
Abstract
BACKGROUND:
Endothelial and platelet activation as well as a disruption of haemostatic balance are crucial in cancer-dependent venous thromboembolism development.
OBJECTIVE:
The aim of this study was to investigate the influence of von Willebrand factor (VWF), sE-selectin, sP-selectin as well as VWF/sE-selectin and sP-selectin/sE-selectin ratios on the probability of disease relapse in invasive breast carcinoma (IBrC) cases.
METHODS:
Eighty-four patients with IA-IIB stage of IBrC who passed a comprehensive clinicopathologic evaluation were included in the study. Follow-up was completed in all patients with a 15.48 % recurrence rate. An immunoassay of VWF antigen, sE-selectin, sP-selectin, as well as an immunohistochemistry of oestrogen and progesterone receptors, human epidermal growth factor receptor 2 (HER2) and Ki67 was performed in all cases.
RESULTS:
The VWF/sE-selectin ratio was significantly higher in patients with poorly differentiated tumours than in those with high-differentiated tumours. A positive correlation between VWF concentration and tumour grade was noted. Eleven of 13 events happened in patients with VWF value below 600 mU/mL with recurrence rate of 25%, but only two events occurred in subject with VWF values above the 600 mU/mL (5%;
CONCLUSIONS:
Our study show that VWF could be considered as a suitable biomarker of breast cancer relapse.
Keywords
Introduction
Breast cancer is one of the primary causes of cancer death in females. It is not a homogenous disease but it covers a group of diseases with specific clinical, histopathological and molecular features. According to the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015 there can be distinguished different intrinsic subtypes of the disease, which include luminal A-like, luminal B-like, HER2-positive and basal-like. Because of the differences in biological features of breast cancers, they are additionally classified as well differentiated (low-grade), moderately differentiated (intermediate-grade) and poorly differentiated (high-grade) using the Elston-Ellis modification of Scarf-Bloom-Richardson grading system. Regarding the stage and molecular determinants, disease management can take different approaches [4].
It is well-established that neoplasm as well as a type of implemented anti-cancer therapy, including surgery procedure, chemotherapy are risk factors for hypercoagulability state. The prevalence of acquired thrombosis in cancer patients is 5-7-fold higher than in non-cancerous individuals [7, 18]. Thus, thrombosis is the second cause of death in hospitalized cancer patients. Importantly, 20% of patients with primary venous thromboembolism (VTE) constitute patients with cancer [7]. The participation in the cancer-related VTE development is attributed to platelets activation and its elevated count, as well as leukocyte count, haemoglobin, d-dimer, tissue factor (TF), soluble form of P-selectin (selectin expressed on platelets and leukocytes), factor VIII, or von Willebrand factor [3]. Additionally, activated platelets promote cancer development and dissemination and are considered as a ‘death mate’ of cancer. These phenomena occur via protection of cancer cells against the immune system and then enabling tumour cells survival in the circulation and by facilitating their adhesion to the endothelial cells (ECs) mediated by selectins [14, 18]. The cancer-dependent thrombocytosis is associated with shortened survival and poor prognosis [26].
Selectins belong to a family of adhesion molecules that mediate interactions between tumour cells, platelets and endothelial cells [14, 21]. P-selectin is a cell adhesion molecule that can be found in the membranes of alpha granules of platelets and the Weibel-Palade bodies of endothelial cells granules. Circulating P-selectin (soluble form of P-selectin) is shedding from damaged or activated platelets or endothelial cells as well as by proteolytic cleavage of the transmembrane protein [3, 15]. Soluble P-selectin is elevated in breast cancer females, further confirming the platelet activation in cancer progression [25]. It has been found that P-selectin deficiency diminishes number of metastasis in a xenographic model of human BrC cells, but it insufficiently abolish them what may suggest a participation of other adhesion molecules in cancer progression [13]. In respect to E-selectin (selectin expressed on endothelial cells) is an adhesion molecule, which is not expressed on the surface of endothelium in quiescent state. However it appears in response to cytokines such as tumour necrosis factor
Interestingly, the principal platelet adhesion ligand, von Willebrand factor, also is involved in cancer growth and progression [1]. In the case of endothelial injury, platelets immediately co-operate with the vessel wall in a glycoprotein (GP) Ib-V-IX-Von Willebrand Factor (VWF)-linked mechanism leading to the platelet adhesion and then aggregation [14]. Several studies suggest that VWF is also associated with angiogenesis, smooth muscle proliferation, and creation of secondary tumour sites [9]. An elevated concentration of plasma VWF is associated with the generation of cancer-related thrombosis, as well as with the degree of malignancy, the rate of metastasis and patients future outcomes [17, 27]. However, an adequate role of VWF in this processes remains unclear and require further elucidation. Since, there are several studies pointing out that VWF exerts antitumor properties, mainly by suppressing angiogenesis and pro-apoptotic effect [16, 20, 24].
