
Abstract
BACKGROUND:
Anastomotic leak (AL), as one of the most devastating complications, is the leading cause of mortality in colorectal cancer (CRC) patients after resection. This study was aimed to investigate potential risk factors for AL in elderly surgical CRC patients.
METHODS:
A total of 1068 elderly subjects who underwent elective curative colorectal surgery from 2012 to 2018 were retrospectively evaluated and enrolled into this study population. The predictive value of C-reactive protein-to-albumin ratio (CAR) for AL in surgical CRC patients was evaluated by receiver operating characteristic (ROC) curve analysis. Potential risk factors for AL were assessed by the univariate and multivariate logistic regression analyses.
RESULTS:
Of all the 1068 enrolled patients, 81 patients have developed AL with an incidence of 7.6% (81/1068). Preoperative CAR was an effective predictor for AL with an area under the curve (AUC) of 0.758, 95% CI of 0.700–0.817, a cut-off value of 2.44, a sensitivity of 61.09% and a specificity of 80.25%, respectively (
CONCLUSIONS:
Our study indicate that preoperative CAR level and duration of operation were two independent predictors for AL among elderly surgical CRC patients.
Introduction
Colorectal cancer (CRC) is globally the third most commonly diagnosed cancer and ranks as the fourth leading cause of cancer-related death worldwide [1]. Furthermore, the incidence of CRC continues to increase in developing countries including China due to the rapid population growth, aging and changed lifestyles [2]. Despite the improved proctocoloscopy and chemotherapy treatment, surgical resection remains the mainstay curative treatment of CRC [3]. Anastomotic leak (AL), as one of the most devastating complications, is the leading cause of mortality in CRC patients after resection [4]. AL is significantly associated with increased reoperation rates, delayed postoperative recovery, prolonged hospital stay, increased morbidity and mortality [5]. The reported incidence rate of AL in surgical CRC patients varies from 3% to 28% [6]. Moreover, delayed The reported incidence rate of AL in surgical CRC patients varies from 3% diagnosis of AL is closely associated with an increased postoperative mortality [7]. Therefore, to identify effective risk factors prior to operation is of critical importance for the prevention of AL.
An active systematic inflammatory response involves in the process of AL development. C-reactive protein (CRP) and albumin (Alb), are two circulating acute phase proteins in response to inflammation and they are closely associated with surgery-related inflammatory status [8]. Postoperative CRP trajectory have been indicated as a candidate predictor for AL in surgical patients with CRC [9, 10] and esophageal cancer [11]. Alb, a sensitive indicator in response to surgical stress, has also been suggested as a useful predictor of postoperative complications [12]. As reported by a multi-center study, serum Alb level is a potential risk factor for AL after colorectal resection in ovarian cancer surgery [13]. A novel indicator, CRP-to-Alb ratio (CAR), has been used to identify the risks of postoperative complications after colorectal surgery, with a superior diagnostic accuracy to CRP or Alb alone [14]. CAR is also reported to be a key indicator for AL after esophagectomy using the classification and regression tree analysis [15]. However, whether CAR can serve as a valid indicator for AL in elderly surgical CRC patients remains unclear, which is the aim of this present study.
Material and methods
Patients
This retrospective study was approved by the Medical Institutional Ethics Committee of Zhejiang provin-ce and HwaMei Hospital. Elderly CRC patients (
Data collection
The following data were extracted from the data-base. (1) Demographic data including age, gender, BMI, smoking and alcohol habits, history of abdominal surgery, preoperative comorbidities (diabetes mellitus, hypertension, hyperlipemia and chronic obstructive pulmonary disease (COPD)) and American Society of Anesthesiologists (ASA) grade; (2) The surgery-related data including surgical approach, duration of operation, estimated blood loss, number of lymph nodes resection, perioperative blood transfusion and time to first flatus; (3) The tumor-related data including preoperative tumor complication (anemia, ileus, etc.), tumor location, tumor and node stage; (4) Laboratory tests.
