To date, serological markers to monitor melanoma progression and response to therapy are lacking. In this context cytokines appear to be promising biomarkers of the disease.
OBJECTIVE:
To compare cytokine and chemokine levels in melanoma patients and in healthy controls and to assess possible variations according to melanoma stage.
METHODS:
Serum chemokine and cytokine levels were determined by ELISA in 34 patients diagnosed histologically of malignant melanoma. Seven healthy volunteers were used as controls.
RESULTS:
We found a subset of cytokines (CCL3, CCL4, IFN- and IL-10) to be significantly higher in melanoma patients than in control group, thus confirming the importance of the inflammation in cancer. While CCL3 increased with tumor progression, IFN- and IL-10 showed higher levels in stage I patients. Moreover, we noticed a direct correlation between CCL3 level and the presence of ulceration in the primary tumor; on the contrary, CCL4, IL-10 and IFN- were lowered down in patients with ulcerated melanoma.
CONCLUSIONS:
These results expand and confirm observations made in other studies focusing on a more limited number of molecules. This extended panel of cytokines examines the potential roles of type2 cytokines (such as IL-4) and many chemokines (mainly CCL3) as biomarkers in melanoma progression.
Melanoma is one of the most aggressive forms of human cancer and its incidence has significantly increased worldwide over the last decades [1, 2, 3]. Every year, more than 100,000 melanomas occur worldwide. The lifetime risk of developing a melanoma is higher for whites than for other ethnic groups: nearly 2.4% for caucasians, 0.1% for blacks, and 0.5% for Hispanics [4, 5]. Intermittent UV exposure, especially during childhood, personal or family history of melanoma, presence of numerous melanocytic nevi and skin phototype I and II are important risks factors [6, 7, 8]. While surgery is the mainstay of therapy for localized disease, generalized forms of the disease have a poorer prognosis and were once considered incurable [9, 10, 11]. Melanoma staging has recently been revised by the American Joint Committee on Cancer [12, 13]. The most reliable outcome predictors, apart from the stage, are in fact several clinical and histological features of the primary tumor, which include not only the Breslow thickness and the presence of ulceration, but also the mitotic rate and the peri-tumoral inflammatory infiltrate [14, 15, 16]. Many authors characterized the peritumoral inflammatory infiltrate with a particular attention to tumor-infiltrating lymphocytes (TILs) [17, 18, 19, 20, 21]. Host-immune response evasion plays a key role in tumor growth and metastatization, as also confirmed by many studies both in animal models and in humans, with all the tested vaccines promoting an antigen-specific anti-tumor T-cell response [22, 23, 24, 25, 26, 27]. Patients with metastatic disease experience profound systemic immunosuppression due to tumor burden, documented to be IL-2 dependent [28, 29, 30]. Global cytokine suppression in the host, together with a selective increase in specific chemokines, constitute a predominant feature of certain melanoma metastatic localizations, such as uveal, lung or brain [31, 32, 33, 34, 35].
Nowadays new therapies boosting the anti-tumor immune response are available both as adjuvant therapies for stage III and as systemic treatments for stage IV disease [36, 37, 38]. These therapies demonstrated higher efficacy than traditional chemotherapy and are today considered first-choice treatments. Efficacy of those treatments (PD1- and CTLA4-inhibitors in particular) gives reason to the central role of the immune system in tumor growth and metastasis, meaning that serological tumor markers should be revisited [39, 40, 41]. Serological markers have not widely been introduced yet in routine clinical practice due to their insufficient diagnostic sensitivity and specificity [42, 43, 44]. Many studies identified possible cytokines subset to use as biomarkers, but they still are not routinely used [45, 46, 47]. In melanoma patients, cytokine profiles seem to be directly related to clinical course and a cytokine imbalance could be associated to tumor progression [48, 49]. However, no validated immune markers are today available so far for prognostic setting and monitoring of patients affected by melanoma [50, 51, 52]. We took advantage of serum-saving pre-arranged multiplexed arrays in order to explore the immunological landscape of cytokines with inflammatory and/or regulatory activities, with particular attention to chemokines, in melanoma patients at different stages.
Methods
We enrolled 34 patients affected by melanoma, referred to the “SS. Annunziata” dermatology clinic (Chieti, Italy) between 2001 and 2017, and 7 healthy controls (HC) in our study (for patient and control characteristics, see Table 1).
Stage, sex and age distribution of the subjects enrolled in the study
Stage
Patients
Age: mean SD (range)
()
TOT
F
M
F
M
I
10
5
5
39.8 11.25 (29–52)
43 13.5 (31–64)
II
12
9
3
48.7 13.3 (27–63)
60 12.1 (47–71)
III
6
2
4
49.5 9.1 (43–56)
54 19 (33–73)
IV
6
3
3
50.6 22.5 (29–74)
65 6.8 (60–73)
0 (HC)
7
4
3
51.5 7.5 (43–60)
44 15 (30–60)
HC: healthy controls; SD: standard deviation.
HC included 4 women and 3 men (M:F ratio 1:1.3), with a mean age of 48. Patients were stratified according to the 8th AJCC classification (American Joint Committee on Cancer Classification of cutaneous melanoma 2018) and included all the possible disease stages (stage I, II, III and IV). The study and consent procedure were approved by the involved Hospital’s Ethics Committee. We obtained appropriate institutional review board approval and have followed the principles outlined in the Declaration of Helsinki for all human experimental investigations. Patients and healthy subjects have provided their written informed consent. For each subject, both serum cytokines and the tumor inflammatory infiltrate were examined. We measured serum levels of a total of 12 cytokines (8 of them belonging to the chemokine family) in 34 patients diagnosed histologically with malignant melanoma just after excision and staging, before the beginning of any systemic therapy, and in 7 HC. Measurements included interleukin (IL)-2, interferon (IFN)-, IL-4 and IL-10, Chemokine C-C Motif Ligand 3, CCL3 (or Macrophage Inflammatory Protein (MIP)-1), CCL4 (MIP-1), CCL2 (or Monocyte Chemotactic protein (MCP)-1), CCL17 (or Thymus and Activation Regulated Chemokine, TARC), CCL1 (or I-309), CCL11 (or eotaxin), CCL22 (or Macrophage Derived chemo-attractant, MDC) and Chemokine (C-X-C motif) Ligand 8, CXCL8 (or IL-8).
