
Abstract
BACKGROUND:
There has been variability between laboratories in the identification of cancer stem cells (CSCs) markers for epithelial ovarian cancer (EOC). We have evaluated three new surface markers for EOC to identify CSCs precisely.
METHODS:
Three new putative CSCs specific surface markers CD9, CD24 and EPHA1 identified by a bioinformatics approach were evaluated in normal ovary, fallopian tube and ovarian tumours.
RESULTS:
The expression of CD9 alone was observed in normal ovarian surface epithelium and fallopian tube whereas CD24 and EPHA1 were not expressed (
CONCLUSION:
These findings suggest that overexpression of these new markers may be useful in identifying and targeting ovarian CSCs and CD24 may be a putative CSCs marker in ovarian cancer.
Keywords
Introduction
Tumors are a heterogeneous mass of phenotypically different cells consisting of blood vessels, infiltrating macrophages, connective tissue and terminally differentiated malignant cells. A very small proportion of cells in this tumour are clonogenic, both in vitro and in vivo [1]. The development of a tumour according to the stochastic model suggests that every malignant cell in a heterogeneous tumour is capable of forming tumours. While the hierarchical model suggests that cancer stem cells (CSCs) alone are responsible for initiation and maintenance. CSCs shows similarity to normal stem cells in properties like self-renewal and differentiation [2].
Ovarian cancer is one of the leading causes of death and has the highest mortality rate among gynecologic cancers. The five-year overall survival is nearly 80% in the early stages, which declines to 30% with advanced disease. The survival rate for epithelial ovarian cancer (EOC) has remained low despite improved debulking surgery and platinum-based chemotherapy [3, 4]. Survival is still poor as majority of patients have recurrence of the disease. One of the reasons for the recurrence is drug resistance due to persistence of CSCs. These cells are usually not sensitive to conventional chemotherapy comprising of taxol and carboplatin. Although CSCs have been identified in many tumours, there has been variability between laboratories in the identity of cell surface protein that marks these cells in EOC [5, 6]. It has become increasingly apparent that a composite approach is required to identify CSCs with certainty [7].
Using publicly available microarray databases, we have identified CD9, CD24 and EPHA1 cell surface proteins as putative CSCs markers in high grade serous adenocarcinoma (Manuscript submitted). This study reports the expression of CD9, CD24 and EPHA1 in a larger cohort of ovarian tumours and their clinical significance with respect to overall survival (OS) and event free survival (EFS). To our knowledge, there are no immunohistochemical studies in EOC correlating the expression of CD9, CD24 and EPHA1 with clinical outcome.
Materials and methods
Patients
Patients diagnosed with EOC between January 2005 and December 2007 (
The study was approved by the Institutional Ethics Committee. Selection of patients for immunohistochemical study was performed depending upon the availability of the formalin fixed paraffin embedded (FFPE) tumours. We have also examined the FFPE sections from consecutive patients (
The diagnosis of EOC was established using a combination of ascitic fluid cytology, CA 125 estimation, histology and imaging (Ultrasonography or Computed axial Tomography-CT scan).
Bioinformatic analysis
A bioinformatic approach was used to identify new putative ovarian CSCs specific cell surface proteins. The analysis was based on the hypothesis that genes expressed at the embryonic stage may be expressed in cancer. Public microarray databases like Oncomine [8], TCGA [9] and Amazonia [10] were analyzed for genes commonly expressed in embryonic stem cells and ovarian cancer. Further, Human protein atlas was used to analyze the expression of these genes in normal ovary and ovarian cancer at the protein level [11]. The analysis identified 13 differentially overexpressed genes in ovarian cancer. CD24, CD9 and EPHA1 were selected on the basis of their expression and number of databases in which they were differentially overexpressed (Table S1).
Immunohistochemistry
We have evaluated the expression of CD24, CD9 and EPHA1 in sections from normal surface epithelium (OSE), fallopian tube (FT) and normal ovary (each
Evaluation of staining
The expression of CD9, CD24 and EPHA1 was evaluated in each section on the basis of percentage of tumour cells stained (coded as 0: no tumour cells stained, 1: 1–40% staining, 2: 40–80% staining and 3:
Statistical analysis
Overall survival (OS) and event-free survival (EFS) were evaluated as the measures of outcome for the selected patients (
Patients characteristics
Patients characteristics
.
