
Abstract
A deficiency and/or dysfunction of von Willebrand factor (VWF) or factor VIII (FVIII) results in the bleeding disorders of von Willebrand disease (VWD) and hemophilia A (HA), respectively. Whereas HA impacts coagulation, VWD primarily impairs hemostasis through defective platelet adhesion and aggregation. In addition, because VWF protects FVIII from proteolytic degradation, a deficiency in VWF can also reduce FVIII levels and affect coagulation. While regular prophylaxis to restore FVIII activity is the standard of care for severe HA, its use to correct the dual VWF/FVIII defect in severe VWD is less well established. Current treatment guidelines suggest the use of long-term prophylaxis rather than no prophylaxis in persons with VWD with a history of severe and frequent bleeds. In this narrative review, we discuss the barriers to the broader adoption of prophylaxis in persons with severe VWD and results of recent clinical studies that provide further evidence to support its use. A growing body of evidence suggests that prophylaxis should be established as the standard care for individuals with severe VWD and recurrent bleeding.
Keywords
Introduction
Von Willebrand factor (VWF) and coagulation factor VIII (FVIII) circulate in the bloodstream as a complex and both play a crucial role in hemostasis.1–5 At the site of endothelial injury, VWF and FVIII dissociate to contribute to primary and secondary hemostasis, respectively.1,2 During primary hemostasis, VWF promotes platelet adhesion, aggregation, and subsequent formation of the initial platelet plug.3,4 During secondary hemostasis, FVIII promotes the synthesis of insoluble fibrin, thereby strengthening and further stabilizing the blood clot.1,5 Because FVIII is protected from proteolytic degradation by its natural binding to VWF, a deficiency in VWF can also cause a decrease in FVIII levels, indirectly affecting secondary hemostasis. 1
Deficiency and/or dysfunction of VWF or FVIII results in von Willebrand disease (VWD) and hemophilia A (HA), respectively.1,6–8 Treatment of VWD and HA shares the common goal of correcting the underlying factor deficiencies,6–8 which can be achieved through regular replacement therapy with either plasma-derived or recombinant factor concentrates.6–9 In persons with milder forms of VWD or HA, treatment is usually administered on an as-needed (on-demand) basis to treat acute bleeding events or to provide hemostatic coverage for challenges such as surgery or medical procedures.6–8
Regular prophylaxis to restore and maintain a minimum FVIII activity and prevent bleeding, particularly into the muscles and joints, is the standard of care in persons with severe HA or a severe bleeding phenotype. 8 Prophylaxis in HA is supported by many years of clinical experience and robust efficacy and safety data from multiple clinical trials as well as established FVIII trough level targets.8,10–12 Several plasma-derived FVIII (pdFVIII) and recombinant FVIII (rFVIII) products are currently approved for HA prophylaxis. In the last decade, new rFVIII products have become available, including concentrates derived from human cell lines and extended half-life products.11,12 Non-factor therapies, administered subcutaneously, such as the FVIII mimetic emicizumab, 13 anti-tissue factor pathway inhibitors (marstacimab 14 and concizumab 15 ) and an antithrombin-targeting small interfering RNA (fitusiran 16 ) have also been approved for prophylaxis in persons with HA. In addition, gene therapy (valoctocogene roxaparvovec) is now licensed for the treatment of adults with severe HA in certain regions of the world. 17 According to the American Thrombosis and Hemostasis Network, 83% of persons with severe HA in the United States receive prophylaxis. 18 Indeed, the HA community has moved beyond debating the need for primary, secondary, or tertiary prophylaxis to focusing on how to best individualize treatment strategies and improve health-related quality of life (HR-QoL).8,19,20
VWD is associated with a significant health burden due to its increased bleeding risk, negative impact on QoL, and high healthcare resource utilization.21,22 Current treatment guidelines for VWD suggest the use of long-term prophylaxis rather than no prophylaxis in persons with VWD with a history of severe and frequent bleeds. 23 However, regular prophylaxis to correct the dual VWF/FVIII defect in persons with severe VWD is less widely adopted.6,9 In contrast to severe HA, VWF replacement treatment options for prophylaxis in severe VWD are currently limited to replacement therapy using VWF-containing products administered by intravenous infusion. International guidelines, published in 2021, recommend the use of long-term prophylaxis in persons with VWD who have a history of severe and frequent bleeds. 23
In this narrative review, we identify some of the potential barriers to the adequate implementation of prophylaxis in severe VWD based on our collective clinical experience and review published clinical data supporting its use,24–31 with a focus on the results from VWD-specific studies investigating the efficacy of prophylaxis with recombinant VWF (rVWF, Vonvendi) 28 and a plasma derived (pd)VWF/FVIII concentrate (wilate), 30 conducted after the publication of the international guidelines. 23 This review was guided by the Scale for the Assessment of Narrative Review Articles (SANRA). 32
Barriers to the use of prophylaxis in severe VWD
Defining and identifying severe VWD
The classification of VWD severity is more complex than in HA, where severity is classified according to residual plasma FVIII activity (FVIII:C) levels as mild (>5 to <40 IU/dL), moderate (1–5 IU/dL), or severe (<1 IU/dL).8,33 Residual FVIII levels closely correlate with the risk of bleeding in men, 8 although some individuals, including women, with non-severe HA (FVIII:C ⩾1 IU/dL) may also present with severe bleeding phenotypes and require prophylaxis. 8 In contrast, VWD is classified into three main types according to either quantitative or qualitative VWF deficiencies.7,34,35 Type 1, the most common form of VWD (~70%–80% of cases), is characterized by a partial quantitative VWF deficiency and is further subdivided into subtype 1C depending upon VWF half-life; type 2 (~20% of cases) is caused by qualitative abnormalities of VWF and is further subdivided into subtypes 2A, 2B, 2M, and 2N depending on the specific VWF functional abnormality. Finally, type 3 (<5% of cases) is characterized by a virtual absence of VWF and consequently very low FVIII levels.7,34,35
In the United States, 24,508 persons with HA receive treatment at specialized hemophilia treatment centers (HTCs) with 10,046 (41%) of them having severe disease (FVIII:C <1 IU/dL 36 ; Figure 1(a)). The number of persons with VWD treated at the HTCs is 35,466, of whom 27,641 (77.9%) have type 1, 3808 (10.7%) type 2, and 531 (1.5%) type 3 36 (Figure 1(b)). However, the true numbers of persons affected by HA and VWD are likely to be considerably higher. The World Federation of Hemophilia (WFH) estimates that >75% of persons with HA and up to 90% of those with VWD are currently undiagnosed, worldwide.37,38 Based on available data, approximately half of all persons with HA can be expected to have severe disease whereas most persons with VWD are expected to have non-severe disease.