The activation of platelets and coagulation process by cancer cells is not just a risk factor for developing thrombosis, but also way that tumour cells promote angiogenesis and metastasis. The inflammatory state in cancer is enhanced by platelets which activate endothelial cells and recruit leukocytes to primary and secondary tumour sites. Thus, the aim of this study was to assess the concentration of VWF, soluble forms of P-selectin and E-selectin in blood of breast cancer patients and their mutual connections in the course of the disease. We also aimed to evaluate of VWF, sP-selectin and sE-selectin as indicators of future prognosis.
Materials and methods
Patient samples
In this study, 84 breast carcinoma patients (mean age of 54.48 years; (interquartile range- IQR: 50–60 years) admitted to Clinical Ward of Breast Cancer and Reconstructive Surgery, Oncology Centre Professor F. Łukaszczyk Memorial Hospital, Bydgoszcz, Poland, from November 2015 to June 2017, were included (Table 1).
Baseline demographic and clinical characteristics of the study population
Baseline demographic and clinical characteristics of the study population
BMI: body mass index, MHT: menopausal hormonal therapy, ER: oestrogen receptor, PR: progesterone receptor, HER-2: human epidermal growth factor receptor 2, Ki-67-proliferation marker.
Study inclusion was carried out by personal interview by an oncologist. Subjects from the study group met the following inclusion criteria: (1) pathologically proven a primary, (2) invasive, (3) unilateral, (4) IA-IIB-stage of breast cancer. The cancer-associated exclusion criteria for all the participants included: (1) carcinoma in situ, (2) tumour larger than 5 cm, (3) stage IIIA or higher, (4) neoadjuvant treatment, (5) locally advanced or metastatic cancer. From the study there were also excluded: (1) males, (2) patients with type 2 diabetes, (3) heart failure, (4) serious liver, lung, kidney, brain and other organ dysfunctions, (5) dyslipidaemia, (6) cerebral-vascular diseases, (7) pre-existing chronic autoimmune or inflammatory disease, (8) recent bleeding or thrombotic events, (9) recent inflammatory or any acute infection. All patients also provided a full history and underwent general clinical examinations.
Ethical approval
The study was approved by the Bioethics Committee Collegium Medicum in Bydgoszcz, the Nicolaus Copernicus University in Toruú, Poland (reference number: KB/547/2015). The study was executed in accordance with the Declaration of Helsinki. Written informed consent was obtained from each patient before enrollment and blood sampling.
Patient follow-up information
Cumulative survival was visualized by Kaplan-Meier graphs. Follow-up was completed in all 84 patients. For the relapse free survival analysis 13 events occurred and follow-up ranged from 21 to 40 months (median follow-up was 33 months) with a 15.48 % recurrence rate. Follow-up times were calculated from the date of the initial visit until the earliest event of interest, i.e. disease spread, death or the last date of contact as of the end of March 2019, and were expressed in months.