Patient characteristics: age, sex, features of the primary tumor (Breslow thickness, ulceration, regression, inflammatory infiltrate), staging (TNM and AJCC)
Patient
Age
Sex
Breslow
Ulceration
Regression
Inflammatory
TNM
Stage
thickness
infiltrate
1
47
M
1.75 mm
Present
Absent
Present: brisk type
T2bN0M0
IIA
2
52
F
1.8 mm
Present
Absent
Present: brisk type
T2bN0M0
IIA
3
62
M
2.5 mm
Absent
Present
Absent
T3aN0M0
IIA
4
31
F
1.3 mm
Present
Absent
Absent
T2bN0M0
IIA
5
61
F
2.5 mm
Absent
Absent
Present: brisk type
T3aN0M0
IIA
6
63
F
1.8 mm
Present
Absent
Absent
T2bN0M0
IIA
7
56
F
3.5 mm
Present
Absent
Absent
T3bN2bM0
IIIB
8
63
F
2 mm
Present
Absent
Present: brisk type
T2bN0M0
IIA
9
33
M
3.8 mm
Absent
Absent
Absent
T3aN2bM0
IIIB
10
44
F
1.1 mm
Present
Present
Present: brisk type
T2bN0M0
IIA
11
43
F
3.4 mm
Present
Absent
Present: brisk type
T3bN2aM0
IIIC
12
73
M
3 mm
Present
Present
Absent
T3bN1aM0
IIIA
13
71
M
1.9 mm
Present
Absent
Present: band like type
T2bN0MO
IIA
14
54
F
1.5 mm
Present
Absent
Present: brisk type
T2bN0M0
IIA
15
33
F
0.8 mm
Absent
Absent
Absent
T1bN0M0
IB
16
64
M
1.1 mm
Absent
Absent
Absent
T2aN0M0
IB
17
43
M
4.8 mm
Present
Absent
Absent
T4bN2bM0
IIIC
18
52
F
0.36 mm
Absent
Absent
Absent
T1aN0M0
IA
19
34
M
0.31 mm
Absent
Absent
Present band like type
T1aN0M0
IA
20
60
M
8 mm
Present
Present
Present: brisk type
T4bN0M1b
IV
21
74
F
2 mm
Absent
Absent
Absent
T2aN2aM1c
IV
22
27
F
1.75
Present
Absent
Absent
T2bN0M0
IIA
23
31
M
0.60 mm
Absent
Present
Absent
T1aN0M0
IA
24
73
M
1.7 mm
Present
Absent
Present: brisk type
T2bN0M1c
IV
25
33
F
1.6 mm
Absent
Absent
Present: brisk type
T2aN0M0
IB
26
63
M
6 mm
Absent
Absent
Absent
T4aN2bM1b
IV
27
67
M
2 mm
Absent
Absent
Present: brisk type
T2aN1bM0
IIIB
28
49
F
5 mm
Absent
Absent
Present: band like type
T4aN0M1c
IV
29
36
M
0.30 mm
Absent
Present
Absent
T1aN0M0
IA
30
50
M
0.68 mm
Absent
Absent
Absent
T1aN0M0
IA
31
52
F
0.50 mm
Absent
Absent
Present: brisk type
T1aN0M0
IA
32
44
F
2.2 mm
Absent
Absent
Present: brisk type
T3aN0M0
IIA
33
29
F
1.6 mm
Absent
Absent
Absent
T2aN2bM1c
IV
34
29
F
0.6 mm
Absent
Present
Present: band like type
T1aN0M0
IA
Cytokines serum levels expressed in pg/ml in patients at different stages of melanoma as median and IQR
Stage
I ( 10)
II ( 12)
III ( 6)
IV ( 6)
-value
CCL3
173.4
(159.0–246.6) pg/ml
297.5
(253.3–368.0) pg/ml
330.0
(272.0–438.0) pg/ml
222.0
(175.6–256.3) pg/ml
0.001
CCL4
130.7
(85.0–168.3) pg/ml
89.5
(70–110.4) pg/ml
143.0
(61.3–210.2) pg/ml
199.4
(171.3–297.5) pg/ml
0.011
CCL2
344.1
(208.9–875.5) pg/ml
447.5
(317.1–632.3) pg/ml
544.0
(363.7–728.3) pg/ml
595.6
(455.0–1322.2) pg/ml
0.378
CCL1
350.2
(293.7–618.9) pg/ml
284.0
(146.3–377.0) pg/ml
267.0
(165.0–526.5) pg/ml
466.2
(356.7–631.3) pg/ml
0.084
CCL17
95.25
(63.0–252.3) pg/ml
88.0
(56.5–293.8) pg/ml
207.4
(68.5–634.7) pg/ml
211.4
(101.8–338.3) pg/ml
0.740
CCL11
296.8
(242.0–659.8) pg/ml
313.5
(253.3–453.8) pg/ml
267
(204.5–443.5) pg/ml
359.8
(278.2–514.7) pg/ml
0.698
CCL22
461.9
(313.9–927.2) pg/ml
753.2
(547.5–925.8) pg/ml
729
(575.5–887.4) pg/ml
739.9
(569.5–895.6) pg/ml
0.347
IL-8
10.6
(6.8–28.2) pg/ml
10.0
(7.0–12.1) pg/ml
13.5
(5.5–24.9) pg/ml
29.8
(9.9–99.2) pg/ml
0.162
IL-2
51.5
(28.1–89.5) pg/ml
37.6
(23.0–58.7) pg/ml
61.5
(26.4–72.9) pg/ml
38.7
(24.8–64.2) pg/ml
0.339
IFN
59.5
(42.5–127.5) pg/ml
8.0
(4.0–11.1) pg/ml
11.5
(3.9–46.9) pg/ml
28.5
(3.8–71.0) pg/ml
0.003
IL-4
28.15
(2.4–61.4) pg/ml
6.0
(5.0–8.0) pg/ml
10.0
(3.1–17.1) pg/ml
1.3
(0.0–14.6) pg/ml
0.098
IL-10
29.4
(5.6–73.7)
3.0
(2.3–7.0)
6.0
(1.5–22.1)
2.8
(1.1–6.6)
0.004
a: Kruskall-Wallis test. MIP-1, MIP-1, IFN- , and IL-10 are significantly higher in melanoma patients compared to HC. A statistically significant increase in MIP-1, and a concomitant decrease in IFN-, and IL-10 levels is evident between stage I and II; MIP-1 is particularly elevated in stage IV patients. IL-4 tends to decrease with disease progression, while IL-8 increases. IL-2 is typically very low in the stage IV group. However, data regarding IL-2, IL-4 and IL-8 are not statistically significant.
