
Abstract
OBJECTIVE
: The aim of this study was to evaluate the prognostic value of a novel tumor marker index (TMI) based on preoperative serum levels of squamous cell carcinoma antigen (SCC) and cytokeratin 19 fragment (CYFRA 21-1) for patients with resectable esophageal squamous cell carcinoma (ESCC).
METHODS:
A total of 315 ESCC patients who had underwent curative surgery between 2008 and 2012 were retrospectively included in this study. The TMI was defined as the geometric mean of normalized SCC and CYFRA21-1 levels. Univariate and multivariate survival analyses were performed to confirm the clinical and prognostic significance of preoperative SCC and CYFRA 21-1 levels and TMI.
RESULTS:
Elevated preoperative SCC was associated with histological grade, pT status, lymph node status and TNM stage. Elevated preoperative CYFRA 21-1 was correlated with tumor size, lymph node status and TNM stage. The overall survival of patients with elevated SCC and CYFRA 21-1 levels was significantly poorer than that of patients with normal levels. Multivariate survival analysis identified that preoperative SCC (
CONCLUSIONS:
Elevated preoperative SCC and CYFRA 21-1 levels were associated with aggressive cancer behavior in ESCC. The TMI based on preoperative SCC and CYFRA 21-1 might serve as a novel marker that can be used to predict the prognosis of ESCC patients.
Introduction
In China, esophageal cancer is the sixth leading cause of cancer-related death, and the pathological type of more than 90% of cases is squamous cell carcinoma [1]. Despite recent advances in surgical techniques and multimodal therapy, the prognosis remains poor due to the high rate of recurrence and metastasis. Patients at high risk of recurrence after curative surgery often have a poor prognosis [2]. Therefore, studies should focus on the identification of suitable biomarkers associated with survival in patients with esophageal squamous cell carcinoma (ESCC) and facilitate prognostic prediction and selection of patients who will benefit from aggressive postoperative treatment [3, 4].
Peripheral serum tumor makers produced by tumor cells are noninvasive diagnostic tools that are commonly used to identify cancer and to assess tumor progression and survival [5, 6]. To date, SCC, which is a tumor-associated antigen, and a fragment of cytokeratin 19 (CYFRA 21-1) are two tumor biomarkers that have been most commonly used to predict the long-term survival of patients with esophageal cancer [7, 8]. However, the sensitivities and specificities of these two tumor markers are unacceptably low, and as a result, there has been controversy over the clinical use of these tumor markers. Therefore, if these tumor markers are used in combination, the prognostic significance of these tumor markers might be more accurate than when used individually. Previously, Muley et al. [9] introduced an algorithm known as the tumor marker index (TMI), which increased the prognostic sensitivity in stage I non-small cell lung cancer (NSCLC) patients. In addition, the TMI corresponding to the geometric means of the levels of normalized CYFRA 21-1 and carcinoembryonic antigen (CEA) not only combined the use of these two markers but also could be used to evaluate the degree of marker elevation [9]. Therefore, it may be desirable to use a similar TMI combination based on SCC and CYFRA 21-1 to predict prognosis in ESCC.
In this study, we investigated the association of the preoperative tumor markers (SCC and CYFRA 21-1) with clinicopathological factors and prognosis in patients with ESCC. Furthermore, a novel TMI based on preoperative SCC and CYFRA 21-1 was established to evaluate the prognosis of patients with resectable ESCC.
Patients and methods
Patients
A consecutive series of 315 patients with histologically confirmed ESCC who underwent curative surgery at the Cancer Institute and Hospital of Tianjin Medical University from January 2008 to December 2012 were retrospectively included. The eligibility criteria included (i) histopathological confirmation of esophageal squamous cell carcinoma; (ii) did not receive neoadjuvant treatment; (iii) complete tumor resection, negative incision margins and no distant metastasis; and (iv) absence of other malignant tumors besides ESCC. The depth of tumor invasion, degree of lymph node infiltration and tumor-node-metastasis (TNM) staging were defined according to UICC/AJCC TNM classification (7th edition) [10]. Histological grade was defined according to the World Health Organization classification of esophageal tumors [11]. This study was approved by the Research Ethics Committee of Tianjin Medical University Cancer Institute. All patients gave written informed consent.