Immunohistochemistry (IHC) analysis
The assessment of oestrogen receptor (ER) and progesterone receptor (PR) status, expression of human epidermal growth factor receptor 2 (HER2) and Ki67-proliferation marker took a standard approach and was performed by methods of immunohistochemistry (IHC). The ER and PR status were determined in accordance with the recommendations of the ASCO/CAP using SP1 and 1E2 primary antibodies (Ventana Medical Systems, Tucson, Arizona, USA), respectively. Hormone receptor status was defined as positive if there were at least 1% of tumour cells noted with nuclear staining and negative if the nuclear staining was completely absent. For the semi-quantitative detection of HER2, the rabbit monoclonal primary antibody VENTANA anti-HER2/neu (4B5) was used with a VENTANA aperture for staining the IHC microscopic slide (Benchmark Ultra, Roche-Ventana). HER2 scores were assessed using the standard ASCO/CAP guideline reporting system on a scale of 0, 1
Blood collection and laboratory measurements
Blood samples were intravenously collected from all patients at the time of admission, according to material collection for laboratory tests standards. A total of 9 ml of venous blood was drawn. 4.5 ml for von Willebrand factor assessment was collected in a fasting state into tubes (BD
Enzyme-linked immunosorbent assay (ELISA)
All parameters were performed using the standard immunoassay technique in accordance with the guidelines of the manufacturer. In all assays the reaction mixture was added in a 96-well plate. Serum concentration of sE-selectin was measured using Diaclone SAS, Human ELAM-1, EL-062E-11 test (Diaclone, Besancon Cedex, France), and for sP-selectin: Human sP-selectin (SELP) Cloud-Colne Corp., TX, USA test was used. Citrate plasma concentration of von Willebrand factor were determined applying Imubind
Data analysis
All statistical analyses were conducted using Statistica v. 13.1 (StatStoft
The concentration of von Willebrand factor as well as soluble forms of selectin E and P, VWF/sE-selectin ratio, sP-selectin/sE-selectin ratios depending on demographic, anthropometric determinants as well as lifestyle factors within breast cancer patients group
The concentration of von Willebrand factor as well as soluble forms of selectin E and P, VWF/sE-selectin ratio, sP-selectin/sE-selectin ratios depending on demographic, anthropometric determinants as well as lifestyle factors within breast cancer patients group
VWF: von Willebrand factor; significant differences are denoted by bold
Clinical summarisation of the study population
Table 1 shows the characteristics of the study population. Eighty-four women were included in this study. The median BMI was 26.20 kg/m
The concentration of von Willebrand factor as well as soluble forms of selectin E and P, VWF/sE-selectin, sE-selectin/sP-selectin ratios depending on clinicopathological features within breast cancer patients group
The concentration of von Willebrand factor as well as soluble forms of selectin E and P, VWF/sE-selectin, sE-selectin/sP-selectin ratios depending on clinicopathological features within breast cancer patients group
VWF: von Willebrand factor; other molecular subtype of breast cancer than luminal A: luminal B HER2
In Tables 2 and 3 statistical calculations were presented in the investigation group based on age, body mass index (BMI), menopausal status, smoking habit, arterial hypertension, localisation of the tumour, tumour size and grade, disease stage and molecular subtype of the tumour. In our study group the concentration of sE-selectin was significantly higher in postmenopausal than premenopausal women (
Furthermore Spearman’s Rank correlation analysis pointed a positive correlation between VWF and tumour grade and a negative correlation between VWF and presence of ER in all patients, regardless of nodal status. Moreover a positive correlation between VWF/sE-selectin ratio and histological grade was noted in both groups, but only a negative correlation between VWF/sE-selectin ratio and ER expression in all patients was revealed. Negative correlations between sP-selectin and age as well as between sP-selectin/sE-selectin ratio and age but only in breast cancer cases without nodal involvement were observed (Tables 4 and 5).