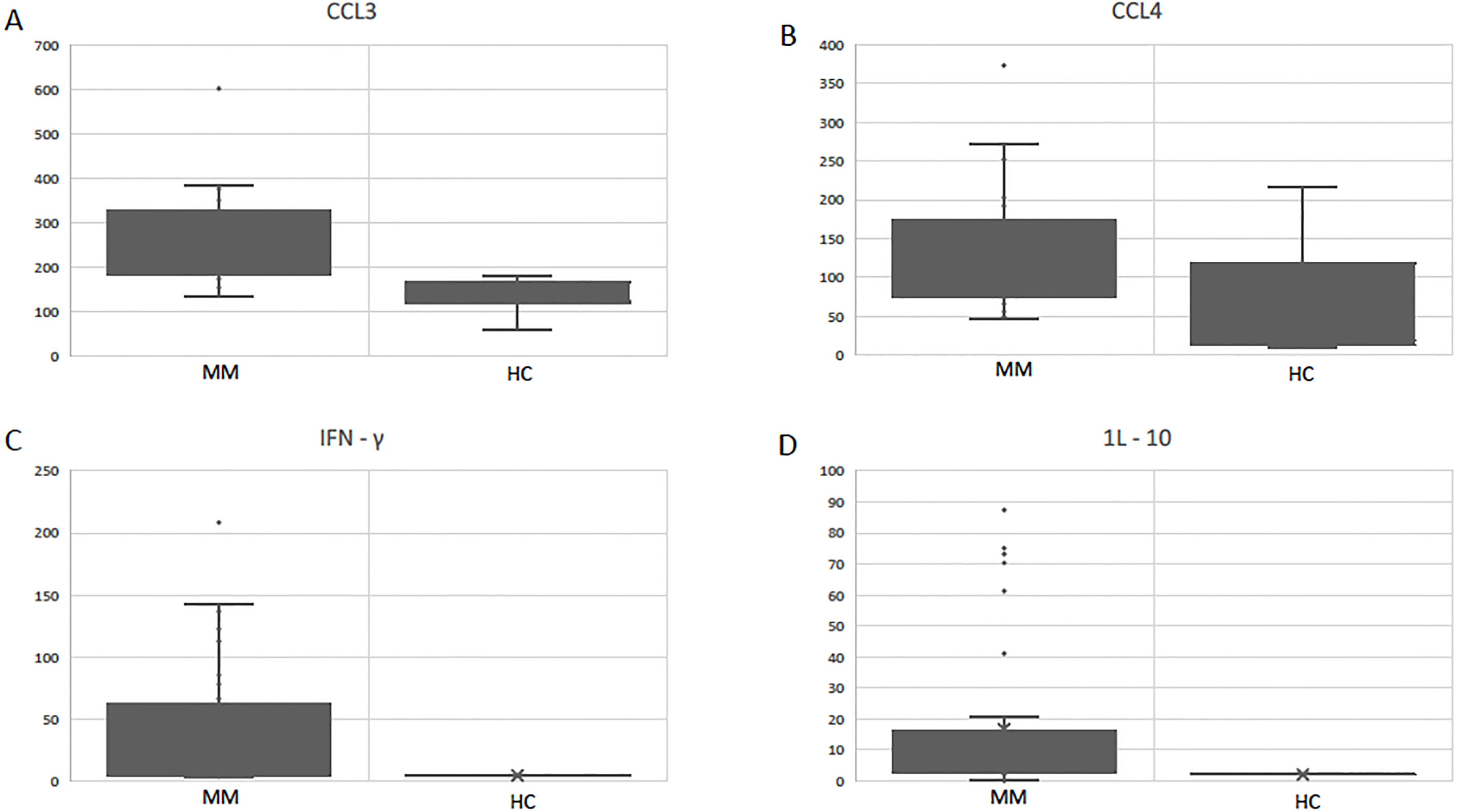
CCL3, CCL4, IFN-, and IL-10 serum levels (expressed in pg/ml) in melanoma patients (MM) compared to HC. All those cytokines showed significantly higher levels in MM when compared to HC. Kruskall-Wallis test was used to determine differences among different groups.
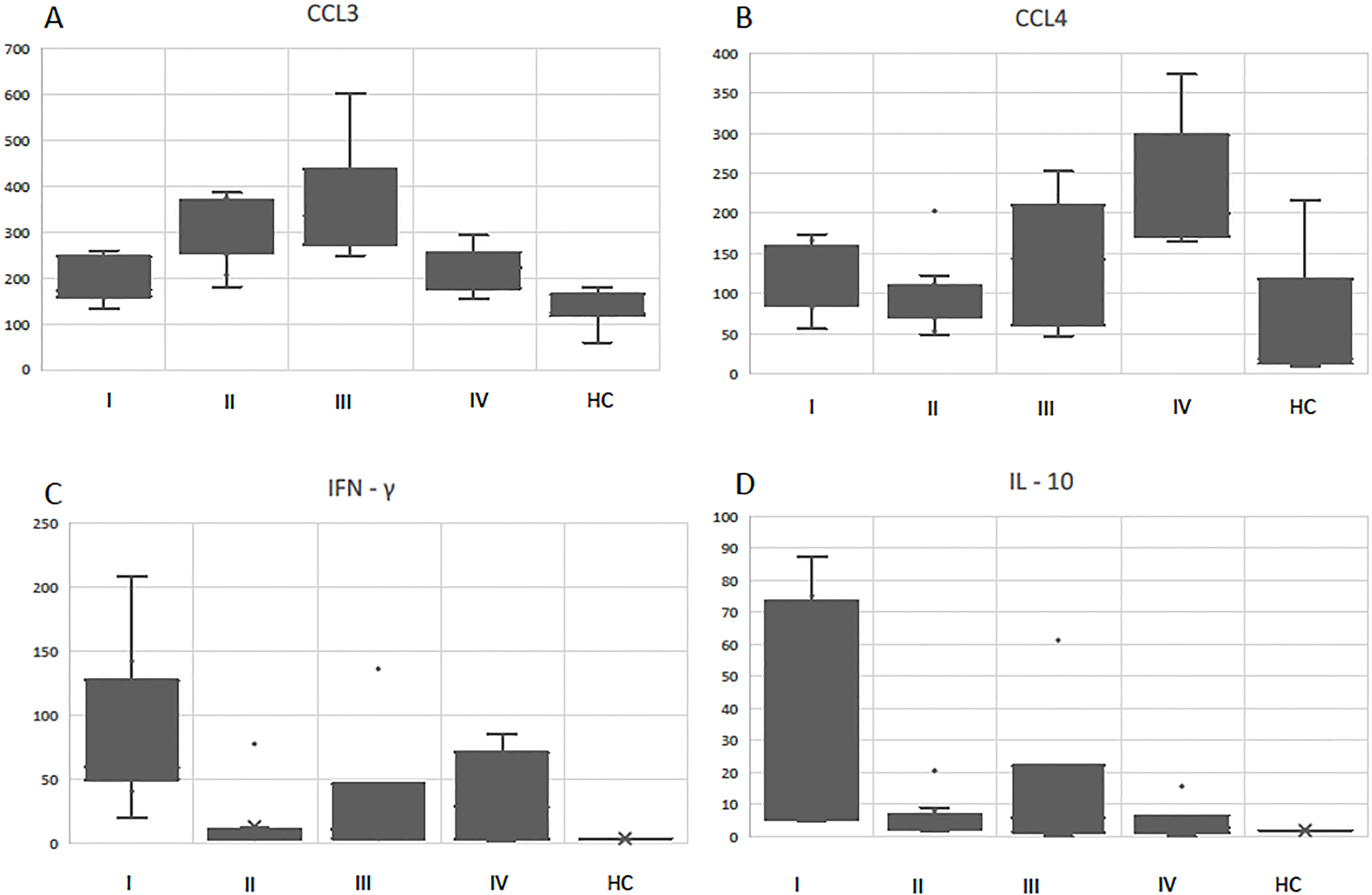
Correlations between CCL3, CCL4, IFN-, IL-10 levels (expressed in pg/ml) and melanoma stages. Panel a: CCL3 increases from stage I to stages II–III. Panel b: CCL4 is higher in stage IV patients when compared to stage I–III. Panel c: IFN- is significantly higher in stage I patients rather than stages II–IV. Panel d: also IL-10 levels are higher in stage I and decrease in more advanced stages. Kruskall-Wallis test was used to determine differences among different groups.