Disease classification of persons treated at US hemophilia treatment centers between January 1, 2012, through March 31, 2024. (a) Hemophilia A by severity, (b) VWD by VWD type, (c) sex distribution by VWD type, and (d) sex distribution in HA severity. 36
Owing to its autosomal inheritance pattern, men and women are equally likely to inherit VWD, although more women are diagnosed with VWD 36 (Figure 1(c)). This discrepancy is due to the presence of recurrent female-specific reproductive tract VWD bleeding symptoms such as heavy menstrual bleeding (HMB) and bleeding associated with pregnancy and childbirth. 39 In contrast, owing to its X-linked inheritance pattern, HA affects all XY men,6,8,40 while XX women can be affected by bleeding and/or low FVIII levels. 41 Affected XX women usually have FVIII deficiencies in the mild range (FVIII:C >5 and <40 IU/dL) 42 and currently account for <1% of persons with severe HA treated at HTCs in the United States (Figure 1(d)).36,42
Although type 1 VWD is considered to be a milder form of VWD and type 3 is considered the most severe,7,34 the clinical severity of VWD varies considerably between and within VWD types. 43 The difficulty in classifying VWD disease severity is exemplified by the wide range of definitions used in different clinical trials (Table 1).43–50 A recent Delphi exercise 51 was undertaken with the aim of developing a consensus definition of severe VWD. 50 The Delphi panel agreed that most (but not all) persons with type 3, many type 2, and some type 1 might have severe VWD. The consensus definition for severe VWD resulting from the Delphi exercise was as follows: (A) anyone meeting the diagnostic classification for VWD and (B) any VWF antigen or activity <20 or <30 IU/dL with excessive bleeding symptoms: (1) bleeding that results in hospitalization, requires a surgical procedure; packed red blood cell blood transfusion, hemoglobin decrease >2 g/dL, or (2) intracranial, intraspinal, intramuscular with compartment syndrome, or (3) persistent or recurrent bleeding that is disruptive of regular functioning. 50
Definitions of VWD severity.

Desmopressin can be used for short-term treatment of many persons with type 1 VWD and some persons with type 2 VWD, except type 2B VWD patients in whom it is generally contraindicated, and it is ineffective in persons with type 3 VWD.1,6,23
Except type 2N.
In persons on prior on-demand therapy.
BE, bleeding episode; FVIII:C, factor VIII activity; GI, gastrointestinal; PBAC, pictorial blood assessment chart; PRBC, packed red blood cell; VWD-PN, VWD Prophylaxis Network; VWF:Ag, VWF antigen; VWF:RCo, VWF ristocetin cofactor activity; WiN, Willebrand in the Netherlands.
The use of bleeding assessment tools (BATs) is recommended in the diagnosis of VWD 52 and could play an important role in defining and identifying severe VWD. International Society on Thrombosis and Haemostasis (ISTH) BAT scores have been shown to correlate with the type of VWD; higher ISTH BAT scores have been recorded in type 3 VWD than in type 2 or type 1, and in persons with VWF levels <10 U/dL compared with VWF levels of 10–30 U/dL. 53
Delays in the diagnosis of VWD
VWD is often underdiagnosed or misdiagnosed in symptomatic persons, which delays optimal treatment of VWD-associated bleeding symptoms.54–56 This can be attributed in part to a lack of disease awareness and the complexity of clinical and laboratory assessment of VWD.55–58 Diagnostic delay is common in VWD and more so in women, 59 which may reflect the persistent barrier of sexism in the treatment of bleeding disorders. 60 VWD is diagnosed approximately 6 years later in women than in men (22.5 years vs 16.6 years) and the diagnostic delay is estimated to be approximately 4 years longer in women than in men (11.6 years vs 7.7 years). 59 In contrast, severe HA is usually diagnosed early in life and regular prophylaxis is recommended from an early age prior to establishment of joint disease.8,61 Children with severe HA usually gain experience with regular infusions that started in childhood, which is not currently the case in VWD. The diverse bleeding symptoms of VWD may also contribute to diagnostic delays. In contrast to severe HA, which is characterized by muscle and joints bleeds, 8 VWD is often characterized by excessive and recurrent mucocutaneous bleeding, such as epistaxis, oropharyngeal bleeds, gastrointestinal bleeding, HMB, and postpartum hemorrhage in women,6,7,56 although joint bleeding can occur with VWD. 62 In clinical studies of persons with VWD and severe bleeding who received on-demand treatment, bleeding symptoms mainly affected the nose and oral mucosa, and less frequently the joints (Figure 2(a)), whereas joint bleeds predominate in persons with severe HA (Figure 2(b)). As the typical symptoms of VWD (e.g., epistaxis) are common in the general population or are physiological in the case of reproductive tract-specific VWD bleeding symptoms, these symptoms are not specific to VWD and may be normalized in families with VWD and therefore likely contribute to the diagnostic delay.