Correlations between VWF as well as soluble forms of selectin P and E, VWF/sE-selectin, sP-selectin/sE-selectin ratios and selected clinicopathological parameters in all breast cancer patients (
84)
Correlations between VWF as well as soluble forms of selectin P and E, VWF/sE-selectin, sP-selectin/sE-selectin ratios and selected clinicopathological parameters in all breast cancer patients (
VWF: von Willebrand factor; Ki67: proliferation marker; HER2: human epidermal growth factor receptor 2; ER: oestrogen receptor; PR: progesterone receptor; significant correlations are denoted by bold
Correlations between VWF as well as soluble forms of selectin P and E, VWF/sE-selectin, sP-selectin/sE-selectin ratios and selected clinicopathological parameters in patients with breast cancer without nodal involvement (
VWF: von Willebrand factor; Ki67: proliferation marker; HER2: human epidermal growth factor receptor 2; ER: oestrogen receptor; PR: progesterone receptor; significant correlations are denoted by bold
Kaplan-Meier survival analysis, subgroup analysis of patients in respect to concentration of von Willebrand Factor [plot A- all study cohort (two-subgroups); plot B- all study cohort (three-subgroups); plot C- IBrC cases without nodal involvement (two-subgroups)], concentration of soluble form of selectin E [plot D- all study cohort (two-subgroups); plot E- all study cohort (three-subgroups); plot F- IBrC cases without nodal involvement (two-subgroups)] and concentration of soluble form of selectin P [plot G- all study cohort (two-subgroups); plot H- all study cohort (three-subgroups); plot H- IBrC cases without nodal involvement (two-subgroups)].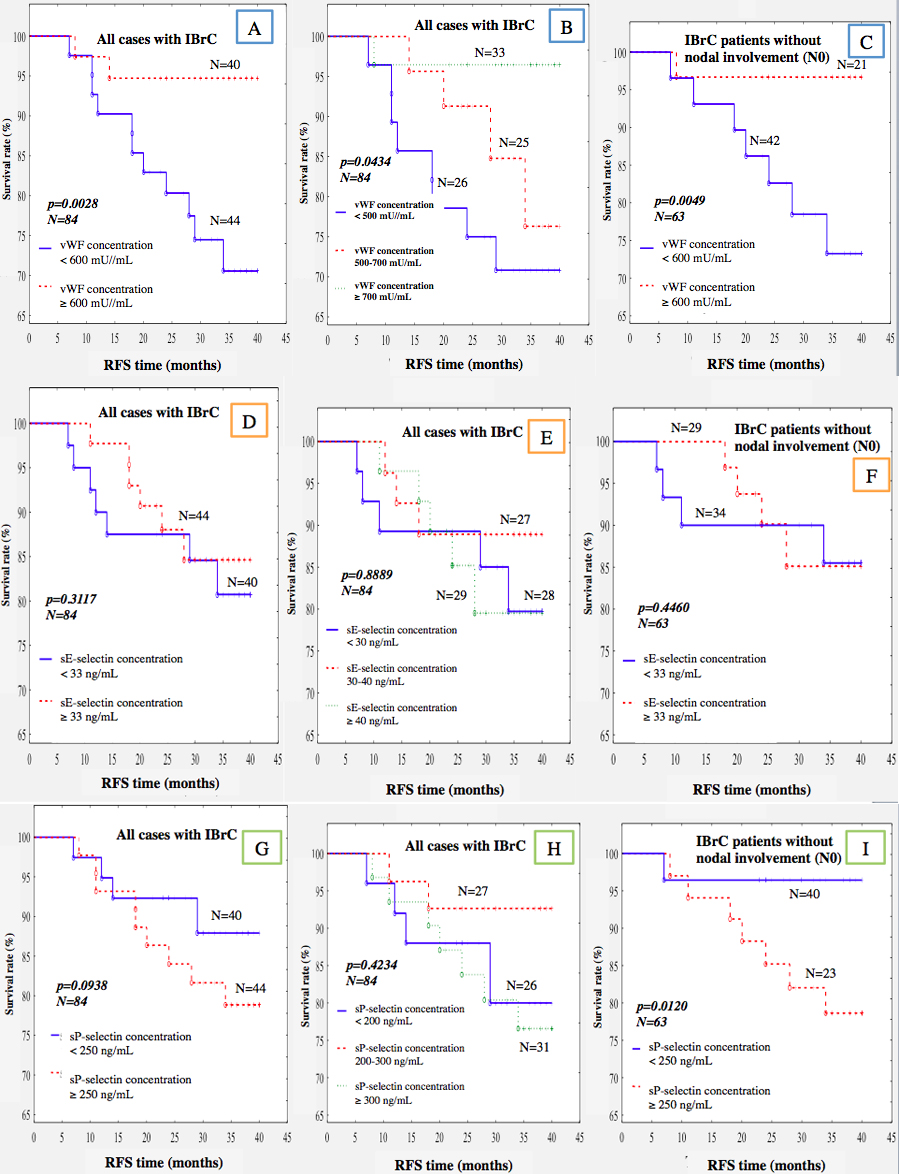