Serum cytokine and chemokine levels were determined by enhanced ELISA-type assays, namely multiplex and protein microarray methods (Pierce Searchlight Proteome Arrays, Search Light Human Th1/Th2 Array 1 and 2, Boston, MA; Human Chemokine array 1, Pierce-Endogen, Rockford, IL, USA). Samples were processed according to the manufacturer’s instructions. Chemiluminescence was detected with an Image and Analysis System, equipped with Array Vision software and a cooled CCD camera (Perbio Science GmbH, Bonn, Germany).
We correlated the serum levels with known parameters affecting clinical outcome, such as Breslow thickness, ulceration status, and lymphocytic infiltrate, as well as stage of disease.
Statistical analysis was performed by Kruskall-Wallis test, Mann-Withney U test and Spearman’s rank test. In particular, correlation between cytokines serum levels and melanoma stage was measured with Kruskall-Wallis test, while Mann-Withney U test was performed to asses correlation of cytokine levels with ulceration; Spearman’s rank test was used to analyze possible correlations among cytokine serum levels. Significance was defined as 0.05 when comparing various groups or parameters.
Serum levels of CCL4, CCL3, IFN- and IL-10 expressed in pg/ml
CCL4
CCL3
IFN-
IL-10
Stage I
111
.5
173
.2
122
.5
75
.1
81
.2
251
.8
142
.6
87
.4
101
.8
160
.3
60
.6
17
.7
149
.9
202
.8
112
.6
70
.3
154
.3
259
.8
43
5
.7
166
.3
155
.1
53
.9
11
.3
174
.1
173
.6
40
.9
5
155
.2
244
.8
208
.6
41
.1
86
.3
162
20
.1
5
.3
56
.2
132
.5
58
.4
73
.2
Stage II
74
303
5
3
49
376
12
8
75
376
4
2
203
344
11
4
73
341
10
3
104
386
4
2
69
284
4
4
53
292
4
3
105
.3
206
.3
11
.1
2
105
260
7
3
112
.1
181
.1
77
.9
20
.5
123
251
9
9
Stage III
147
603
10
5
47
383
4
2
66
317
17
7
252
.3
248
.8
3
.5
0
139
343
13
9
196
.2
279
.8
136
.4
61
.2
Stage IV
272
.2
293
.2
85
.3
3
.5
165
244
20
.6
2
192
.4
220
.7
36
.4
1
.5
173
.4
223
.2
3
0
373
.2
186
.1
4
.1
3
.5
206
.3
143
.9
66
.2
15
.7
Subtot overall M
165
.06
264
.76
41
.81
16
.6
HC
216
165
4
2
18
123
4
2
13
59
4
2
86
161
4
2
19
119
4
2
10
121
4
2
118
180
4
2
Subtot HC
125
.71
132
.57
4
2
M: melanoma patients; HC: healthy controls.
Results
Patients had a mean age of 49.9 14.7 and a male:female ratio of 1:1.2. Mean Breslow thickness was 2.2 mm. Ulceration was present in 15 cases, none of them classified as stage I. Regression was present in 7 primary tumors and half of the cases showed peritumoral inflammatory infiltrate, 4 being band-like type and 13 brisk-type. Patient characteristics are summarized in Table 2.
Cytokine and chemokine levels both in patients affected by melanoma and in healthy controls were measured. Results were then divided according to disease stage. As shown in Table 3, only results regarding CCL3, CCL4, IFN- and IL-10 were considered significant and mainly correlated with disease stage. However, a significant principal difference ( 0.05) between all melanoma patients and healthy controls (HC) was found: all the four above-mentioned cytokines showed lower levels in the control group, thus confirming the prominent role of inflammation in cancer [53, 54, 55] (see Fig. 1 and Table 4).
All the significant correlations between these four cytokines and melanoma stages are shown in Fig. 2. A statistically significant increase in CCL3, and a concomitant decrease in IFN-, and IL-10 levels has been noticed between stage I and II (see Fig. 2, panels a, c, d). Moreover, IFN- and IL-10 levels continue to be significantly lower in stage III and IV, while CCL3 is persistently increased.
Patients with stage-I disease show IL-10 and IFN- serum levels significantly higher when compared to healthy controls, while IFN- and IL-10 decrease together with disease progression. CCL4 was particularly elevated in stage IV patients, both when compared to healthy controls and stage I-III (see Fig. 2, panel b).
As shown in Table 3, IL-4 tends to decrease with disease progression, while IL-8 (a chemokine well known to be correlated to a metastatic phenotype) increases [56, 57]. IL-2 is typically very low in the stage IV group. However, data regarding IL-2, IL-4 and IL-8 are not statistically significant.
Cytokines serum levels in pg/ml in patients with and without ulceration as median and IQR (interquartile range)
Ulceration
Absent ( 19)
Present ( 15)
-value
CCL3
202.8
(162.0–251.8)
317.0
(284.0–376.0)
0.001
CCL4
149.9
(105.0–192.4)
75.0
(66.0–165.0)
0.043
CCL2
471.0
(313.1–573.6)
618.0
(329.0–852.1)
0.242
CCL1
380.3
(294.3–470.2)
251.0
(147.0–504.2)
0.066
CCL17
116.9
(71.6–246.3)
236.0
(58.0–294.0)
0.560
CCL11
304.9
(251.6–540.1)
278.0
(238.0–463.4)
0.372
CCL22
612.7
(412.6–829.6)
780.0
(616.0–971.0)
0.147
IL-8
11.0
(7.0–25.8)
11.0
(7.0–20.0)
0.632
IL-2
53.1
(27.6–84.0)
33.2
(23.0–64.0)
0.157
IFN-
53.9
(13.0–112.6)
10.0
(4.0–12.0)
0.001
IL-4
14.5
(2.0–35.3)
6.0
(4.0–9.0)
0.128
IL-10
11.3
(5.0–61.2)
3.0
(2.0–4.0)
0.001
a: Mann-Withney U test. MIP-1 is significantly higher in patients with ulcerated melanomas, while MIP-1, IL-10 and IFN- are lowered down in this subgroup of patients.