Under recognition of VWD-specific disease burden
Compared with the general population, persons with VWD have poorer HR-QoL and higher resource utilization.21,22 A population-based case-control study reported a twofold increase in the rate of outpatient visits and hospitalizations in persons with VWD compared with age- and sex-matched controls. 63 Epistaxis and HMB were the most common causes of outpatient visits, and gastrointestinal bleeding was the most common cause of hospitalization. 63 Frequent and severe nosebleeds can lead to the development of iron deficiency anemia (IDA) and a potential need for blood transfusions or recurrent oral or intravenous iron replacement. 64 HMB occurs in ⩾80% of women with VWD 65 and affects women with moderate or severe VWF deficiencies across all VWD types. 66 The presence of HMB is also associated with a significant increased risk for IDA, 67 blood transfusion, 66 hospitalization, 63 reduced HR-QoL, 68 and interference with social, school, and work activities. 69 Furthermore, women with VWD have an increased risk for bleeding during pregnancy and delivery.70–74 Additionally, the incidence of anxiety and depression is considerably higher in persons with VWD (54%–64%) compared with the general population (6%–7%). 75
The burden of VWD-related bleeding symptoms is generally considered to be lower than the burden of joint bleeding associated with severe HA for which prophylaxis is the standard of care. 8 Although VWD may be clinically mild in many cases, the seriousness of the disease may be under recognized, particularly in persons with a more severe condition 76 and in women who have bleeding symptoms.77,78 In studies investigating the use of prophylaxis versus on-demand treatment, the total annualized bleeding rates (ABRs) during on-demand treatment appear to be slightly higher in HA (ABRs of 31–58)79–81 than in VWD (ABR of 13–33),25,30 although the ABRs in persons with severe VWD were still significant. It is important to note that there are limitations in comparing ABRs in VWD and HA. For example, defining a bleeding event in the setting of HMB can be more challenging than defining a joint bleed in HA because regular bleeding symptoms related to menstruation are expected but joint bleeds are not.
Data from the Willebrand in the Netherlands (WiN) study showed that HR-QoL is lower in persons with moderate and severe VWD compared to the general population, and this HR-QoL was strongly associated with the observed severity of their bleeding phenotype. 82 Further data from the WiN study showed that hemophilia-like joint bleeding and arthropathy can also occur in persons with moderate or severe VWD.62,83 Joint bleeds were reported with 22% of those with type 1, 21% with type 2, and 47% of those with type 3. 62 A case-control study, analyzing the same cohort, reported that arthropathy was present in 40% of persons with VWD who had a history of joint bleeds. 83 This complication was associated with chronic joint pain, radiological abnormalities, functional limitations, and reduced social participation. 83 In a separate analysis, joint outcomes were compared for persons with moderate or severe VWD versus persons with moderate or severe HA. 84 Joint outcomes were similar in persons with moderate or severe VWD and moderate HA, and between persons with type 3 VWD and severe HA. 84
VWD represents a significant burden for persons with VWD and their families. For example, a nationwide Swedish study of caregivers of children with more severe forms of VWD reported that caregivers’ QoL was significantly affected by their child’s VWD diagnosis. 85 High rates of school absenteeism, limitations in physical activity, and financial impact were also reported. 85
Although the burden of VWD is increasingly recognized, a greater awareness and recognition of this burden will undoubtedly facilitate the wider adoption of prophylaxis in VWD.
Efficacy and safety, HR-QoL, hospitalizations, and resource use
Clinical studies investigating the efficacy of prophylaxis in persons with severe VWD
Guidelines of the American Society of Hematology (ASH), the ISTH, the National Hemophilia Foundation (NHF), and the WFH, published in 2021, recommend the use of long-term prophylaxis in persons with VWD who have a history of severe and frequent bleeds. 23 Although the exact definitions of severity or bleeding frequency were not provided, it is important to highlight that this recommendation did not specify whether prophylaxis should be restricted to a particular type of VWD or within a certain range of VWF activity level. 23 The panel also called for further studies to investigate the use of prophylaxis for women with VWD and HMB. 23
Since the cut-off date (October 2019) for the ASH/ISTH/NHF/WFH guidelines, 86 results of several, prospective, non-randomized observational,24,26,27,31 and interventional25,28–30 studies investigating prophylaxis with VWF concentrates have been published (Table 2).
Studies reporting ABRs during long-term prophylaxis in persons with VWD published after the ASH/ISTH/NHF/WFH 23 cut-off date.