Kaplan-Meier survival analysis, subgroup analysis of patients in respect to von Willebrand Factor/soluble form of selectin E ratio [plot A- all study cohort (two-subgroups); plot B- all study cohort (three-subgroups); plot C- IBrC cases without nodal involvement (two-subgroups)] and soluble form of selectin P/soluble form of selectin E ratio [plot D- all study cohort (two-subgroups); plot E- all study cohort (three-subgroups); plot F- IBrC cases without nodal involvement (two-subgroups)].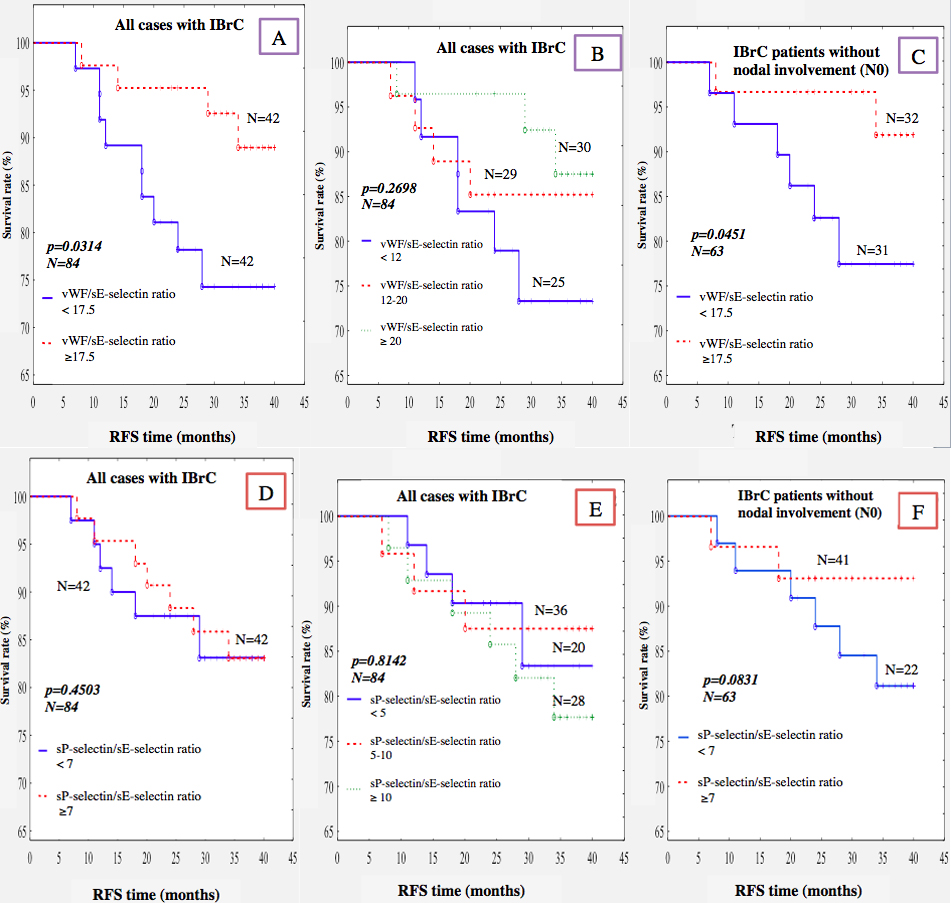
Kaplan-Meier estimates of survival of patients with luminal A and luminal B HER negative IBrC, cohort stratified into 2 strata of each analysed parameter.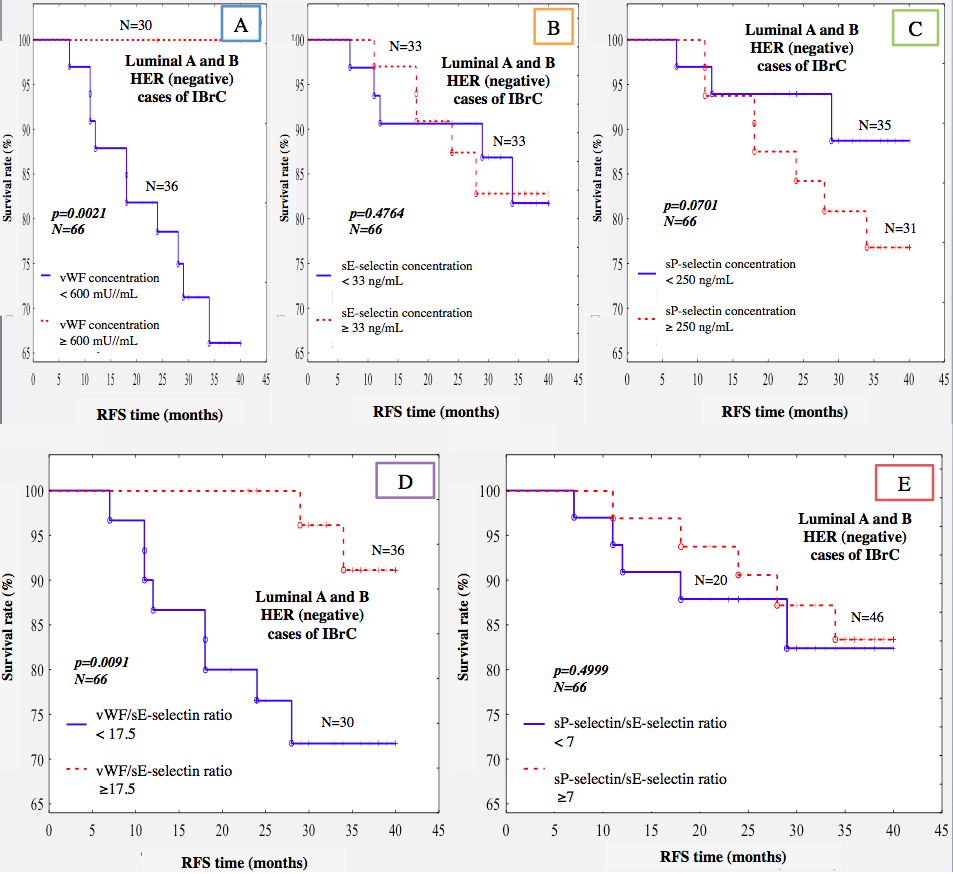
Eighty-four patients were followed-up for a median period of 33 months (ranging from 21 to 40 months). For the relapse-free survival (RFS) analysis, 13 events occurred with a RFS rate of 15.48%. Two (2.4%) patients died during the follow-up period due to systemic metastatic disease (bones, liver and spine metastases). A total of 84 invasive breast cancer (IBrC) patients were divided into 2 (plot A, D, G) or 3 (plot B, E, H) subgroups based on their von Willebrand factor, sE-selectin, sP-selectin levels as well as was performed analysis for IBrC patients without nodal involvement (N0) and those patients were splitted out into 2 subgroups (plot C, F, I). Our analysis indicates that the