Expression of CD24, CD9 and EPHA1 in normal tissues. An approximate expression of CD24, CD9 and EPHA1 in different types of normal tissues at RNA (GTEX) and protein level derived from online database (Human Protein Atlas).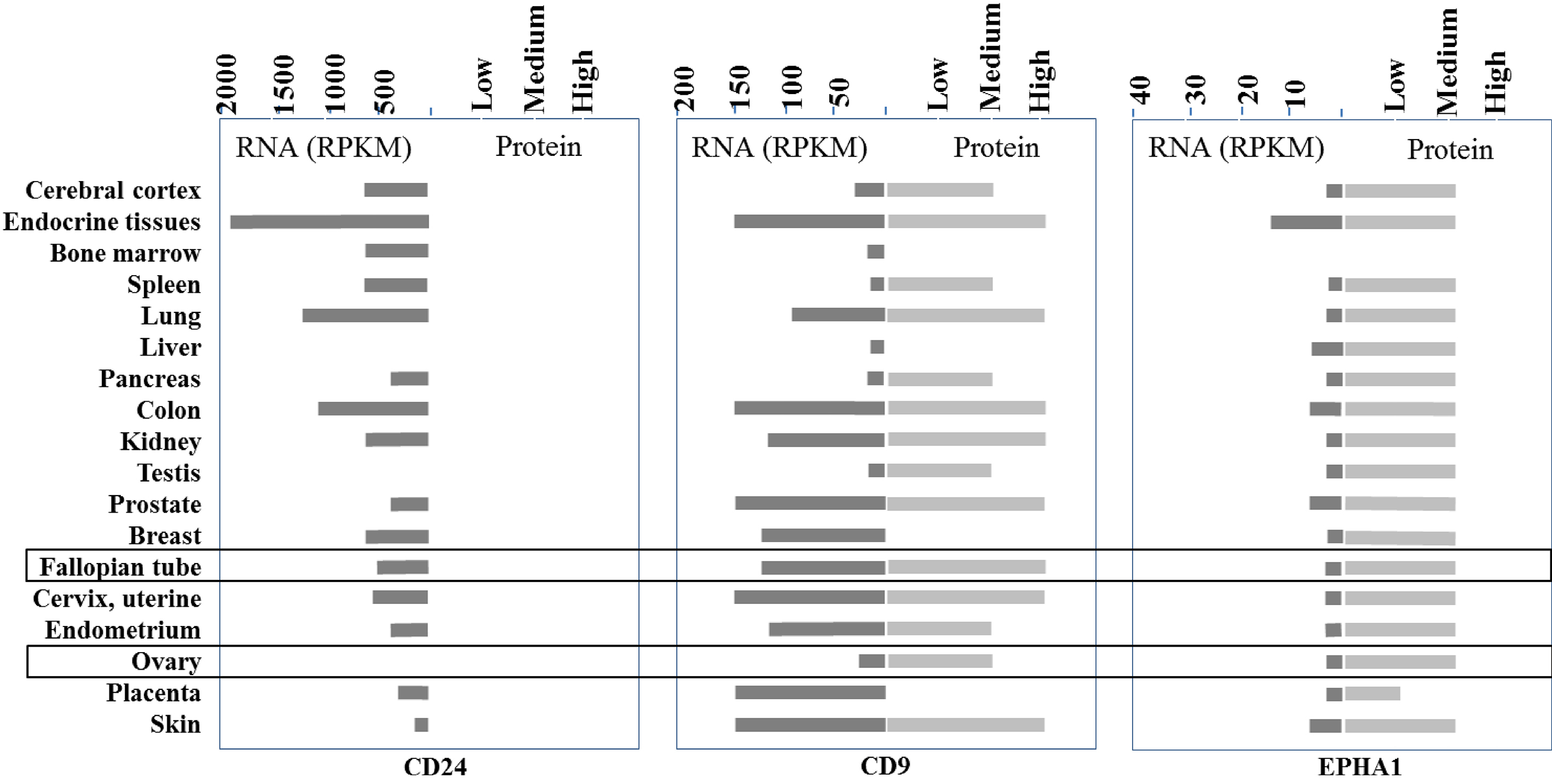
Expression of CSC markers in normal ovarian surface epithelium (OSE), Fallopian tube (FT) and ovary. The immunohistochemistry of normal OSE (Top panel), fallopian tube (Middle panel) and ovary (Lower panel) sections with antibodies against CD9, CD24 and EPHA1 with their respective H and E sections. (Representative image, 400X).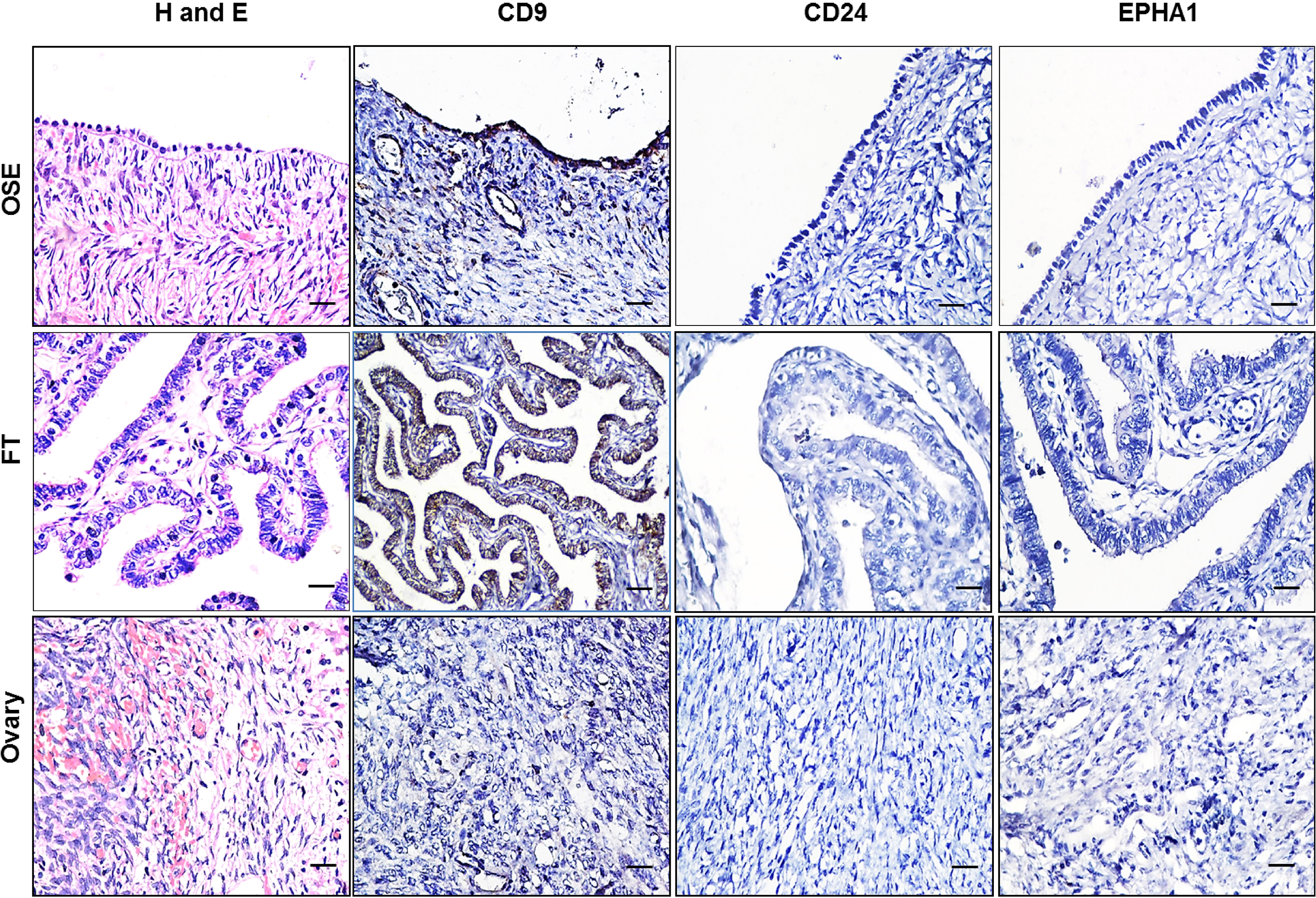
Expression of CD24, CD9 and EPHA1 in ovarian tumours
Patient characteristics
Consecutive patients who presented to the Cancer Institute (WIA) between 2005 and 2007 were selected (
Expression of CD9, CD24 and EPHA1
We have used normal OSE, FT and ovary (each
Normal ovary
CD9 was expressed in both the surface epithelium of the ovary and fallopian tube. CD24 and EPHA1 were not expressed in both OSE and FT. None of the three markers were expressed in the stroma and follicles of the normal ovary (Fig. 2). For comparison, we have also evaluated previously reported ovarian CSCs markers such as CD133, CD117 and CD44. CD117 alone was expressed in FT while CD44 and CD133 were absent in all tissue sections (Data not shown).