Median or median (range) or range.
Dose refers to IU/kg VWF:RCo.
Estimate from 43.5 IU/kg per infusion twice weekly.
Estimate from 42.8 IU/kg per infusion once (n = 4), 2–3 times (n = 3) or 3 times (n = 2) per week or 1–2 times per month (n = 1).
Mean value; median values were not reported.
In persons on prior on-demand treatment.
In persons on prior prophylaxis.
Data for all bleeds (treated and untreated).
WIL-31 is the only prophylaxis study in VWD with a prospective on-demand run-in study as an intra-individual comparator.
ABR, annualized bleeding rate; ASH, American Society of Hematology; BE, bleeding episode; ED, exposure day; ENT, ear, nose, and throat; GI, gastrointestinal; ISTH, International Society on Thrombosis and Haemostasis; IU, international unit(s); NHF, National Hemophilia Foundation; NR, not reported; SABR, spontaneous annualized bleeding rate; TABR, total annualized bleeding rate; VWD, von Willebrand disease; WFH, World Federation of Hemophilia.
In a prospective, observational, post-marketing study using Wilfactin, a pdVWF almost devoid of FVIII, the median total ABR (TABR) was 1.0 in 20 persons who received prophylaxis for ⩾12 months (prior TABR was not reported). 24 In an observational study with Voncento, a 2.4:1 pdVWF/FVIII, the median TABR was reduced from 1 to 0.3 in 19 persons on prior prophylaxis with other concentrates. 27 In a different post-marketing study with Voncento in persons with severe VWD, median TABR for treated non-surgical bleeds in 14 persons on prophylaxis was 4.4. 31 In another study with Voncento, those on prophylaxis (n = 10) experienced a median of 4.4 non-surgical bleeds per year compared with 12.7 in those persons treated on-demand (n = 7). 25 In an observational, prospective, phase IV, post-marketing study with wilate, a 1:1 pdVWF/FVIII, median TABR was 1.9 compared with 12 prior to the study in 25 persons on prophylaxis. 26 In a case report of a 12-year-old boy with type 3 VWD who experienced frequent bleeding while receiving prophylaxis with Wilfactin and FVIII (Factane), switching to wilate prophylaxis reduced the TABR by 73% (7.5 vs 2) and spontaneous ABR (SABR) by 83% (3 vs 0.5). 87
Leebeek et al. 28 published the first evidence supporting the efficacy of rVWF (Vonvendi) prophylaxis in a prospective, 12-month, phase III study in adults with severe VWD, defined as VWF:RCo <20 IU/dL. Persons with ⩾3 documented spontaneous bleeding episodes (not including menorrhagia) requiring VWF therapy in the past year (prior on-demand group) or persons receiving pdVWF prophylaxis (switch group) were eligible for this study. The study included 13 participants in the “prior on-demand group” and 10 in the “switch group,” 78% of whom had type 3 VWD. The median weekly prophylactic dose of Vonvendi was 96 and 107 IU/kg in the “prior on-demand” and “switch” groups, respectively. All the participants in the “prior on-demand group,” and 8 (80%) of participants in the “switch group,” were on a twice-weekly regimen. ABRs during prophylaxis were compared with historical bleed data derived from medical records. In the “prior on-demand group,” the model-based mean TABR was reduced by 46% from 5.1 to 2.7 and SABR was reduced by 57% from 4.9 to 2.1. 29 Despite this trial having some limitations (non-randomized, non-comparative design, collection of historical bleeding data from medical records, small sample size), these results led to US FDA approval of rVWF (Vonvendi) for prophylaxis in adults with VWD. 88