Tumor thickness is certainly a major determinant in melanoma staging, especially for stage I and II, but ulceration plays also a key role in melanoma staging. Cytokine and chemokine levels were stratified according to the presence or absence of ulceration (see Table 2). None of the 8 patients with T1 (Breslow 1 mm) had histologically proven ulceration, while in T2 group (Breslow thickness between 1.1 and 2 mm), 9 patients out of 14 had ulcerated melanomas. Tumor thickness and ulceration are in fact two highly-associated variables: none of the patients with a melanoma 1 mm had ulceration, while the majority of tumors 1 mm was ulcerated. It is therefore quite impossible to evaluate the statistical significance of the two isolated variables. However, as shown in Table 5, CCL3 is significantly higher in patients with ulcerated melanomas, while CCL4, IL-10 and IFN- are lowered down in this subgroup of patients.
a: Spearman’s rank test. An inverse correlation between MIP-1 and IL-10 and/or IFN- is present: IL-10 and IFN- higher in stage I and slowly decrease in parallel to MIP-1 increase.
Trends of different cytokines in patients affected by melanoma are strictly correlated one to each other. Table 6 summarizes all the statistically significant correlations among cytokines. It’s important to underline that our results confirm the inverse correlation between CCL3 and IL-10 and/or IFN- that could be hypothesized from our data regarding melanoma stages. In fact, while CCL3 increases with disease progression from stage I to stage IV, IL-10 and IFN- appear to be higher in stage I, and slowly decrease in parallel to CCL3 build up.
Discussion
Several studies in the past 15 years have concluded that multiplexed analysis of serum biomarkers may be useful for the evaluation of clinical outcome as well as potentially predictive of response to therapy [58, 59, 60]. However, the panels investigated varied markedly and the cytokine markers indicated differed among the studies, most of them evaluating longitudinal changes after treatment in just one or few molecules [61, 62, 63, 64]. An exception is represented by Neagu and coworkers who analyzed up to 6 cytokines in over 100 cases followed for up to 3 years [65].
Of the 12 analyzed in our study, 4 cytokines (IL-10, IFN-, CCL3 and CCL4) were demonstrated to be significantly higher in melanoma patients when compared to HC. In particular, IL-10 levels, higher in melanoma patients than in HC, confirmed its role in the evasion of immune-surveillance [66, 67, 68, 69]. IFN- decrease from stage I to stages II–IV reflects the importance of interferons in boosting the anti-tumor immune response [70, 71, 72]. Further studies are needed to assess whether both type I and type II endogenous interferons decrease together with disease progression and to justify the use of IFN-a as an adjuvant therapy for high-risk patients [73]. CCL-3 and CCL-4, also known as MIP-1 and MIP-1, are monokines with inflammatory and chemotactic properties [74]. They are generally produced by innate immunity cells, but CD8 T-cells can as well produce them as they were first discovered as HIV-suppressive factors [75]. Their role in cancer and in the anti-tumor response is still not well-known [76, 77].
IL2 and IL4 levels tend to decrease with disease progression. Despite not statistically significant, those results reflect the reduction in the anti-tumor T-cell response with disease progression, both Th1 and Th2 [57, 78]. IL8 is a chemokine well-known to be related to a metastatic phenotype: despite not statistically significant, it is increased in stage IV-patient sera [79, 80, 81].
Our results expand observations made in several previous studies which focused on a more limited number of molecules, and for those already reported confirms some observations (as for IFN- and IL-8) regarding changes in different stages [82, 83]. This extended panel of cytokines examines for the first time the potential roles of type2 cytokines (such as IL-4) and many chemokines (mainly CCL3) in melanoma progression and for the assessment of the patients’ immune status. Data regarding MIP are of particular interest: if the version attracts mainly NK and monocytes, the form attracts mainly neutrophils, our results emphasizing thus on the intense inflammatory status of the patients. Since the main limit of the study is probably the small number of patients screened, we strongly encourage the use of this particular panel of cytokines in a larger population.
More data are needed to confirm the trends of mean cytokine and chemokine levels observed among different disease stages and to better define cytokine role in cancer development and spreading [84].
Footnotes
Conflict of interest
none.
Supplementary materials
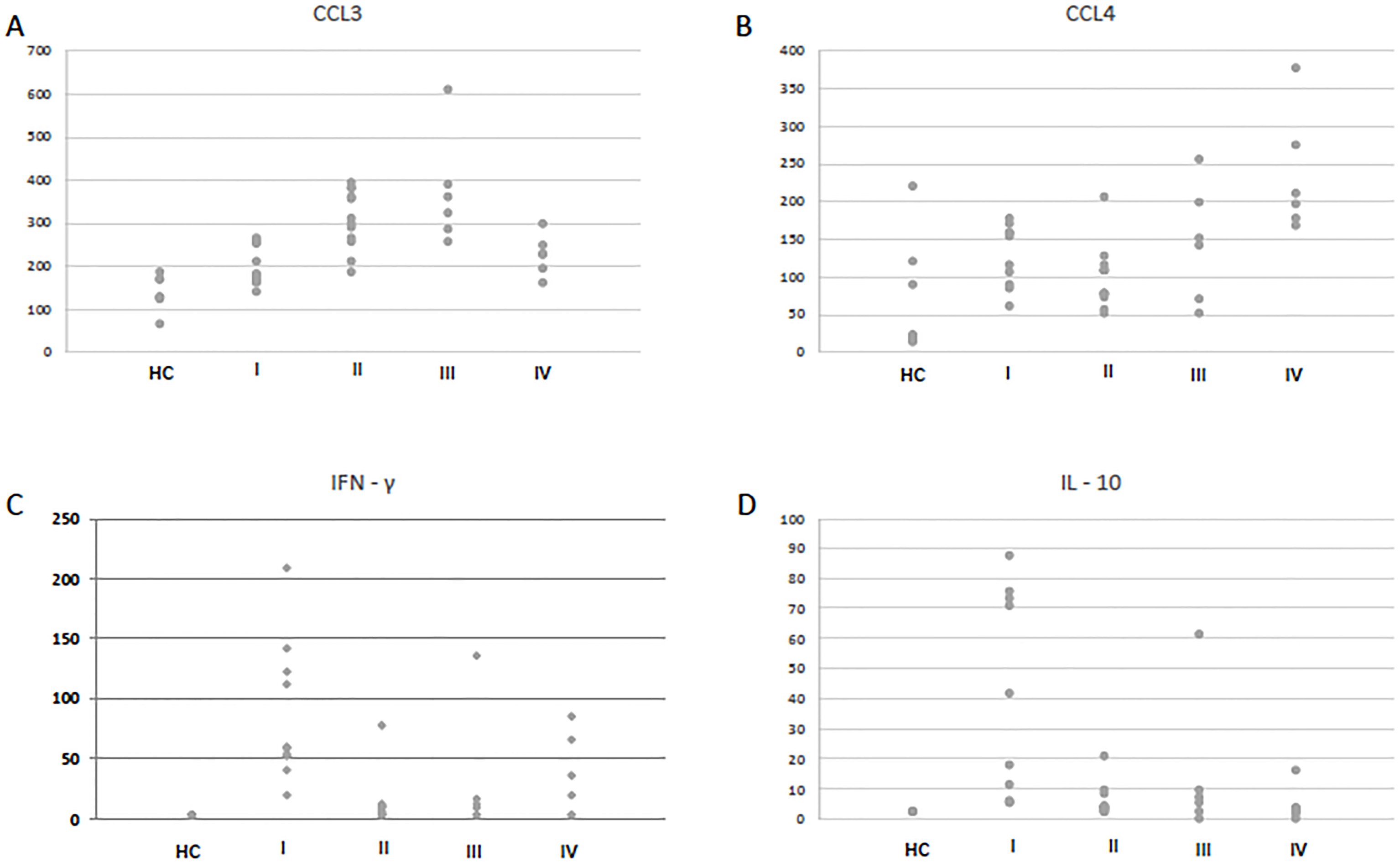
Dot plot showing CCL4, CCL3, IFN- and IL-10 serum levels of the single subjects enrolled in the study (measured in pg/ml).