Laboratory tests
Preoperative peripheral venous blood samples were obtained on 1 day before the surgery. The blood cell analyses including white blood cell (WBC), hemoglo-bin (Hb), platelet (Plt) and hematocrit (Hct), biochemical examinations including Alb, creatinine and urea were detected in the laboratory of our hospital. The inflammatory cytokines including CRP, interleukin-6 (IL-6) and tumor necrosis factor-
AL definition
AL, as the primary endpoint in this study, was defined as the leakage of bowel content from the anastomosis according to the descriptions by previous reports [16]. In brief, clinical AL was diagnosed if any one of the following descriptions were present: fecal or gas discharge from the surgical incision, drain tract or vagina; fecal peritonitis; intraabdominal peritonitis or abscess along with an anastomotic defect which was verified through imageological examination, colonoscopy, or laparotomy. Moreover, those patients with a pelvic abscess near the anastomotic site with no obvious signs of fecal fistula were also categorized into AL group [17].
Statistical analysis
Statistical analyses were performed using GraphPad prism (version. 5.0, GraphPad Inc., San Diego, CA, USA) and SPSS (version 19.0, SPSS Inc., Chicago, IL, USA). Comparisons of AL and Non-AL groups were performed using Chi-square test with respect to categorical variables, Student
Results
Patient characteristics
According to the inclusion and exclusion criteria, a total of 1068 elderly subjects who underwent elective curative colorectal surgery were enrolled in the final analysis. Of these, 81 patients have developed AL with an incidence of 7.6% (81/1068). The mean age for all the enrolled patients was 72.0 years and the majority were male patients (58.3%, 623/1068). Table 1 lists the demographic, the surgery- and tumor-related data between the patients who had AL or not. There were no significant differences in gender distribution, smoking and alcohol habits, ASA grade, sex, ASA, and operation between patients with or without AL development (
Laboratory tests and AL
As shown in Table 2, patients with AL had a significantly lower Hb (
Preoperative CAR and AL
We constructed the ROC curve to access the predictive value of preoperative CAR for AL in surgical CRC patients. As presented in Fig. 1, preoperative CAR was an effective predictor for AL with an area under the curve (AUC) of 0.758, 95% CI of 0.700–0.817, a cut-off value of 2.44, a sensitivity of 61.09% and a specificity of 80.25%, respectively (
Predictive value of preoperative CAR for AL in elderly surgical CRC patients by ROC curve analysis. Preoperative CAR was an effective predictor for AL in CRC patients with an AUC of 0.758, 95% CI of 0.700–0.817, a cut-off value of 2.44, a sensitivity of 61.09% and a specificity of 80.25%, respectively (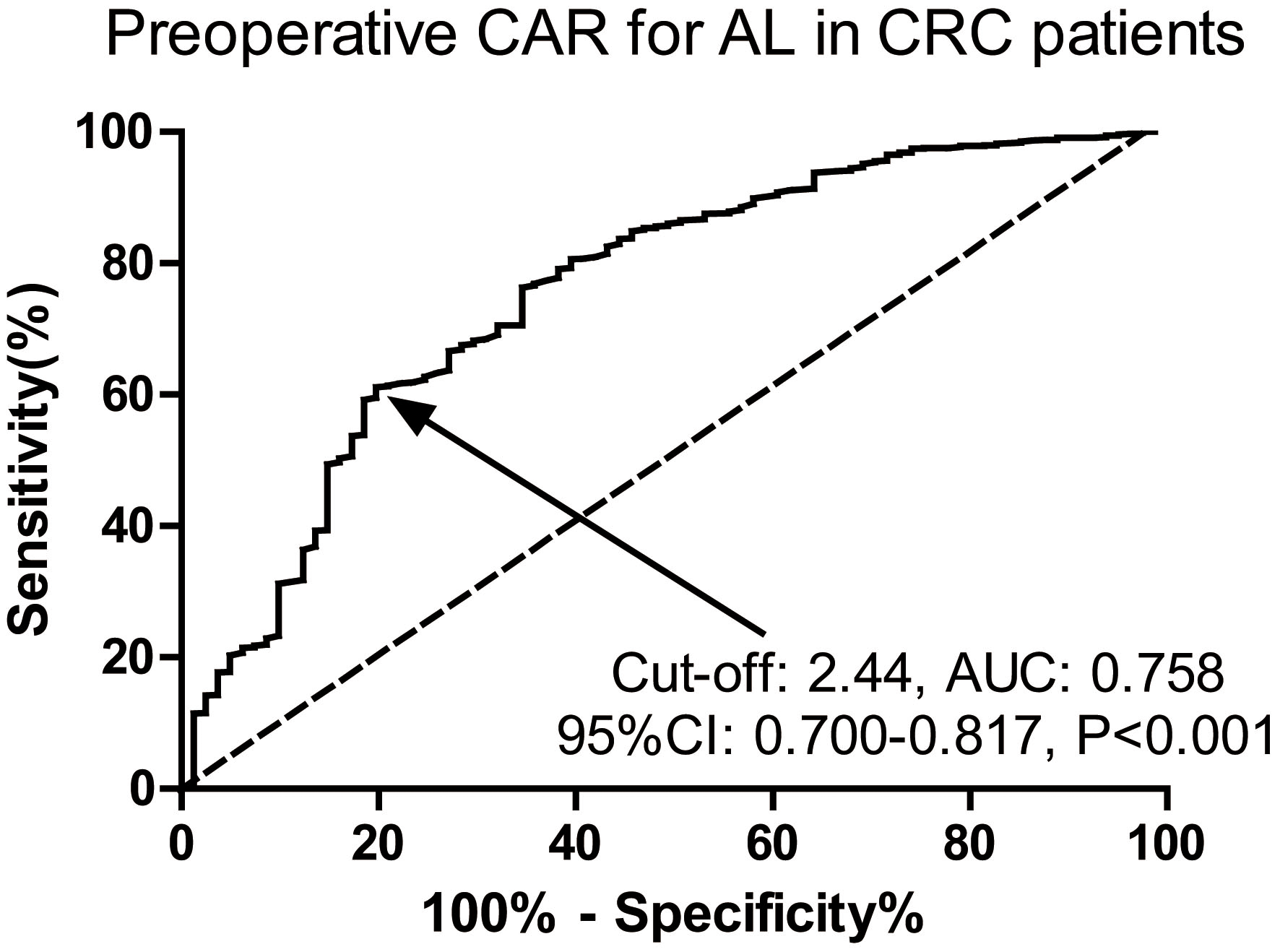
Clinicpathological parameters associated with AL in CRC patients
AL, anastomotic leak; CRC, colorectal cancer; BMI, body mass index; ASA, American Society of Anesthesiologists.
Laboratory tests associated with AL in CRC patients