The WIL-31 study is currently the largest prospective prophylaxis study in VWD with an on-demand run-in study as an intra-individual comparator. 30 This was a 12-month, prospective, phase III study that evaluated the efficacy of wilate prophylaxis in 33 participants with severe VWD. It was preceded by a 6-month prospective run-in study (WIL-29) during which participants received on-demand treatment with any available VWF concentrate. Participants with type 3, type 2 (except 2N), or severe type 1 VWD (VWF:RCo <30 IU/dL) were eligible for the study if they had experienced ⩾6 bleeding episodes during WIL-29 (excluding menstrual bleeds), of which ⩾2 were treated with a VWF-containing product. The median weekly prophylactic dose of wilate was 58 IU/kg, with 70% of participants on a twice-weekly regimen at the end of the study. The mean TABR decreased by 84% from 33.4 during on-demand treatment to 5.2 during prophylaxis. Similarly, the mean SABR decreased by 87% from 24.4 during on-demand treatment to 3.2 during prophylaxis. Reductions in ABRs were seen across all age groups, in men and women, and across VWD types (Figure 3). 30 Despite this trial having some limitations (non-randomized, non-controlled open-label design, small sample size), the results of this study led to the US FDA approval of wilate for prophylaxis in individuals ⩾6 years with all types of VWD. 89
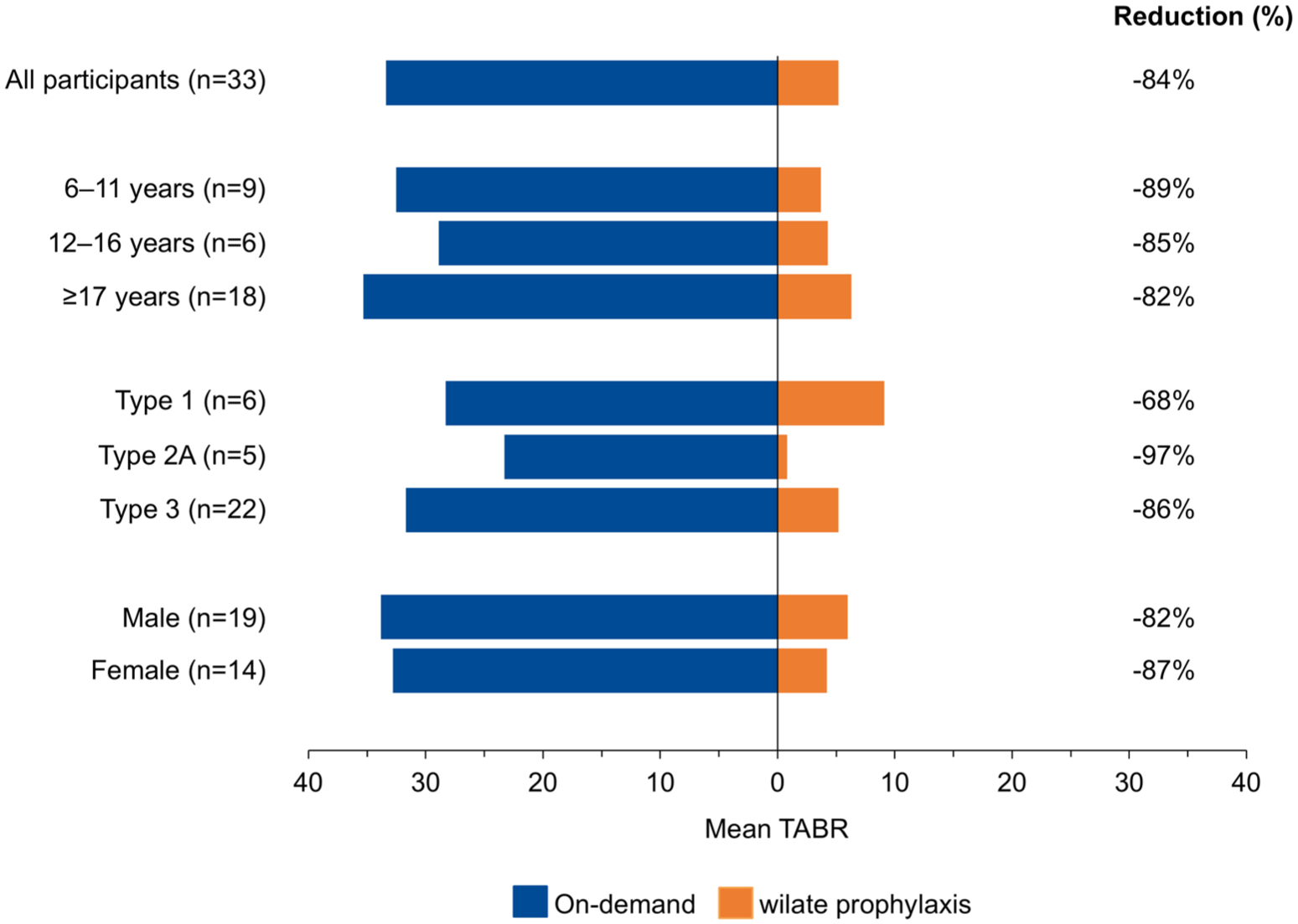
TABRs for wilate during on-demand treatment (WIL-29) and during prophylaxis (WIL-31). 30
The WIL-31 study 30 is the only prophylaxis study published after the ASH/ISTH/NHF/WFH guidelines24–30 to separately report data on HMB, although the sample size was small. In five participants, mean intra-individual heavy menstrual ABR was reduced by 74% from 9.7 to 2.4. 90 All the menstrual bleeds during prophylaxis occurred in two participants with concomitant comorbidities that may have affected their menstrual health (polycystic ovaries in one participant, and hypothyroidism, obesity, anemia, type 2 diabetes, and hypertension in another). In four participants with available pictorial blood loss assessment chart (PBAC) scores, including the two participants with comorbidities, median scores decreased by 43% from 227 during on-demand treatment to 131 during prophylaxis. 90
The VWDMin study, a phase III, open-label, randomized crossover trial, compared the effect of rVWF (Vonvendi) versus tranexamic acid on HMB in persons with mild or moderate VWD. 91 Participants were randomly assigned (1:1) to Vonvendi, 40 IU/kg on day 1 of the menstrual cycle, or tranexamic acid 1300 mg three times daily on days 1–5 of the menstrual cycle. The primary outcome measure was the amount of blood loss during each cycle, which was determined using PBAC scores. The findings showed significantly lower PBAC scores with tranexamic acid compared with rVWF (146 vs 213; p = 0.039). The authors concluded that rVWF was not superior to tranexamic acid in reducing HMB in this study, and that tranexamic acid was less costly. 91 The VWDMin study had some limitations. The target number for inclusion was not reached, and the study was stopped after inclusion of 36 of the 60 individuals planned. This limited the validity of the study results, especially given the well-known variability in PBAC scores over time in persons with VWD. Other limitations were the inclusion of only persons with mild and moderate VWD, no persons with type 3 VWD were included, the absence of a clear target VWF level, treatment was not given prior to menstruation, and rVWF was only administered on day 1 of the menstrual cycle. 91
Safety of prophylaxis in persons with VWD
Many years of clinical experience with VWF concentrates in on-demand treatment for acute bleeding episodes and short-term surgical prophylaxis in persons with VWD have demonstrated that VWF concentrates are well tolerated.92–98 Hypersensitivity, immunogenicity, and thromboembolic risk are considered adverse events of special interest in the management of VWD as is the case for HA.