Ovarian tumours
The expression of these cell surface markers was evaluated in primary ovarian tumours (
Expression of CD9, CD24 and EPHA1 in ovarian tumours. Immunohistochemistry of representative ovarian tumour sections (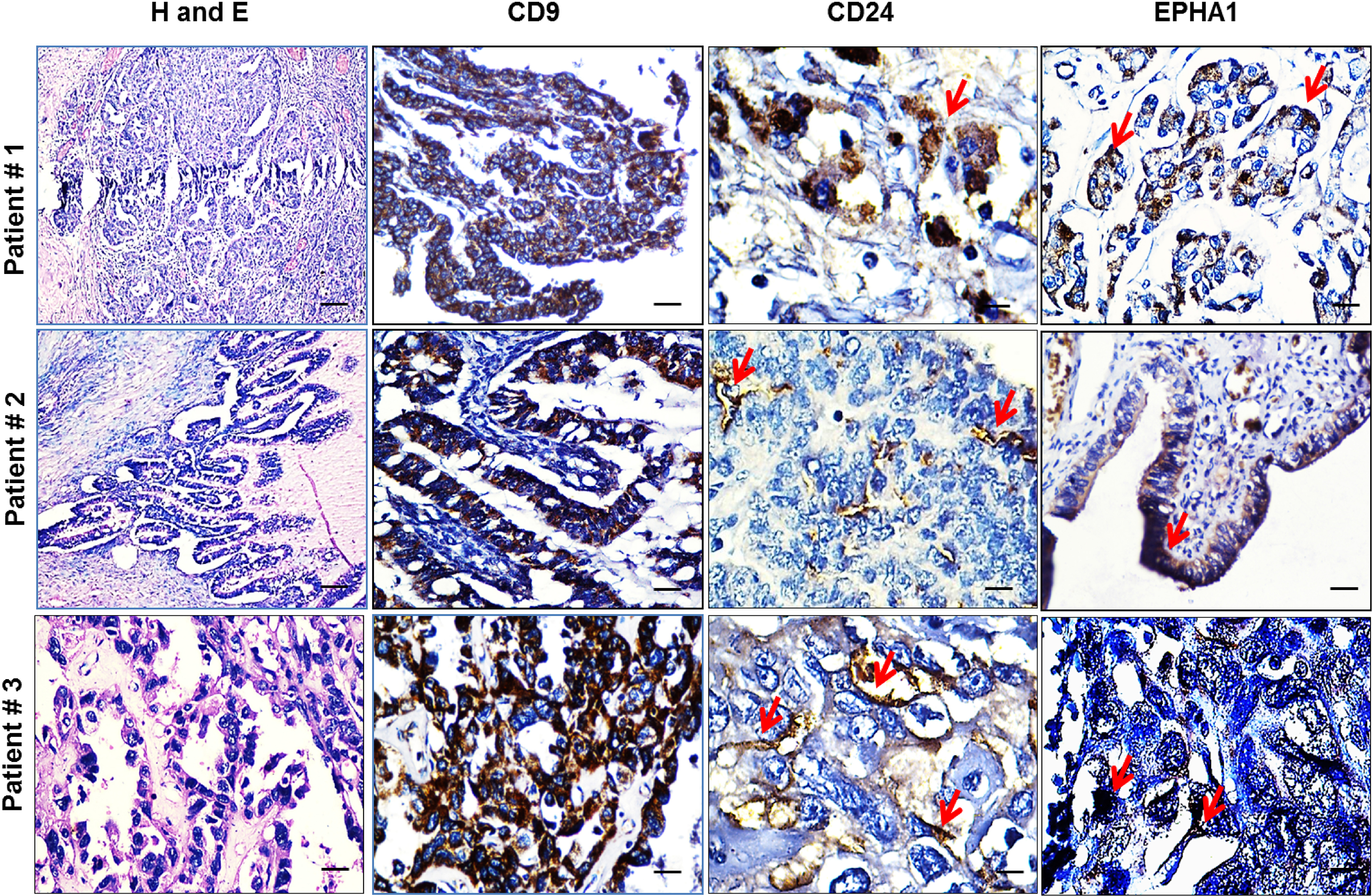
The co-expression of putative CSCs specific surface markers (CD24, CD9 and EPHA1) markers was evaluated in individual FFPE sections of same tumours from the patients with EOC (
Co-expression of CD24, CD9 and EPHA1 in ovarian tumours
Co-expression of CD24, CD9 and EPHA1 in ovarian tumours
The prognostic factors were evaluated in all the 101 patients with EOC by univariate and multivariate analysis. In this cohort of patients, OS and EFS did not significantly correlate with the expression of CD9 (
Correlation of expression of surface markers with outcome. Clinical correlation for expression of CD9, CD24 and EPHA1 with OS and EFS. A. in patients with EOC (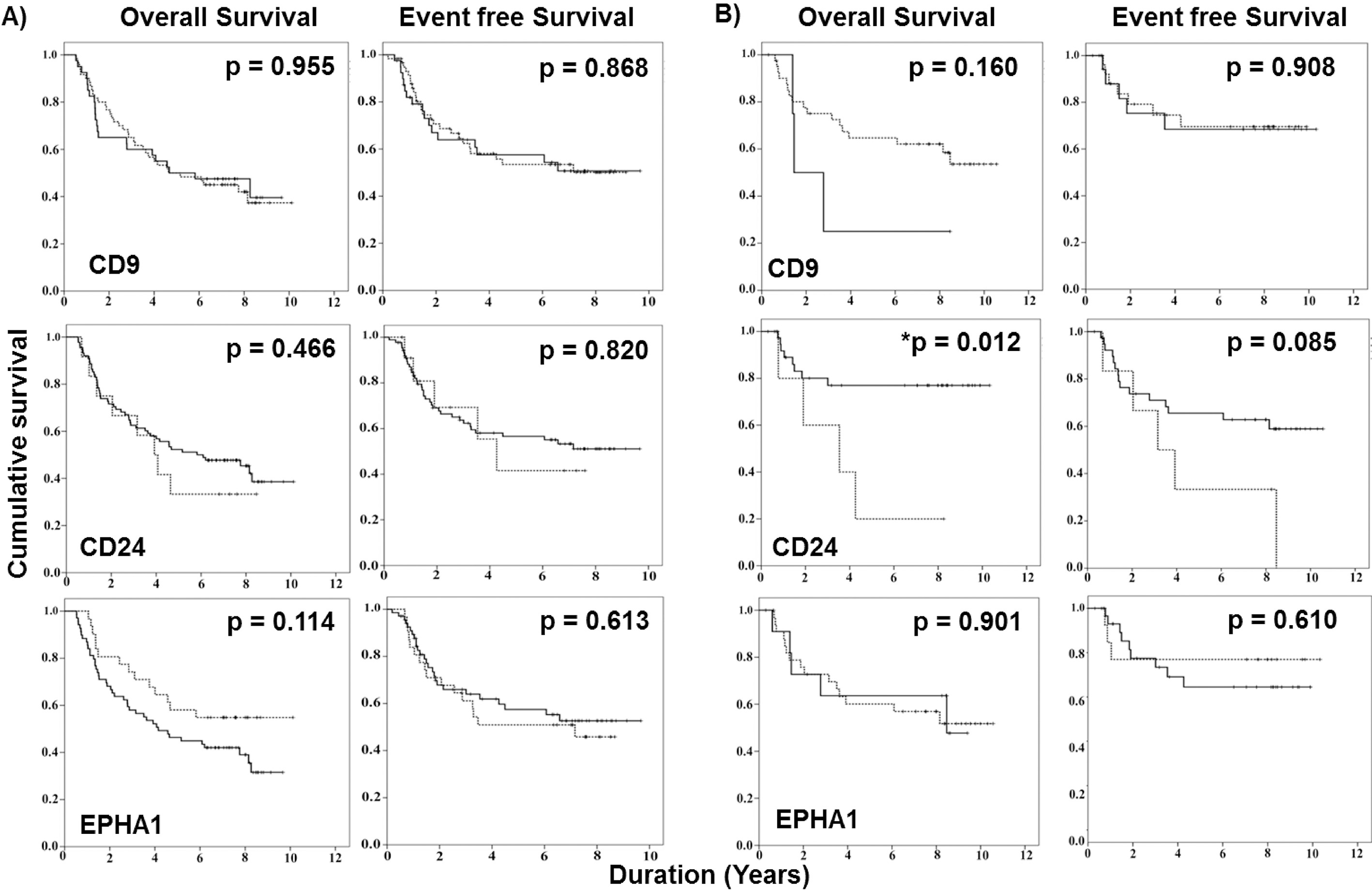