AL, anastomotic leak; CRC, colorectal cancer; Hb, hemoglobin; Plt, platelet; WBC, white blood cell; Hct, hematocrit; IL-6, interleukin-6; TNF-
Risk factors for AL in CRC patients by univariate and multiple logistic regression analysis
AL, anastomotic leak; CRC, colorectal cancer; Hb, hemoglobin; IL-6, interleukin-6; TNF-
Table 3 presents potential risk factors for AL among the elderly surgical CRC subjects. The following five risk factors were found to be potentially associated with AL in the univariate logistic regression model: age, history of abdominal surgery, diabetes mellitus, duration of operation and preoperative CAR (
Discussion
The results of this present study indicate that duration of operation and preoperative CAR were two independent risk factors for AL among elderly surgical CRC patients. The incidence of AL in this study was calculated to be 7.6%, which was quite similar to the reported rate of 8.4% by habits [20] have been shown to be associated with Frasson et al. [18]. Male sex [19] and smoking increased risk of AL development by some studies. Our results also showed that the current smoking habits were associated with AL development. However, our results of logistic regression analysis did not suggest the predictive roles of male sex and smoking habits for AL. Some other factors described in previous studies, such as BMI [21] and surgical approach [16], were not found to be closely related with AL development in this present analysis.
Our results by the univariate logistic regression model indicate five potential risk factors including age, history of abdominal surgery, diabetes mellitus, duration of operation and preoperative CAR. Nevertheless, the final multivariate analysis only support duration of operation and preoperative CAR as the two independent predictors for AL. Diabetes mellitus has been reported to be associated with an increased risk of AL in elderly patients after colectomy [22]. Another study by Yao and Zhang has also indicated diabetes mellitus as a risk factor of AL in the procedures of trans-abdominal and transanal total mesorectal excision for rectal cancer [23]. A systematic review by Li et al. has demonstrated that diabetes mellitus is a significant risk factor of AL for patients after esophagectomy [24]. The history of previous abdominal surgery is reported gastrointestinal anastomosis [25]. On the contrary, to be an independent risk factor for AL development after lower some other studies show that no significant association is observed between abdominal surgery history and early or Late AL in patients undergoing surgery for CRC [26], which is in accordance with our results. As revealed by previous literature, older age is associated with the postoperative complications, overall survival, cancer-and cardiovascular-specific mortality [27]. Age is also associated with increased risk of early AL (within day 6 postoperatively) after surgical resection for CRC [26]. However, this present study did not suggest its predictive role of age for AL. We consider that the different patients characteristics, sample sizes, surgical types and the disease heterogeneity might be possible explanations for the different conclusions.