References
1.
TrippM.K.WatsonM.BalkS.J.SwetterS.M. and GershenwaldJ.E., State of the science on prevention and screening to reduce melanoma incidence and mortality: the time is now, CA. Cancer J. Clin. (May 2016).
2.
FerlayJ. et al., Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018, Eur. J. Cancer Oxf. Engl. 1990103 (Nov. 2018), 356–387.
3.
BrayF.FerlayJ.SoerjomataramI.SiegelR.L.TorreL.A. and JemalA., Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries, CA. Cancer J. Clin.68(6) (Sep. 2018), 394–424.
4.
ApallaZ.LallasA.SotiriouE.LazaridouE. and IoannidesD., Epidemiological trends in skin cancer, Dermatol. Pract. Concept.7(2) (Apr. 2017), 1–6.
5.
GandhiS.A. and KamppJ., Skin cancer epidemiology, detection, and management, Med. Clin. North Am.99(6) (Nov. 2015), 1323–1335.
6.
CustA.E. et al., Sunbed use during adolescence and early adulthood is associated with increased risk of early-onset melanoma, Int. J. Cancer J. Int. Cancer128(10) (May 2011), 2425–2435.
7.
AschaM.AschaM.S.TanenbaumJ. and BordeauxJ.S., Risk factors for melanoma in renal transplant recipients, JAMA Dermatol.153(11) (Nov. 2017), 1130–1136.
8.
CustA.E. et al., MC1R genotypes and risk of melanoma before age 40 years: a population-based case-control-family study, Int. J. Cancer J. Int. Cancer131(3) (Aug. 2012), E269–E281.
9.
TarhiniA.A.LoriganP. and LeachmanS., Operable melanoma: screening, prognostication, and adjuvant and neoadjuvant therapy, Am. Soc. Clin. Oncol. Educ. Book Am. Soc. Clin. Oncol. Annu. Meet.37 (2017), 651–660.
10.
FongZ.V. and TanabeK.K., Comparison of melanoma guidelines in the U.S.A., Canada, Europe, Australia and New Zealand: a critical appraisal and comprehensive review, Br. J. Dermatol.170(1) (Jan. 2014), 20–30.
11.
et al.Guidelines of care for the management of primary cutaneous melanoma, J. Am. Acad. Dermatol.(Oct. 2018).
12.
BrancaccioG. et al., Eighth American Joint Committee on Cancer (AJCC) melanoma classification: what about stage IIC? Br. J. Dermatol. (Oct. 2018).
13.
Abdel-RahmanO., Evaluation of the eighth American Joint Committee on Cancer staging system for malignant melanoma of the skin, Future Oncol.14(5) (Feb. 2018), 471–481.
14.
BolandG.M. and GershenwaldJ.E., Principles of Melanoma Staging, in MelanomaKaufmanH.L. and MehnertJ.M., Eds. Cham: Springer International Publishing, Vol. 167, 2016, pp. 131–148.
15.
GershenwaldJ.E. et al., Melanoma staging: evidence-based changes in the american joint committee on cancer eighth edition cancer staging manual, CA. Cancer J. Clin.67(6) (Nov. 2017), 472–492.
16.
HomsiJ.Kashani-SabetM.MessinaJ.L. and DaudA., Cutaneous melanoma: prognostic factors, Cancer Control J. Moffitt Cancer Cent.12(4) (Oct. 2005), 223–229.
17.
ClementeC.G.MihmM.C.BufalinoR.ZurridaS.ColliniP. and CascinelliN., Prognostic value of tumor infiltrating lymphocytes in the vertical growth phase of primary cutaneous melanoma, Cancer77(7) (Apr. 1996), 1303–1310.
18.
CamisaschiC.VallacchiV.CastelliC.RivoltiniL. and RodolfoM., Immune cells in the melanoma microenvironment hold information for prediction of the risk of recurrence and response to treatment, Expert Rev. Mol. Diagn.14(6) (Jul. 2014), 643–646.
19.
Zito MarinoF. et al., Are tumor-infiltrating lymphocytes protagonists or background actors in patient selection for cancer immunotherapy? Expert Opin. Biol. Ther.17(6) (2017), 735–746.
20.
SamaniegoR. et al., CCL20 expression by tumor-associated macrophages predicts progression of human primary cutaneous melanoma, Cancer Immunol. Res. (Jan. 2018).
21.
MauldinI.S. et al., Intratumoral interferon-gamma increases chemokine production but fails to increase T cell infiltration of human melanoma metastases, Cancer Immunol. Immunother.65(10) (Oct. 2016), 1189–1199.
22.
KnightD.A. et al., Host immunity contributes to the anti-melanoma activity of BRAF inhibitors, J. Clin. Invest.123(3) (Mar. 2013), 1371–1381.
23.
SurcelM.ConstantinC.CaruntuC.ZuracS. and NeaguM., Inflammatory cytokine pattern is sex-dependent in mouse cutaneous melanoma experimental model, J. Immunol. Res.2017 (2017), 1–10.