The univariate analysis in patients (
Univariate analysis
Multivariate analysis
The expression of CD9, CD24 and EPHA1 was further evaluated in tissue sections from patients who underwent primary surgery (
Comparative expression of CD24 in paired sections from biopsy and IDS
Among the three new markers, only CD24 showed significant correlation with OS in patients who underwent primary surgery. Therefore, expression of CD24 was further evaluated in paired tumour sections (a diagnostic biopsy and IDS;
Comparative expression of CD24 in paired sections from biopsy and IDS. A. Representative images of CD24 expression in paired sections. H and E staining (left panel), Immunohistochemical staining for CD24 expression in paired biopsy (middle panel) and interval debulking surgery (right panel). B. Expression of CD24 in paired biopsy and IDS sections from all patients (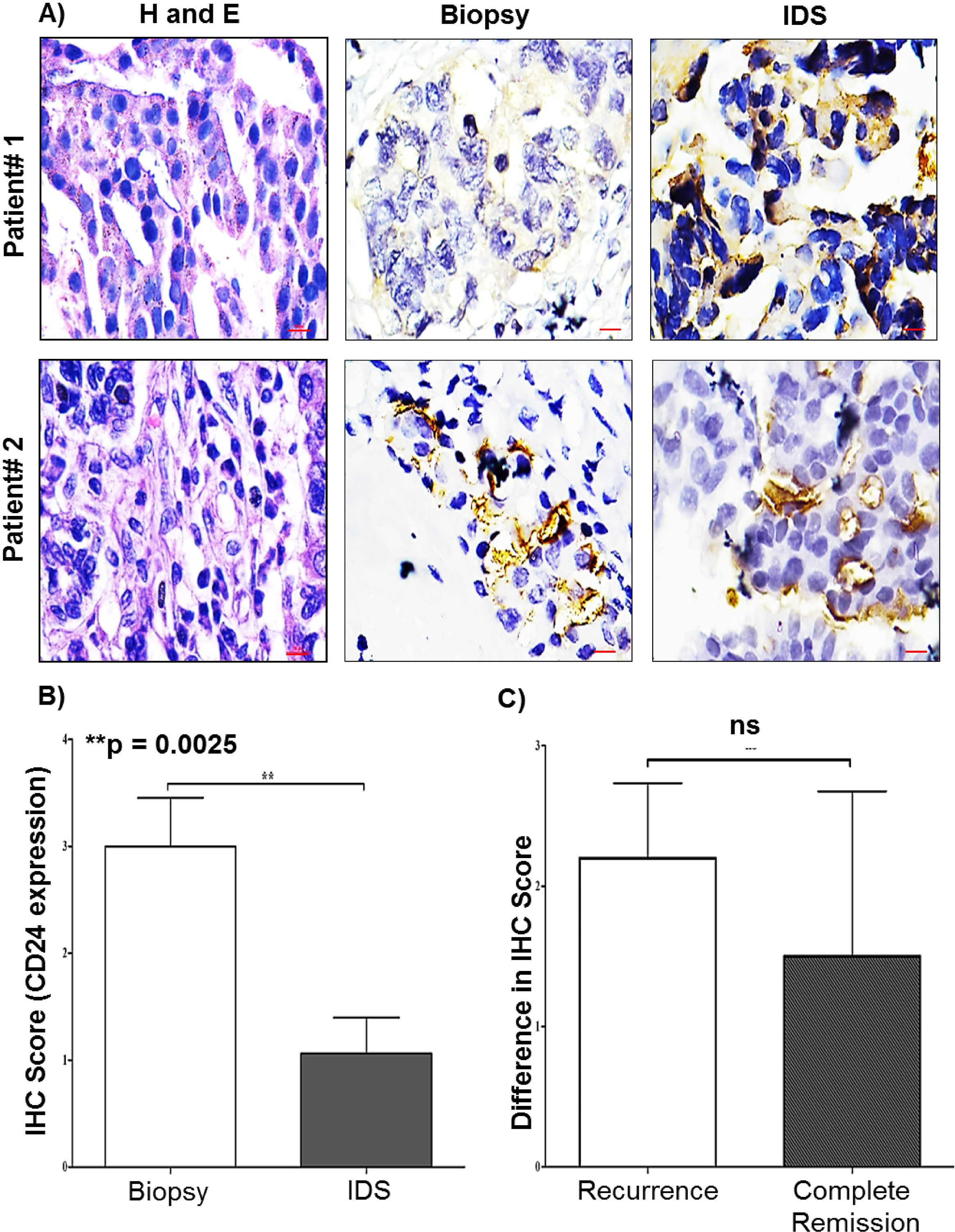