A population-based study has shown that greater operative duration can serve as a valid predictor for AL after colorectal resection [28], which strongly supports our conclusions. An operation time over 3 hours has been identified as a significant risk factor for both minor and major AL through a national analysis [29]. As an indicator of surgical difficulty, our results corroborate previous findings that operation time is an independent predictor for AL. Longer operation time was usually associated with increased surgical difficulty, which might lead to technical failure of the anastomosis and increased risk of AL. To our knowledge, previous published data regarding CAR and AL are quite limited. The study by Shao et al. has reported the predictive role of CAR for AL [15]. Different from our study design, they performed the study in patients following esophagectomy and the application of classification and regression tree analysis indicated the predictive role of postoperative CAR level for AL. Postoperative CRP levels, especially on postoperative day 3 or 4, were widely suggested to be utilized for postoperative AL prediction [30, 31] and diagnosis [9, 32]. Furthermore, postoperative serum Alb concentration instead of preoperative Alb was indicated as an independent risk factor for AL in CRC patients [33]. While CAR, taking CRP and Alb into combination, was proved to be a potential predictor for AL in this study. Our analysis identified a CAR cutoff value of 2.44 as having the predictive value for AL. When comparing with CRP or Alb alone, CAR is a better index for the reflection of inflammation stress [14]. Furthermore, CAR is also a valid index for nutritional status assessment, which is associated with the anastomotic healing. Beyond the tension and ischemia, some biological factors that may impact anastomotic healing significantly remain poorly understood [34]. New insights focusing on the pathophysiology of AL at the molecular and cellular level will lead to solutions for AL [34]. The potential mechanisms for the predictive role of CAR for AL remains unclear due to the unclear physiopathologic mechanisms of AL. In our consideration, the association between inflammation, nutritional status and anastomotic healing might be the possible explanations for the predictive role of CAR for AL in surgical CRC patients. It is well known that angiogenesis, collagen deposition and inflammation play critical roles in the process of anastomotic healing [35]. In comparison with CRP, CAR is a better marker reflecting the inflammatory status. Furthermore, CAR is reported be closely linked to imperfect reperfusion and the prognosis of myocardial infarction in patients undergoing percutaneous coronary intervention treatment, indicating the potential association between CAR and ischemia [36]. The reports mentioned above might offer potential explanations for the predictive value of CAR for AL. As a sensitive and effective marker for systemic inflammatory response, CAR has been suggested to be a valid novel indicator for clinical outcomes [15]. Postoperative CAR was reported to be a novel predictor for short-term complications in patients with gastric cancer following gastrectomy [37]. Ge et al. have revealed that CAR could help to identify the risks of postoperative complications after colorectal surgery, with a higher diagnostic accuracy than CRP alone [14]. Moreover, a previous study by Kim et al. has indicated CAR at admission as a significant predictor for mortality in patients with severe sepsis or septic shock [38]. Another study by Gibson et al. has also reported that CAR is an effective predictor for clinical efficacy in patients with acute severe ulcerative colitis [39].
Steele et al. have stated that anastomosis ischemia is probably the leading cause of AL, based on the theory that adequate blood flow occupies the major contributing factor to the integrity and viability of the anastomotic stoma [40]. Ischemia-modified albumin (IMA), a test using copper binding assay, some level of efficiency [41]. A previous study by has been recently suggested to be a potential marker of bowel ischemia with Hyspler et al. has found that IMA was an efficient predictor of AL in colorectal surgery patients [42]. Intestinal Fatty Acid Binding Protein (i-FABP), a protein which is expressed in the cytosol of enterocytes, is significantly associated with epithelial destruction, resulting in intestinal ischemia [43]. An experimental study in rats has indicated i-FABP as a potential marker of AL after colonic resection [44].
Conclusions
In conclusion, our study indicate that preoperative CAR level and duration of operation were two independent predictors for AL among elderly surgical CRC patients. In our opinion, our conclusions may have important implications during preoperative patient counselling, evaluation, and decision-making for defunctioning stoma formation. This study has some limitations. First, this is a single-center study with the retrospective nature. Second, only preoperative CRP and Alb values are evaluated and whether postoperative levels can serve as a predictor for AL remains unclear. The last, the involved mechanisms for the predictive role of CAR is not investigated and more longitudinal studies with larger scales are urgently required to confirm our findings.