The associations between the SCC level, CYFRA 21-1 level and the clinicopathological factors in 315 patients with ESCC
The associations between the SCC level, CYFRA 21-1 level and the clinicopathological factors in 315 patients with ESCC
SCC: Squamous cell carcinoma antigen; CYFRA21-1: Cytokeratin 19 fragment; ESCC: Esophageal squamous cell carcinoma; TNM: Tumor-node-metastasis.
Blood specimens were drawn within 1 week prior to surgery, and the serum SCC and CYFRA 21-1 were detected by commercially available enzyme immunoassays with a Cobas Core analyzer (Roche Diagnostics, Mannheim, Germany) at the clinical laboratory. The normal upper limits were 1.5
TMI
The TMI was calculated as previously described [9]. In the present study, the TMI was defined by determining the geometric mean of the normalized values of the serum SCC concentration and serum CYFRA 21-1 concentration. Normalization was performed by dividing the individual marker values by the corresponding diagnostic cut-off points, which were 1.5
Statistical analysis
A chi-square test was employed to analyze the relationship between the levels of serum SCC and CYFRA 21-1 and the clinicopathological characteristics. Spearman’s correlation analyses were conducted to analyze the associations of SCC and CYFRA with TMI. A receiver operating characteristic (ROC) curve was used to determine the cut-off value of TMI used for prognostic prediction. Survival time was calculated from the date of operation until the date of death or last date of contact. The hazard ratio (HR) and 95% confidence interval (CI) within each subgroup were summarized for the subgroup analysis of overall survival. Univariate analysis of survival data was performed using the Kaplan-Meier method. Multivariate survival analysis was performed using Cox proportional hazard regression.
Univariate and multivariate analyses of clinical and pathological variables associated with overall survival in 315 patients with ESCC (Model 1)
Univariate and multivariate analyses of clinical and pathological variables associated with overall survival in 315 patients with ESCC (Model 1)
SCC: Squamous cell carcinoma antigen; CYFRA21-1: Cytokeratin 19 fragment; ESCC: Esophageal squamous cell carcinoma; HR: Hazard ratio; CI: Confidence interval.
Kaplan-Meier survival curves based on preoperative SCC and CYFRA 21-1 levels in patients with ESCC. A: Preoperative SCC level; B: Preoperative CYFRA 21-1 level. 
Patient and disease characteristics
The clinicopathological characteristics of the study patients are summarized in Table 1. The median age of the 315 included ESCC patients was 61 years (range: 33 to 85 years). Two hundred sixty-one (82.9%) were males, and 54 (17.1%) were females. The tumors were located in the upper 1/3 in 18 (5.7%) patients, in the middle 1/3 in 219 (69.5%) patients and in the lower 1/3 in 78 (24.8%) patients. There were 147 (46.7%) patients with stage I and II ESCC and 168 (53.3%) patients with stage III ESCC.
The associations of preoperative serum SCC and CYFRA 21-1 levels with clinicopathological characteristics
The preoperative serum levels of SCC and CYFRA 21-1 were considered to be elevated when they exceeded 1.5 ug/L and 3.3 ug/L, respectively. Within the whole cohort, high serum levels of SCC and CYFRA 21-1 were found in 49/315 (15.6%) and 83/315 of patients (26.3%), respectively (Table 1). There were significant associations between the preoperative SCC serum level and histological grade (
The prognostic value of preoperative serum SCC and CYFRA 21-1 levels
The 5-year overall survival rate for the patients with a high SCC level was 29.7%, which was significantly lower than that for patients with a normal SCC level (42.8%,
All significant prognostic factors tested with univariate analysis were further evaluated with multivariate analysis. The results demonstrated that tumor size (HR 1.478; 95% CI 1.092-2.000;
Multivariate analysis of prognostic factors in 315 patients with ESCC (Model 2)
Multivariate analysis of prognostic factors in 315 patients with ESCC (Model 2)
ESCC: Esophageal squamous cell carcinoma; TMI: Tumor marker index; HR: Hazard ratio; CI: Confidence interval.