A small population of malignant cells termed as cancer stem cells (CSCs), are thought to be mainly responsible for initiation and maintenance of tumour [2]. These CSCs have been identified consistently using surface markers in different solid tumours like breast, brain, colon and melanoma. Unlike other solid tumours, there has been inconsistency in identifying specific markers for ovarian cancer. Due to this variability it has proved to be challenging to isolate CSCs in ovarian cancer [7]. We have identified new surface markers CD9, CD24 and EPHA1 using publicly available microarray databases. These were the most common genes differentially overexpressed in ovarian cancer when compared with normal ovary and embryonic stem cells [15].
Ovarian cancer is considered to originate from either the ovarian surface epithelium (OSE) or fallopian tube (FT) [16]. It is therefore possible that potential CSC markers are expressed in these locations. To address this question, we evaluated the expression of these new surface markers in normal OSE, FT and ovary sections along with primary tumors from patient specimens.
Microarray data from various laboratories has identified several genes in ovarian cancer with amplification or deletion relative to normal ovarian surface epithelial cells. Among them, CD24 has been found to be highly expressed in the epithelial ovarian cancer [17]. The expression of CD24 was observed in serous as well as endometrioid ovarian cancer subtypes [18]. It is now apparent that CD24 is expressed at high levels in many cancers [19]. CD24 appears to play an important role in metastasis via JAk-2 pathway in ovarian cancer [20]. Further, CD24 has been also shown to promote self-renewal through Nanog mediated by STAT3 phosphorylation that leads to metastasis [21]. Interestingly CD24 is a transcriptional target of hypoxia inhibitory factor and its expression increases in the presence of hypoxia [22].
