acute myeloid leukemia, Clin Cancer Res21(17) (2015), 3977–3985.
14.
PaiettaE.NeubergD.BennettJ.M.DewaldG.RoweJ.CassilethP.CripeL.TallmanM.WiernikP. and the Eastern Cooperative Oncology Group, Low expression of the myeloid differentiation antigen CD65s, a feature of poorly differentiated AML in older adults: Study of 711 patients enrolled in ECOG trials, Leukemia17(8) (2003), 1544–1550.
15.
MiltiadesP.LamprianidouE.VassilakopoulosT.PapageorgiouS.GalanopoulosA.VakalopoulouS.GarypidouV.PapaioannouM.HadjiharissiE.PappaV.PapadakiH.SpanoudakisE.TsatalasK. and KotsianidisI., Expression of CD25 antigen on CD34+ cells is an independent predictor of outcome in late-stage MDS patients treated with azacitidine, Blood Cancer Journal4 (2014), e187.
16.
KhasawnehM.K. and Abdel-WahabO., Recent discoveries in molecular characterization of acute myeloid leukemia, Curr Hematol Malig Rep9(2) (2014), 93–99.
17.
TerwijnM.FellerN.van RhenenA.KelderA.WestraG.ZweegmanS.OssenkoppeleG. and SchuurhuisG.J., Interleukin-2 receptor alpha-chain (CD25) expression on leukaemic blasts is predictive for outcome and level of residual disease in AML, Eur J Cancer45 (2009), 1692–1699.
18.
CiminoG.AmadoriS.CavaM.C.De SanctisV.PettiM.C.Di GregorioA.O.SgadariC.VegnaL.CiminoG. and MandelliF., Serum interleukin-2 (IL-2), soluble IL-2 receptors and tumor necrosis factor-alfa levels are significantly increased in acute myeloid leukemia patients, Leukemia5 (1991), 32–35.
19.
DeckerT.BognerC.OelsnerM.PeschelC. and RingshausenI., Antiapoptotic effect of interleukin-2 (IL-2) in B-CLL cells with low and high affinity IL-2 receptors, Ann Hematol89 (2010), 1125–1132.
20.
PaiettaE.RacevskisJ.NeubergD.RoweJ.M.GoldstoneA.H. and WiernikP.H., Expression of CD25 (interleukin-2 receptor alpha chain) in adult acute lymphoblastic leukemia predicts for the presence of BCR/ABL fusion transcripts: Results of a preliminary laboratory analysis of ECOG/MRC intergroup study E2993, Leukemia11 (1997), 1887–1890.
21.
GengH.BrennanS.MilneT.A.ChenW.Y.LiY.HurtzC.KweonS.M.ZicklL.ShojaeeS.NeubergD.HuangC.BiswasD.XinY.RacevskisJ.KetterlingR.P.LugerS.M.LazarusH.TallmanM.S.RoweJ.M.LitzowM.R.GuzmanM.L.AllisC.D.RoederR.G.MüschenM.PaiettaE.ElementoO. and MelnickA.M., Integrative epigenomic analysis of adult B-acute lymphoblastic leukemia identifies biomarkers and therapeutic targets, Cancer Discov2 (2012), 1004–1023.
22.
TestaU.RiccioniR.DiverioD.RossiniA.Lo-CocoF. and PestleC., Interleukin 3 receptor in acute leukemia, Leukemia18 (2004), 219–226.
23.
Chávez-GonzálezA.Dorantes-AcostaE.Moreno-LorenzanaD.Alvarado-MorenoA.Arriaga-PizanoL. and MayaniH., Expression of CD90, CD96, CD117, and CD123 on different hematopoietic cell populations from pediatric patients with acute myeloid leukemia, Arch Med Res45 (2014), 343–350.
24.
TholF.DammF.LudekingA.WinschelC.WagnerK.MorganM.YunH.GöhringG.SchlegelbergerB.HoelzerD.LübbertM.KanzL.FiedlerW.KirchnerH.HeilG.KrauterJ.GanserA. and HeuserM., Incidence and prognostic influence of DNMT3A mutations in acute myeloid leukemia, J Clin Oncol29 (2011), 2889–2896.
25.
HouH.A.KuoY.ChouW.C.ChouW.C.LeeM.C.ChenC.Y.LinL.I.TsengM.H.HuangC.F.ChiangY.C.LeeF.Y.LiuM.C.LiuC.W.TangJ.L.YaoM.HuangS.Y.KoS.C.HsuB.S.WuS.J.TsayW.ChenY.C. and TienH.F., DNMT3A mutations in acute myeloid leukemia: Stability during disease evolution and clinical implications, Blood119(2) (2012), 559–568.
26.
ZeijlemakerW.GrobT.MeijerR.HanekampD.KelderA.Carbaat-HamJ.Oussoren-BrockhoffY.Snel1A.VeldhuizenD.ScholtenW.MaertensJ.BreemsD.PabstT.ManzM.van der VeldenV.SlompJ.PreijersF.CloosJ.van de LoosdrechtA.LöwenbergB.ValkP.Jongen-LavrencicM.OssenkoppeleG. and SchuurhuisG., CD34+CD38- leukemic stem cell frequency to predict outcome in acute myeloid leukemia, Leukemia33 (2019), 1102–1112.
27.
ZeijlemakerW.GrobT.MeijerR.HanekampD.KelderA.Carbaat-HamJ.C.Oussoren-BrockhoffY.J.M.SnelA.N.VeldhuizenD.ScholtenW.J., MaertensBreemsD.A.PabstT.ManzM.G.van der VeldenV.H.J.SlompJ.PreijersF.CloosJ.van de LoosdrechtA.A.LöwenbergB.ValkJ.M.Jongen-LavrencicM.OssenkoppeleG. and SchuurhuisG.L.G., CD34+CD38- leukemic stem cell frequency to predict outcome in acute myeloid leukemia, Leukemia33 (2019), 1102–1112.
28.
HwangK.ParkC.J.JangS.ChiH.S.KimD.Y.LeeJ.H.ImH.J. and SeoJ.J., Flow cytometric quantification and immunophenotyping of leukemic stem cells in acute myeloid leukemia, Ann Hematol91 (2012), 1541–1546.
29.
RietherC.SchürchC. and OchsenbeinA., Regulation of hematopoietic and leukemic stem cells by the immune system, Cell Death and Differentiation22 (2015), 187–198.