24.
ZhangX. et al., A vaccine targeting basic fibroblast growth factor elicits a protective immune response against murine melanoma, Cancer Biol. Ther.19(6) (Jun. 2018), 518–524.
25.
KooremanN.G. et al., Autologous iPSC-based vaccines elicit anti-tumor responses in vivo, Cell Stem Cell22(4) (Apr. 2018), 501–513.e7.
26.
MaraveyasA. et al., Possible improved survival of patients with stage IV AJCC melanoma receiving SRL 172 immunotherapy: correlation with induction of increased levels of intracellular interleukin-2 in peripheral blood lymphocytes, Ann. Oncol. Off. J. Eur. Soc. Med. Oncol.10(7) (Jul. 1999), 817–824.
27.
RedondoP.Sánchez-CarpinteroI.BauzáA.IdoateM.SolanoT. and MihmM.C., Immunologic escape and angiogenesis in human malignant melanoma, J. Am. Acad. Dermatol.49(2) (Aug. 2003), 255–263.
28.
BernengoM.G.QuaglinoP.CappelloN.LisaF.Osella-AbateS. and FierroM.T., Macrophage-mediated immunostimulation modulates therapeutic efficacy of interleukin-2 based chemoimmunotherapy in advanced metastatic melanoma patients, Melanoma Res.10(1) (Feb. 2000), 55–65.
29.
RaymanP. et al., Tumor-induced dysfunction in interleukin-2 production and interleukin-2 receptor signaling: a mechanism of immune escape, Cancer J. Sci. Am.6(Suppl 1) (Feb. 2000), S81–87.
30.
FumagalliL.A.VinkeJ.HoffW.YpmaE.BrivioF. and NespoliA., Lymphocyte counts independently predict overall survival in advanced cancer patients: a biomarker for IL-2 immunotherapy, J. Immunother. Hagerstown Md 199726(5) (Oct. 2003), 394–402.
31.
IzraelyS. et al., The metastatic microenvironment: melanoma-microglia cross-talk promotes the malignant phenotype of melanoma cells, Int. J. Cancer (Jul. 2018).
32.
KleinA. et al., Astrocytes facilitate melanoma brain metastasis via secretion of IL-23: astrocytes facilitate melanoma brain metastasis via IL-23, J. Pathol.236(1) (May 2015), 116–127.
33.
Di GiacomoA.M.ValenteM.CovreA.DanielliR. and MaioM., Immunotherapy targeting immune check-point(s) in brain metastases, Cytokine Growth Factor Rev.36 (Aug. 2017), 33–38.
34.
WestphalD.Glitza OlivaI.C. and NiessnerH., Molecular insights into melanoma brain metastases: insights into melanoma brain metastases, Cancer123(S11) (Jun. 2017), 2163–2175.
35.
UsuiY. et al., Aqueous immune mediators in malignant uveal melanomas in comparison to benign pigmented intraocular tumors, Graefes Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Klin. Exp. Ophthalmol.255(2) (Feb. 2017), 393–399.
36.
FranklinC.LivingstoneE.RoeschA.SchillingB. and SchadendorfD., Immunotherapy in melanoma: recent advances and future directions, Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol.43(3) (Mar. 2017), 604–611.
37.
HerzbergB. and FisherD.E., Metastatic melanoma and immunotherapy, Clin. Immunol. Orlando Fla172 (Nov. 2016), 105–110.
38.
SanlorenzoM. et al., Melanoma immunotherapy, Cancer Biol. Ther.15(6) (Jun. 2014), 665–674.
39.
CirenajwisH. et al., Molecular stratification of metastatic melanoma using gene expression profiling: prediction of survival outcome and benefit from molecular targeted therapy, Oncotarget6(14) (May 2015).
40.
KoguchiY. et al., Serum immunoregulatory proteins as predictors of overall survival of metastatic melanoma patients treated with ipilimumab, Cancer Res.75(23) (Dec. 2015), 5084–5092.
41.
FoleyK.C.NishimuraM.I. and MooreT.V., Combination immunotherapies implementing adoptive T-cell transfer for advanced-stage melanoma, Melanoma Res. (Mar. 2018), 1.
42.
VihinenP. et al., Serum angiogenin levels predict treatment response in patients with stage IV melanoma, Clin. Exp. Metastasis24(7) (Oct. 2007), 567–574.
43.
NeaguM.ConstantinC.MandaG. and MargaritescuI., Biomarkers of metastatic melanoma, Biomark. Med.3(1) (Feb. 2009), 71–89.
44.
FangS. et al., C-reactive protein as a marker of melanoma progression, J. Clin. Oncol.33(12) (Apr. 2015), 1389–1396.
45.
YamazakiN. et al., Cytokine biomarkers to predict antitumor responses to nivolumab suggested in a phase 2 study for advanced melanoma, Cancer Sci.108(5) (May 2017), 1022–1031.
46.
BoyanoM.D. et al., Soluble interleukin-2 receptor, intercellular adhesion molecule-1 and interleukin-10 serum levels in patients with melanoma, Br. J. Cancer83(7) (Oct. 2000), 847–852.
47.
MorettiS. et al., Serum imbalance of cytokines in melanoma patients, Melanoma Res.11(4) (Aug. 2001), 395–399.
48.
NeaguM.ConstantinC. and TanaseC., Immune-related biomarkers for diagnosis/prognosis and therapy monitoring of cutaneous melanoma, Expert Rev. Mol. Diagn.10(7) (Oct. 2010), 897–919.
49.
GrimmE.A.SmidC.M.LeeJ.J.TsengC.H.EtonO. and BuzaidA.C., Unexpected cytokines in serum of malignant melanoma patients during sequential biochemotherapy, Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res.6(10) (Oct. 2000), 3895–3903.
50.
ChenL.HuangC.ShengY. and JiaJ., Identification of melanoma biomarkers based on network modules by integrating the human signaling network with microarrays, J. Cancer Res. Ther.10(7) (2014), 114.
51.
HarbstK. et al., Molecular profiling reveals low- and high-grade forms of primary melanoma, Clin. Cancer Res.18(15) (Aug. 2012), 4026–4036.
52.
Kashani-SabetM., Molecular markers in melanoma, Br. J. Dermatol.170(1) (Jan. 2014), 31–35.
53.
DengelL.T. et al., Interferons induce CXCR3-cognate chemokine production by human metastatic melanoma, J. Immunother.33(9) (Nov. 2010), 965–974.
54.
ChenQ.DanielV.MaherD.W. and HerseyP., Production of IL-10 by melanoma cells: examination of its role in immunosuppression mediated by melanoma, Int. J. Cancer56(5) (Mar. 1994), 755–760.
55.