Cumulative survival curves for 315 patients with ESCC based on TMI by Kaplan-Meier survival analysis. The 5-year OS rates for the low-and high-TMI groups were 50.4% and 30.9%, respectively (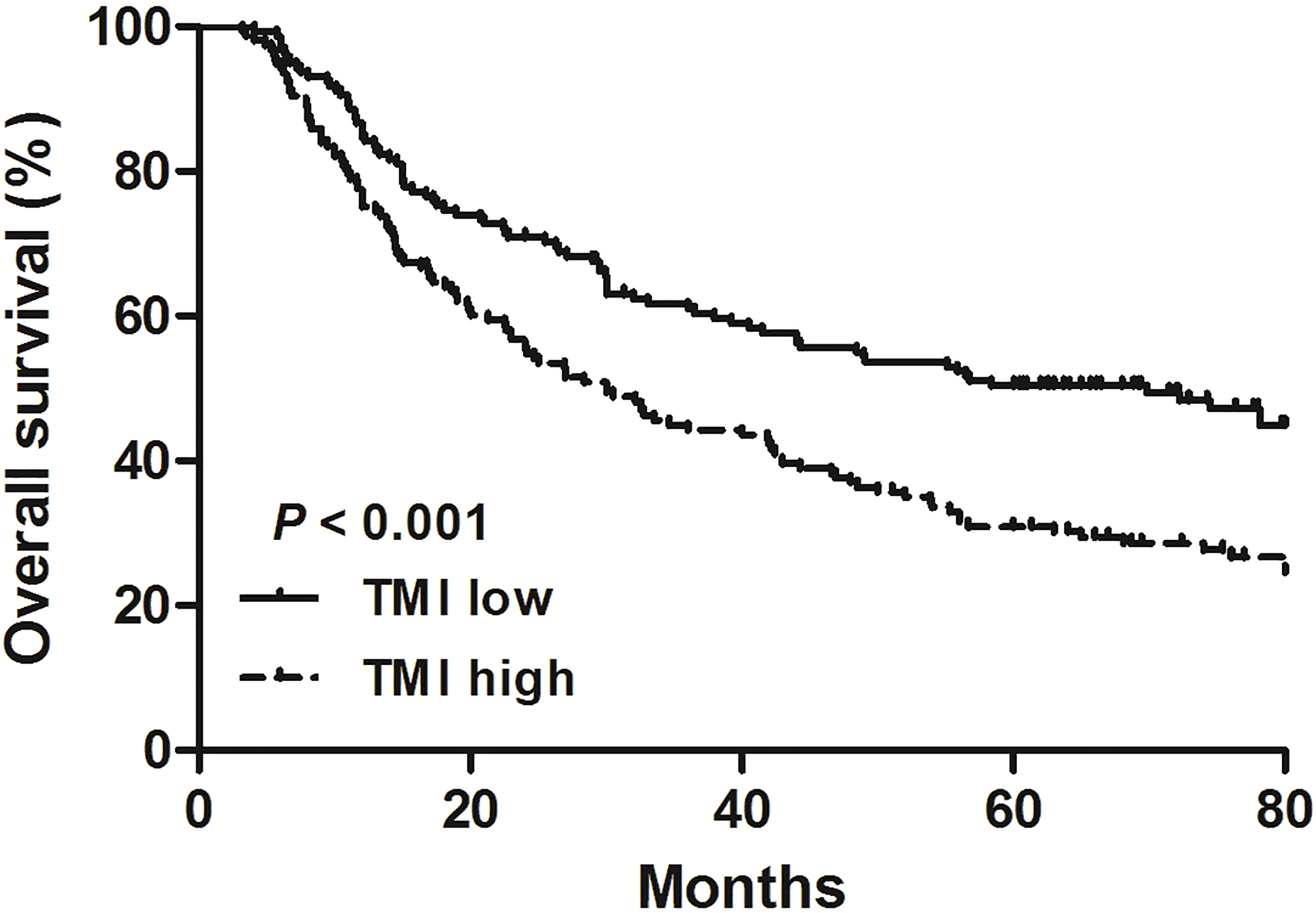
As first described by Muley et al. [9], the TMI and the geometric means of the normalized SCC and CYFRA 21-1 levels were introduced into our analysis. Spearman’s correlation analyses showed that, TMI was positively correlated with SCC and CYFRA 21-1 (
The prognostic value of the TMI based on SCC and CYFRA 21-1
Based on the ROC curve, the best cut-off value for the TMI was 0.531 (sensitivity: 67.86%; specificity: 60.48%). Using this TMI cut-off value, we subdivided the patients into 2 groups: those with a TMI less than or equal to 0.531 and those with a TMI greater than 0.531. There were 158 patients (64.2%) in the low TMI group and 157 patients (35.8%) in the high TMI group. The 5-year survival rate for patients in the low TMI group was 50.4% compared to 30.9% for patients in the high TMI group, and there was a significant difference between the two groups (
After the SCC and CYFRA 21-1 were combined into the new variable, TMI, these significant predictors were included in the final Cox proportional hazards model. As summarized in Table 3, tumor size (HR 1.477; 95% CI 1.095–1.991;
Subgroup analysis
We further stratified the patients into groups according to pT status (T1-T2 and T3-T4), lymph node status (N0 and N+), and tumor stage (stage I-II and stage III). Our results showed that the TMI could be used to separate the patients into two independent groups in the T1-T2 (
Cumulative survival curves based on preoperative SCC and CYFRA 21-1 levels for ESCC patients with different clinicopathological features. (A) Cumulative survival for patients with T1-T2 status. (B) Cumulative survival for patients with T3-T4 status. (C) Cumulative survival for patients without lymph node metastasis. (D) Cumulative survival for patients with lymph node metastasis. (E) Cumulative survival for patients with pTNM stage I-II. (F) Cumulative survival for patients with pTNM stage III.
Although the incidence rate of esophageal cancer has decreased in recent years, the overall 5-year survival rate remains relatively low [12]. In addition, it is well known that there are substantial differences in survival between patients with cancer at the same TNM stage [13]. Therefore, there is an urgent need to identify valuable biomarkers for the early identification of ESCC patients who are at risk and have poor prognosis. Tumor markers are attracting such attention and have potential use for diagnosis, treatment monitoring and the determination of prognosis [6].