While allergic-type hypersensitivity reactions are possible with VWF concentrates, reported incidence rates of hypersensitivity in post-marketing surveillance were 1 case per 14,788 doses of Voncento 97 and 1 case per 23,636 doses of Humate-P. 98
In contrast to FVIII inhibitors,99,100 development of VWF inhibitors in persons with VWD is less common and it mainly occurs in persons with type 3 VWD. 101 VWF genotype is a risk for VWF inhibitors, with genotypes that include a deletion posing the highest risk. 102 The 3WINTERS study reported an anti-VWF inhibitor frequency of 8.4% in a cohort of 213 persons with type 3 VWD and a possible association with anaphylactic reactions. 103 This finding underscores the importance of careful monitoring for all persons receiving regular VWF treatment. Reported incidence rates of VWF inhibitors for Voncento 97 and Humate-P 98 in post-marketing surveillance were 1 case per 916,875 doses and 1 case per 92,857 doses, respectively.
Supraphysiologic levels of both VWF and FVIII are associated with an increased thromboembolic risk.104–107 When using VWF concentrates there is the potential for thromboembolic events, especially in situations where repeated high doses are required, such as during perioperative prophylaxis. Reported incidences of thromboembolism with VWF concentrates have been rare and mainly in a surgical setting.108–111 An analysis of two studies of Humate-P found that supraphysiologic levels of VWF and FVIII were recorded in most persons during surgery. 110 In one study, 111 VWF:RCo and/or FVIII activity ⩾150% was observed at least once in 29 of the 35 individuals, yet no venous thromboembolic events occurred. In the other study, 112 VWF and/or FVIII activity ⩾150% was observed at least once in 24 of 27 individuals who underwent surgery and 2 individuals had postoperative venous thromboembolic events: a mild thrombophlebitis of the lower leg (FVIII:C not reported) and pulmonary embolism (FVIII:C 450 IU/dL). The reported incidence rates of thromboembolic events for Voncento and Humate-P in post-marketing surveillance were 1 case per 183,375 doses 97 and 1 case per 78,787 doses, 98 respectively. In the prophylaxis setting, the doses administered would not be expected to significantly elevate VWF and/or FVIII levels above normal levels. In the WIL-31 study, analysis of FVIII and VWF levels over time during wilate prophylaxis confirmed that there was no accumulation. 30
The ASH/ISTH/NHF/WFH analysis of PRO.WILL data concluded that prophylaxis may increase the risk of serious adverse events (SAEs) compared with on-demand treatment49,86 because of one SAE (intestinal perforation) reported in the prophylaxis arm and none in the on-demand arm.49,86 However, this SAE was not considered to be treatment-related. 49 Otherwise, no SAEs were reported during prophylaxis in five observational studies analyzed by the ASH/ISTH/NHF/WFH. 86 Furthermore, no treatment-related SAEs were reported in studies with VWF concentrates published after the ASH/ISTH/NHF/WFH cut-off date.24–31 Safety data from these studies indicate that prophylaxis with VWF concentrates is well tolerated and there were no reports of VWF or FVIII inhibitor development.24–31 There was a single reported case of thromboembolism (purpura) in a participant receiving rVWF prophylaxis,28,29 but no cases of thromboembolism were reported in studies of prophylaxis using pdVWF/FVIII.24–27,30,31
Prophylaxis effect on HR-QoL, hospitalizations, and resource use
Although the clinical studies of prophylaxis in persons with severe VWD did not report data on HR-QoL changes, the observed reduction in bleeding rates, as well as the potential reduction in the fear of bleeding when on prophylaxis, would be expected to positively impact HR-QoL. It is important to recognize that not only life-threatening bleeds, but all VWD-related bleeds, can significantly impact a person’s life by limiting daily activities, including missed days of school or work, reduced social and physical activity, and increased anxiety and depression.75,82,113,114
Data on hospitalizations and resource use for severe VWD are sparse. One analysis of clinical trial data showed that prophylaxis significantly reduced the incidence of hospitalizations in 105 persons with clinically severe VWD (712 vs 448 events per 1000 person years). 63 Two analyses115,116 have been conducted in persons who were not on prophylaxis, but would be eligible for prophylaxis based on their bleeding history meeting the definition used in the randomized PRO.WILL study. 49 One was a retrospective analysis of European data that assessed the disease-related burden of VWD in persons on prophylaxis (n = 229) and those potentially eligible persons but not receiving prophylaxis (n = 102). Persons on prophylaxis were less likely to be hospitalized due to acute bleeds or have chronically damaged joints compared with persons not receiving prophylaxis (Figure 4). 115 Work productivity and HR-QoL were similar between the two groups, although only approximately 20%–25% of individuals completed these questionnaires. 115 The second analysis used data from the integrated US healthcare system for two different cohorts: the overall VWD population (n = 396); and a subset of these (n = 75) who were considered potentially eligible for prophylaxis treatment based on a history of severe and frequent bleeding. 116 Resource use was higher in the prophylaxis-eligible subset compared with the overall VWD population in terms of the percentage of persons with ⩾1 VWD-related outpatient (91% vs 81%) or emergency department (39% vs 13%) visit, and the mean number of inpatient stays (2.5 vs 1). 116

Bleeding-related complications in persons with VWD who were receiving prophylaxis compared with persons who were eligible for prophylaxis, based on bleeding history, but were not receiving prophylaxis. 124
Future directions
In contrast to HA, there are limited data available on prophylaxis in young children with VWD. The efficacy and safety of wilate prophylaxis in children (<6 years) with severe VWD is being investigated in the phase III WIL-33 study (NCT04953884). 30 A phase III study (NCT05582993) evaluating the efficacy and safety of Vonvendi in children up to 17 years of age is ongoing. 28
Determining the exact clinical indicators for prophylaxis in VWD is an important topic for investigation. Current international guidelines recommend the use of long-term prophylaxis in persons with VWD with a history of severe and frequent bleeding events. 23 However, a consensus on what constitutes “severe and frequent bleeds” would be beneficial to identify those who could benefit from prophylaxis.