NemunaitisJ.FongT.ShabeP.MartineauD. and AndoD., Comparison of serum interleukin-10 (IL-10) levels between normal volunteers and patients with advanced melanoma, Cancer Invest.19(3) (2001), 239–247.
56.
LucaM.HuangS.GershenwaldJ.E.SinghR.K.ReichR. and Bar-EliM., Expression of interleukin-8 by human melanoma cells up-regulates MMP-2 activity and increases tumor growth and metastasis, Am. J. Pathol.151(4) (Oct. 1997), 1105–1113.
57.
KuceraR. et al., Evaluation of IL-2, IL-6, IL-8 and IL-10 in malignant melanoma diagnostics, Anticancer Res.35(6) (Jun. 2015), 3537–3541.
58.
LeeJ.H.ChenY.ChanJ.L.QianY. and GoydosJ.S., Molecular analysis of melanoma-induced sentinel lymph node immune dysfunction, Cancer Immunol. Immunother.60(5) (May 2011), 685–692.
59.
NeaguM., The immune system – a hidden treasure for biomarker discovery in cutaneous melanoma, Adv. Clin. Chem.58 (2012), 89–140.
60.
NeaguM.ConstantinC. and LongoC., Chemokines in the melanoma metastasis biomarkers portrait, J. Immunoassay Immunochem.36(6) (Nov. 2015), 559–566.
61.
KaliaM., Biomarkers for personalized oncology: recent advances and future challenges, Metabolism64(3) (Mar. 2015), S16–S21.
62.
YurkovetskyZ.R. et al., Multiplex analysis of serum cytokines in melanoma patients treated with interferon-alpha2b, Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res.13(8) (Apr. 2007), 2422–2428.
63.
JamalR. et al., Peripheral and local predictive immune signatures identified in a phase II trial of ipilimumab with carboplatin/paclitaxel in unresectable stage III or stage IV melanoma, J. Immunother. Cancer5(1) (Dec. 2017).
64.
SanmamedM.F. et al., Changes in serum interleukin-8 (IL-8) levels reflect and predict response to anti-PD-1 treatment in melanoma and non-small-cell lung cancer patients, Ann. Oncol. Off. J. Eur. Soc. Med. Oncol.28(8) (Aug. 2017), 1988–1995.
65.
NeaguM.ConstantinC. and ZuracS., Immune parameters in the prognosis and therapy monitoring of cutaneous melanoma patients: experience, role, and limitations, BioMed Res. Int.2013 (2013), 1–13.
66.
DummerW.BastianB.C.ErnstN.SchänzleC.SchwaafA. and BröckerE.-B., Interleukin-10 production in malignant melanoma: preferential detection of IL-10-secreting tumor cells in metastatic lesions, Int. J. Cancer66(5) (May 1996), 607–610.
67.
WigunaA.P. and WaldenP., Role of IL-10 and TGF-β in melanoma, Exp. Dermatol.24(3) (Mar. 2015), 209–214.
68.
Torisu-ItakuraH.LeeJ.H.HuynhY.YeX.EssnerR. and MortonD.L., Monocyte-derived IL-10 expression predicts prognosis of stage IV melanoma patients, J. Immunother.30(8) (Nov. 2007), 831–838.
69.
GerliniG.Tun-KyiA.DudliC.BurgG.PimpinelliN. and NestleF.O., Metastatic melanoma secreted IL-10 down-regulates CD1 molecules on dendritic cells in metastatic tumor lesions, Am. J. Pathol.165(6) (Dec. 2004), 1853–1863.
70.
VuletićA. et al., Decreased interferon γ production in CD3+ and CD3-CD56+ lymphocyte subsets in metastatic regional lymph nodes of melanoma patients, Pathol. Oncol. Res.21(4) (Sep. 2015), 1109–1114.
71.
SchmittM.J. et al., Interferon-γ-induced activation of Signal Transducer and Activator of Transcription 1 (STAT1) up-regulates the tumor suppressing microRNA-29 family in melanoma cells, Cell Commun. Signal.10(1) (2012), 41.
72.
RespaA. et al., Association of IFN-signal transduction defects with impaired HLA class I antigen processing in melanoma cell lines, Clin. Cancer Res.17(9) (May 2011), 2668–2678.
73.
SinghR.K.GutmanM.LlansaN. and FidlerI.J., Interferon-β prevents the upregulation of interleukin-8 expression in human melanoma cells, J. Interferon Cytokine Res.16(8) (Aug. 1996), 577–584.
74.
MaurerM. and von StebutE., Macrophage inflammatory protein-1, Int. J. Biochem. Cell Biol.36(10) (Oct. 2004), 1882–1886.
75.
AnsariA.W.HeikenH.MoenkemeyerM. and SchmidtR.E., Dichotomous effects of C-C chemokines in HIV-1 pathogenesis, Immunol. Lett.110(1) (May 2007), 1–5.
76.
NakasoneY. et al., Host-derived MCP-1 and MIP-1α regulate protective anti-tumor immunity to localized and metastatic B16 melanoma, Am. J. Pathol.180(1) (Jan. 2012), 365–374.
77.
SchallerT.H.BatichK.A.SuryadevaraC.M.DesaiR. and SampsonJ.H., Chemokines as adjuvants for immunotherapy: implications for immune activation with CCL3, Expert Rev. Clin. Immunol.13(11) (2017), 1049–1060.
78.
SonD.J. et al., Activated natural killer cells mediate the suppressive effect of interleukin-4 on tumor development via STAT6 activation in an atopic condition melanoma model, Neoplasia N. Y. N19(7) (Jul. 2017), 537–548.
79.
ZhangH. et al., IL8 and cathepsin B as melanoma serum biomarkers, Int. J. Mol. Sci.12(3) (Feb. 2011), 1505–1518.
80.
PengH.-H.LiangS.HendersonA.J. and DongC., Regulation of interleukin-8 expression in melanoma-stimulated neutrophil inflammatory response, Exp. Cell Res.313(3) (Feb. 2007), 551–559.
81.
EneC.-D.AnghelA.-E.NeaguM. and NicolaeI., 25-OH vitamin D and interleukin-8: emerging biomarkers in cutaneous melanoma development and progression, Mediators Inflamm.2015 (2015), 1–8.
82.
ArgirisA. et al., Serum biomarkers as potential predictors of antitumor activity of cetuximab-containing therapy for locally advanced head and neck cancer, Oral Oncol.47(10) (Oct. 2011), 961–966.
83.
ThurneysenS. et al., An exploratory study investigating the metabolic activity and local cytokine profile in patients with melanoma treated with pazopanib and paclitaxel, Br. J. Dermatol.175(5) (Nov. 2016), 966–978.
84.
YoungH.L. et al., An adaptive signaling network in melanoma inflammatory niches confers tolerance to MAPK signaling inhibition, J. Exp. Med.214(6) (5 2017), 1691–1710.