CD24 is an important molecule for B-cell function and interestingly, it is one of the 30 genes that are expressed in the embryonic stem cells [23]. Ovarian cancer cells identified using CD24 as a marker, have shown stem cell properties like self-renewal, quiescence and resistance to chemotherapy. In assays CD24
On careful scrutiny of the literature, none of the reports have examined the expression of CD24 either in primary tumours or paired samples and correlated with outcome in the context of cancer stem cells. When evaluated in selected number of patients who had undergone surgery as primary treatment (
The expression of CD24 was further evaluated in paired tumour sections (biopsy and IDS). CD24 expression was significantly higher in biopsies as compared to IDS (Fig. 5A and B). This was further reflected in a higher magnitude of difference in patients who have had a recurrence as compared to those in complete remission on follow up. The the magnitude of difference did not correlate significantly with the probability of recurrence (Fig. 5C). This is related to the quantum of CSCs at presentation. This is variable between patients. The level of expression of CSC markers in the initial biopsy or surgical specimen has been the factor that correlated with outcome in many cancers. When paired samples from primary ovarian cancer and recurrent tumours have been examined there has been enrichment for a CSC marker [28, 29].
In this study the expression of CD9 observed in high grade serous ovarian adenocarcinoma (HGSOC) was similar to that obtained from Human Protein Atlas at the RNA level. The expression of CD9 is an adverse prognostic factor in different tumours. However, in gastro-intestinal stromal tumour, over expression was correlated with better survival [30]. In an effort to identify new surface markers in acute lymphoblastic leukemia other than CD34, cells expressing CD9 showed stem cell properties both in vitro and in vivo serial transplantation assays [31]. This is the first report on CD9 as a putative ovarian cancer stem cell marker. CD9 alone was expressed in OSE while FT showed the expression of both CD9 and CD117. We have shown that these cell surface markers were differentially overexpressed in primary tumours when evaluated in a larger cohort of patient specimens (Figs 2 and 3). In contrast to normal ovary, there was higher expression of CD9 (59.40 %) in tumour cells (Table 3) but there was no significant correlation observed with overall survival (
EPHA1 receptor was first isolated from an Erythropoietin producing hepatoma cell line [32]. The increased expression of EPHA1 was observed in advanced ovarian tumours with respect to normal controls [33]. The Eph family plays an important role in signaling of cancer cells and co-expression of ephrin ligands and Eph receptors may be responsible for progression [34]. The altered expression of these receptors contributes to migration and invasion of cancer cells in vitro [35]. High expression of EPHA1 correlated with aggressive tumour type and could be useful for identifying low grade tumours from high grade [36]. We observed low expression of EPHA1 in majority of stage III/IV (68.91 %), high grade (73.52%) and serous sub-type (71.42%) of epithelial ovarian cancer while high EPHA1 expression was observed in only 31 (30.69%) tumours (Table 3). Similarly, reduced expression of EPHA1 correlated with poor clinical outcome in colorectal cancer [37]. Our study is the first to report EPHA1 as a putative cancer stem cell marker in ovarian cancer based on expression of this receptor.
In general, the identification of cell surface markers that target CSCs has to be evaluated in primary tumours. Although, there are well established approaches to prove that a marker targets CSCs in vitro and in vivo, it is more challenging to demonstrate its significance in primary tumours [7]. First, the evaluation of the expression of such a marker in primary tumours by immunohistochemistry is important. However, as this is only semi-quantitative it is difficult to be sure of the proportion of malignant cells that express a particular marker. The evaluation of any CSC marker in primary tumours for expression and correlation with outcome does not definitively prove the clinical relevance. Perhaps the best way is to examine tissue sections from diagnostic biopsies and surgery at recurrence for level of expression of these markers. If indeed, persistence of CSCs leads to recurrence after initial treatment, then the second biopsy should be enriched for the marker [29]. This approach can be evaluated thoroughly for all the tumour types. Ultimately, only by developing treatments that target CSCs and improve survival can the hypothesis be proven.
In conclusion, this report has identified and evaluated 3 new potential CSC markers in ovarian cancer. This data sets the tone for a more detailed evaluation of these markers to delineate their role in the pathogenesis of ovarian cancer.
Footnotes
Acknowledgments
The work is supported by Indian Council for Medical Research (ICMR), Department of Biotechnology (DBT) and University Grant Commission (UGC), Government of India. We are also thankful to Departments of Pathology, Surgical Oncology and Epidemiology, Biostatistics and Cancer Registry.
Conflict of interest
Authors declare no conflict of interest.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/CBM-201463.