Aside from playing an important role in VWD diagnosis and inhibitor risk assessment,52,117,118 genetic testing could also play a role in identifying persons with VWD who have a severe phenotype and may benefit from prophylaxis. The planned Genetics of VWD in the U.S. (VUS) study will investigate genotype-phenotype relationships in VWD and the potential role of comprehensive VWF genotyping in informing treatment decisions.
Individualized prophylaxis in VWD could help to optimize the dose and/or dosing frequency and provide even better protection against bleeding, in a similar way to what has been achieved with HA where individualized prophylaxis is now recommended as the standard of care.8,119–121 Factors that could be taken into consideration when individualizing VWD prophylaxis include age, VWD type, residual FVIII and VWF levels, bleeding phenotype (frequency, severity, and location (e.g., gastrointestinal bleeds vs nose/oral bleeds)), desmopressin response, and pharmacokinetics (PK). A population PK model has been developed by the OPTI-CLOT group that may facilitate more accurate targeting of VWF and FVIII levels during perioperative treatment with Humate-P. 122 Another group has developed a population PK model for type 3 VWD based on PK data in persons treated with rVWF or Humate-P. 123 However, the results of PK-guided dosing studies for prophylaxis in persons with VWD have not yet been published. Unlike prophylaxis studies in HA, where a target FVIII trough levels of ⩾1% is usually specified, there are limited data on the optimal VWF trough level target, or whether the same trough would be applicable in persons with different types of VWD, and how to account for the fact that many persons with VWD on prophylaxis may have measurable baseline levels. Studies to determine the appropriate trough levels in persons with VWD during prophylaxis could aid decision-making regarding dosing regimen. Such studies are more difficult in VWD than in HA due to the differences in VWF levels across VWD subtypes and the greater heterogeneity of bleeding sites in VWD than in HA. The predictive performance of population PK models in measuring VWF and FVIII levels and the association between these concentrations and bleeding events in persons with VWD is being evaluated in the OPTI-CLOT:To WiN study (EudraCT 2018-001631-46). 124 In addition, a population PK study is planned that aims to create and optimize a PK model for wilate.
Short-term prophylaxis with VWF replacement may be indicated to counter the increased risk of bleeding during menstruation, pregnancy, and postpartum in women with VWD.71,72 Current guidelines for HMB recommend consideration of hormonal therapy in women with VWD who do not wish to conceive and to consider tranexamic acid in those who wish to conceive. 23 There is evidence from clinical practice of the use and effectiveness of combination therapy with tranexamic acid and hormonal therapy for HMB.125,126 Efficacy and safety studies comparing combination therapy with single therapy are needed. 23 Persons not responding to these treatments or with contraindications should be treated with a VWF-containing product 127 which may also be used as an alternative to surgical control to mitigate HMB symptoms. 128 The EMPOWER trial (NCT06205095) will evaluate the effect of prophylaxis with wilate compared with placebo on HMB in women with VWD. The double-blind, randomized controlled trial will evaluate the effect of 2–3 doses of prophylaxis with 40–60 IU/kg wilate when provided on the two heaviest days within the first 4 days of menstruation compared with placebo (normal saline). In the childbirth setting, peripartum wilate was shown to be effective in preventing bleeds in a case series of 10 deliveries. 129 In addition, a report from a single-institution cohort study concluded that a strategy of targeting higher peak plasma VWF and FVIII:C levels (⩾100 IU/dL) at the time of delivery may be effective in reducing the risk of delivery-associated bleeding complications. 130 The Von Willebrand Factor in Pregnancy (VIP) study (NCT04146376) is an ongoing investigator-initiated, prospective, open-label, multicenter cohort study in the United States that is assessing the peripartum efficacy and safety of wilate in women with VWD. The primary objective is to observe the rate of primary postpartum hemorrhage in women who deliver with VWF levels >100%. Those with endogenous VWF levels <100% will be treated with wilate and tranexamic acid peripartum, and those with plasma levels ⩾100% will be treated with tranexamic acid. An ongoing, prospective, randomized trial (NCT04344860, VWD-WOMAN trial) is comparing the efficacy of rVWF (Vonvendi) plus tranexamic acid versus Vonvendi alone in reducing postpartum hemorrhage in women with VWD.