concentration of VWF is the most suitable prognostic parameter of RFS. VWF demonstrates significance relevance in this aspect, regardless of analysed group. A significantly higher incidence of disease relapse in breast cancer patients with lower than 600 mU/mL baseline concentrations of VWF compared with those with higher concentrations of VWF (
In Fig. 2 we demonstrate 6 plots of examined ratios. We juxtaposed VWF and sE-selectin as well as sP-selectin with sE-selectin due to the fact that all parameters are sensitive biomarkers of endothelial dysfunction. We noted that lower VWF/sE-selectin ratio (
In our study 78.6% of all cases were oestrogen receptor (ER) or progesterone receptor (PR)-positive and HER2 negative, which is in line in epidemiological studies. Thus, we created homogenous group consisting of patients with luminal A and luminal B HER2 negative molecular subtypes. In those patients in the RFS analysis, 10 events happened with a RFS rate of 15.15%. Interestingly, all events occured in cases with lower VWF concentration (
Discussion
In the present study the concentrations of VWF, sE-selectin and sP-selectin as well as VWF/sE-selectin and sP-selectin/sE-selectin ratios were analysed in patients with IBrC to determine whether measured parameters were useful indicators for disease relapse prediction. The results of the present study suggest that the VWF antigen and VWF/sE-selectin ratio are potential biomarkers for future prognosis in IBrC patients. We believe that VWF level is a more useful biomarker than other analysed proteins.