SCC, which is isolated from cervical SCC, has been commonly used as a tumor marker for ESCC. Previous studies have shown that elevated SCC levels were associated with tumor progression and adverse prognosis for patients with ESCC [14, 15]. CYFRA 21-1, a member of the keratin family, is a protein that is encoded by the KRT19 gene [16]. It is overexpressed in many malignant cancers, such as lung cancer [17], colorectal cancer [18] and breast cancer [19]. Recently, CYFRA 21-1 was reported to promote cell growth, adhesion, migration and invasion [20]. Yamamoto et al. [21] reported that the sensitivity and specificity of CYFRA 21-1 concentrations were 47.9% and 100%, respectively, in patients with ESCC. In addition, an association between the serum CYFRA 21-1 level and advanced cancer stage and survival has also been observed [22]. Therefore, in the present study, we evaluated the associations between preoperative serum SCC and CYFRA 21-1 levels and clinicopathological parameters and prognosis in ESCC patients. Our results revealed that elevated preoperative levels of SCC and CYFRA 21-1 indicated advanced disease in patients with ESCC. Our findings are consistent with those from studies by Kosugi et al. [15] and Cao et al. [13]. Furthermore, we analyzed the prognostic value of preoperative SCC and CYFRA 21-1 levels. Univariate analysis showed that elevated preoperative SCC and CYFRA 21-1 levels were associated with worse outcomes in patients with ESCC. However, we failed to demonstrate the independent prognostic value of the SCC and CYFRA 21-1 levels by multivariate analysis. To date, the use of serum markers has not been accepted for assessing prognosis in ESCC after curative surgery. The prognostic value of CYFRA 21-1 and SCC are also still controversial [13]. Indeed, clinical use of only a single positive tumor marker for prognostic evaluation may be difficult because of the lack of high sensitivity [23]. Yamamoto et al. [21] reported that the sensitivity rates of SCC and CYFRA 21-1 in ESCC were 25.0% and 47.9%, respectively. Therefore, to evaluate the prognostic predictive value of the two markers more accurately, the combined use of serum SCC and CYFRA 21-1 levels may be needed to increase the sensitivity and thereby allow useful prognostic determination.
Previously, Muley et al. [9] introduced an algorithm based on the serum CYFRA 21-1 and CEA levels. The variable known as the tumor marker index (TMI), which corresponds to the geometric mean of the normalized CYFRA 21-1 and CEA levels (the marker value divided by the diagnostic cut-off), served as an independent prognostic factor for stage I NSCLC. Furthermore, it is sometimes difficult to evaluate the prognosis of patients with a single positive tumor marker. Therefore, a similar TMI variable, which was introduced by Muley et al. [9] and can be used to evaluate two markers simultaneously, was used in our present study. The TMI in the present study was based on preoperative SCC and CYFRA 21-1 levels that correspond to the geometric mean of the normalized SCC and CYFRA 21-1 levels. The optimal cut-off level of TMI was established by using ROC curves, and the selected cut-off value was 0.531. Patients were subdivided into two groups: patients with a high TMI (TMI
The measurement of serum SCC and CYFRA 21-1 levels is inexpensive, noninvasive and routinely available in the clinic. Although a previous study investigated the use of a more sensitive SCC mRNA method to predict prognosis in esophageal cancer [24], this method of molecular detection is expensive and routinely available only for researchers. The present results demonstrated the independent prognostic role of the TMI based on serum SCC and CYFRA 21-1 levels in ESCC patients. The TMI may serve as a new variable for prognostic prediction in ESCC patients. Patients with a high TMI represent a subgroup who might benefit from aggressive postoperative treatment.
However, there are some limitations in the present study. First, data for patients in this study were collected from a single institutional database; thus, the extent of selection bias might be underestimated. Second, it includes only a single retrospective study, and errors and biases inherent in its design may inevitably affect the results. Thirdly, instead of confirming the prognostic value of TMI in patients with ESCC, we could not make clear whether TMI can be used as a target for treatment of ESCC. Therefore, in the future, prospective studies with an expanded number of serum samples and patients are needed to verify these results. Finally, although the TMI index is a meaningful and more sensitive index that could be used noninvasively and routinely for the prediction of prognosis in ESCC, the TMI index is a less powerful prognostic factor than the TNM stage.
Preoperative SCC and CYFRA 21-1 levels were associated with advanced biological behavior in resectable ESCC patients. These two markers were not independent prognostic factors. We have provided the first evidence that the TMI, which is based on preoperative serum SCC and CYFRA 21-1 levels, served as an independent prognostic factor for ESCC patients who underwent curative surgery. The TMI may serve as a potential marker for prognostic prediction in ESCC. Further prospective studies with adequate sample sizes are needed to validate our results.
Footnotes
Acknowledgments
This study was supported by National Natural Science Foundation of China (81772619), Science Foundation of Tianjin Medical University (2016KYZM03).
Conflict of interest
The authors declare that there are no conflicts of interest.