Further studies are needed to assess disease-related burden of severe VWD in well-defined populations, and to examine the effectiveness of prophylaxis in reducing this burden, as well as that of their family and caregivers. While the cost-effectiveness of prophylaxis versus on-demand treatment is well documented in persons with HA, 131 economic analyses comparing prophylaxis and on-demand treatment in persons with VWD are certainly needed and will be important to extend the currently limited reimbursement of VWF replacement for prophylaxis.
Several potential treatment strategies for VWD prophylaxis are at various stages of development that offer the prospect of reducing the frequency of intravenous infusion or enabling subcutaneous administration.132,133 These include therapies currently used for the treatment of HA (ultra-long half-life rFVIII (efanesoctocog alfa) and non-factor therapy (emicizumab)), an aptamer that increases VWF levels (BT200, rondoraptivon pegol), a bispecific antibody that binds and accumulates endogenous activated FVII (HMB-001), a monovalent antibody designed to increase levels of VWF and FVIII (HMB-002), and gene therapy.132–134
Conclusion
Despite the proven efficacy and safety of prophylaxis use in VWD, its adoption remains less established than FVIII prophylaxis in HA. The 2021 ASH/ISTH/NHF/WFH guidelines represented a step forward for persons with VWD by recommending the use of long-term prophylaxis for those who have a history of severe and frequent bleeds. Results from several studies of VWF prophylaxis have now been published since the guidelines were released,24–31 including phase III studies leading to the US FDA approval of Vonvendi for VWD prophylaxis in adults28,88 and for wilate in adults and children at least 6 years of age.30,89 Updated prophylaxis guidelines are needed and would provide valuable support for both treating physicians and persons with VWD.
Selecting those individuals who could benefit from prophylaxis is more complex than for HA. The FDA approval of prophylaxis for any type of VWD is a major step forward for persons with VWD in the United States because it allows treatment to be based on clinical needs regardless of VWD type. In persons treated on-demand, reasons to switch to prophylaxis might include frequent on-demand treatment in the past 6–12 months, bleeding events requiring hospitalization, failure of other therapeutic options (e.g., for HMB), bleeding interfering with daily activities, bleeding leading to iron deficiency and/or anemia, and bleed prevention for high levels of physical activity. For newly diagnosed individuals, reasons to start prophylaxis might include type 3 VWD, history of bleeds requiring hospitalization, recurrent bleeding episodes, and iron deficiency and/or anemia.
This narrative review was undertaken to identify potential barriers to the adequate implementation of prophylaxis in severe VWD and review the latest clinical evidence on prophylaxis in VWD. As a narrative review, it is acknowledged that there are some limitations. The identification of the barriers to prophylaxis was largely based on the personal experiences of the authors, together with a broad review of available published literature, and was not intended to constitute an exhaustive list. Given the nature of topic explored, a narrative review was selected to enable wider evaluation of the literature rather than the more structured but narrower approach of a systematic review.
After many years of lagging behind HA, barriers to prophylaxis use among individuals with VWD are finally being overcome. In the United States, persons with VWD now have access to effective prophylaxis options that have the potential to position this strategy as the new standard of care for persons with severe VWD and replicate the successful experience observed in HA. The use of personalized therapy in VWD deserves further investigation as it is likely this will also become a central component of VWD prophylaxis in the same way that it has for HA. A consensus on the most effective approach to identify individuals with VWD who would benefit from prophylaxis remains a key research priority.
Footnotes
Acknowledgements
Medical writing assistance was provided by Dominic Hague, PhD, at Cactus Life Sciences AG, Meggen, Switzerland. All the authors have authorized the submission of their manuscript via third party and approved any statements or declarations.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medical writing assistance was funded by Octapharma AG.
Competing interests
R.F.S. Jr has received research funding from Octapharma and Takeda, honoraria for consulting and advisory boards from Octapharma, Takeda, LFB, Sanofi, SOBI, Novo Nordisk, Bayer, Pfizer, BioMarin, Vega, and Guardian Therapeutics, and payment for expert testimony from Sanofi; has participated on a data safety monitoring board or advisory board for UniQure; and has had a role as American Thrombosis and Hemostasis Network board member, International Society on Thrombosis and Haemostasis (ISTH) Chair, Hemophilia Federation of America medical adviser, and with the Medical and Scientific Advisory Council of the National Hemophilia Foundation. F.F.C.-M. has a received a research grant from Bayer and educational grants from Octapharma; has received honoraria from Novo Nordisk and Biomarin, and acted as an advisory board member for Bayer, CSL Behring, Genentech, Octapharma, Sanofi, and Takeda. J.M.J. has received research funding from Octapharma to the University of Washington, and consulted for Biomarin, CSL Behring, and Takeda. M.S. reports unrestricted research funding from Octapharma and Pfizer, and honoraria for advisory boards and speaking engagements from Octapharma, SOBI, and Pfizer. C.M. has received research support from Roche, Bayer, Sanofi, Takeda, Pfizer, and Novo Nordisk; honoraria from Sanofi, Bayer, Octapharma, and Novo Nordisk; and participated in advisory boards for Bayer and Takeda. N.T.C. reports serving as a consultant for Takeda; participating in advisory boards for Takeda, Genentech, Sanofi Genzyme, Pfizer, Bayer, and Medzown; and receiving honoraria/travel support from Octapharma AG.
Availability of data and materials
Data sharing not applicable—no new data generated.