In physiological conditions von Willebrand factor plays a key role in the initiation of platelets adhesion and further aggregation as well as in the secondary haemostasis by binding factor VIII prolonging its half-life in the blood [16]. However its contribution to various processes, such as thrombosis, inflammation, angiogenesis and eventually cancer metastasis cannot be omitted [9]. The VWF disruption in the course of malignant diseases, including leukemias, colorectal cancer, leiomyosarcoma, breast cancer and prostate cancer has been reported [8, 17, 27]. In our study, regardless of analysed subgroup of IBrC the VWF concentration were higher than the normal range (50–150 mU/mL) reported in the general population. Interestingly, a positive correlation between the concentration of VWF and a tumour grade in IBrC subjects was noted, which is in line with Pepin et al. study [17]. The precise mechanism between elevated VWF levels and neoplastic diseases is quite complicated to define, since VWF is an acute phase protein and an endothelial dysfunction marker and its concentration depends on stimulation of sympathetic nervous system, infection, aging process, even a blood type [16, 20]. However, extremely high level of VWF (over 600 mU/mL) as well as a higher vWF/sE-sel ratio than 17.5 were linked to better survival rates in breast cancer patients. The results refer to the whole study group and to women without nodal involvement as well as with luminal A and luminal B HER2- tumours. This observation is consistent with previous study, which demonstrates anti-metastatic role of VWF in experimental mouse model. Terraube et al. observed an increased number of pulmonary metastasis in the absence of VWF. Authors demonstrated that VWF is important agent in protection against tumour cell spread in vivo, interestingly the mechanism of metastasis inhibition and tumour cells death induced by VWF is independent of its function in coagulation [24]. Tigges et al. claim that endothelial VWF deficiency can promote angiogenesis [23]. Also, Stark et al. shown that the absence of VWF enhances angiogenesis. Authors found that inhibition of VWF expression by short interfering RNA (siRNA) in vitro led to in increased integrity of the vessel network via an increased vascular endothelial growth factor receptor type 2- dependent (VEGFR-2) proliferation and migration of endothelial cells. They also observed that neo-angiogenesis and vascularization are enhanced in the VWF-deficient mouse. The capillary tube network was markedly greater in VWF-deficient cells, pointing out that both extracellular and intracellular VWF controls angiogenesis. Stark et al. speculate that elevated VWF levels, as reported in many diseases, may suppress angiogenesis [20]. However, Pepin et al. suggest that high VWF levels are correlated with cancer dissemination [17]. Moreover, Obermeier et al. reported that high VWF levels were independently associated with worse overall survival [10]. Despite of lack of scientific consensus in respect to VWF role in neoplastic diseases; in our study at the end of the observation period of 40 months, 11 of 13 events occured in patients with VWF value below 600 mU/mL with recurrence rate of 25%, but only two events occurred in subject with VWF values above the 600 mU/mL (5%;
Furthermore, according to statistical analysis we observed a higher concentration of sP-selectin in hypertensive patients than non-hypertensive ones as well as a sP-selectin level was negatively associated with the age in the group of IBrC patients without nodal involvement. It is worth a mention that platelet P-selectin has been acknowledged a marker for prediction of thrombosis and angiogenesis in breast cancer. P-selectin not only mediates the adhesion of leukocytes, platelets, and cancer cells during inflammatory processes and thrombosis but also contributes to cancer growth and metastasis. The P-selectin mediates tumour cells dissemination out of the tumour microenvironment by supporting arrest of cancer cells in the circulation and extravasation at distant sites [12]. This is consistent with our results, where lymph node-negative patients shown a shorter recurrence-free survival with higher concentrations of sP-selectin. Furthermore these results suggest activation of platelets even in patients are at early stage of the disease. Based on previous study we suggest, that in the group of IBrC patients with elevated sP-selectin, the higher risk of disease progression or recurrence is associated with massive platelet activation, but also independently with thrombosis development, since elevated level of sP-selectin may strongly predict venous thromboembolic event (VTE) in neoplastic patients [5]. Qi et al. demonstrate that platelets are actively penetrate to solid tumours, including insulinoma and malignant melanoma, via a P-selectin-related pathways, where they release VEGF, and other pro-angiogenic mediators, thereby leading to formation new capillary network and supporting tumour growth [6]. Undoubtedly, elevated level of sP-selectin is negative prognostic indicator. Since, according to our study in patients with sP-selectin above 250 ng/mL, the recurrence rate was 30.43%, whereas IBrC patients with lower sP-selectin
We observed a higher concentration of sE-selectin in post-menopausal subjects in respect to pre-menopausal IBrC cases. Also in patients aged 55 or more and those who were overweight and obese there was a tendency towards a higher concentration of sE-selectin. Ragab et al. observed elevated serum levels of soluble form of E-selectin in patients with breast cancer compared to benign group and compared to their healthy counterparts [11]. Furthermore Kang et al. reported a positive association between a sE-selectin concentration with tumour diameter, grade, stage, molecular subtype and worse survival in breast cancer [22]. During metastatic spread of cancer cells into distant tissues, inflamed endothelium expresses different adhesion molecules, including E-selectin, which most important role is to mediate rolling and vascular adhesion of breast cancer cells and leukocytes [2]. Furthermore circulating form of E-selectin potentiates adhesion and migration of these cells independently from vascular endothelium and facilitate tumour progression and metastasis [22]. The involvement of E-selectin on tumour progression is still unknown. Most likely, the role of E-selectin in tumour cells dissemination is associated with attachment and diapedesis of tumour cells through the vessel wall [2, 22]. Furthermore, we noticed that a higher concentration of sE-selectin at the time of diagnosis were not linked with worse clinical outcome. Our findings deviate from the view of using of sE-selectin as a biomarker for early detection of metastasis for several types of cancer. The applicable value of sE-selectin as a single biomarker may require more accurate consideration, as its concentration may be influenced different factors, hence sE-selectin show a limited practicality in a clinical setting. Thus we suggest to juxtaposition of sE-selectin with second endothelial activity/function biomarker- VWF, since both markers are sensitive on endothelial cells stimulation. In our study the VWF/sE-selectin ratio was significantly higher in patients with grade 3 than in those cases with grade 1 and 2 tumours as well as it correlated positively with tumour grading and negatively with expression of oestrogen receptor. There was also a tendency for higher VWF/sE-selectin ratio in premenopausal women and those who were younger than 55 years old. Furthermore we investigated the prognostic value of VWF/sE-selectin ratio – lower ratio than 17.5 was associated with worse survival rate in the whole study group, as well as in a group of patients without nodal involvement and in a group of patients with luminal A or B HER2- subtype of breast cancer (recurrence rate: 21.43%, 19.35%, 26.67%, respectively).
The present study has several limitations, including a short observation period and quite small sample size. Breast cancer patients have been in peri-menopausal period, which is associated with age-related comorbidities including weight gain, elevation in blood pressure or hormone imbalance, which may impact on the VWF, sE-selectin and P-selectin levels.
Our study demonstrates that VWF could be considered as an accurate and specific biomarker of breast cancer relapse, regardless of analysed subgroup. However, we claim that should be established a cut-off value for VWF concentration to consider the degree of its elevation. We propose, that the sP-selectin concentration over 250 ng/mL is connected with the higher risk of disease progression. A soluble form of E-selectin does not present any essential value in malignancy disease prediction. We believe that VWF/sE-selectin ratio is a more suitable indicator of tumour progression and spread than a sE-selectin as a single parameter.
Footnotes
Acknowledgments
We would like to thank all of the patients for participating in our study.
Conflict of interest
The authors have declared that no competing interests exist.