
Abstract
BACKGROUND:
This study aimed to investigate the correlation of BRCA2 gene mutation and prognosis as well as variant genes in patients with invasive urothelial carcinoma of the bladder. It predicted and explored the possible mechanism and clinical value of BRCA2 in the occurrence and development of tumors.
METHODS:
Data sets of patients with bladder cancer were collected from the Cancer Genome Atlas (TCGA) database. Also the gene expression profile data and clinical information of the BRCA2 mutation group and non-BRCA2 mutation group were downloaded.
RESULTS:
The prognosis of the BRCA2 mutation group was better than that of the non-mutant group. Among the down-regulated genes, the following genes showed significant differences between the two groups: CCL22, CYP2B6, CYP2E1, CYP4F2, HTR1E, HTR1F, KLRC1, NAPSA, SELL, SFTPA1, SFTPA2, SFTPB, SFTPC and STRA8, while the following genes among the up-regulated genes showed significant differences between the two groups: ELAVL3, NOTUM, TRH and VIP. Meanwhile, the following gene sets were highly enriched in BRCA2: cell cycle, DNA replication, homologous recombination, oocyte meiosis, ubiquitin-mediated proteolysis, base excision repair, progestin mediated oocyte maturation, basal transcription factor, biosynthesis of N polysaccharide, mismatch repair, sliceosome, purine metabolism as well as P53 and neurotrophic factor signaling pathway, etc.
CONCLUSION:
These findings suggested that the BRCA2 gene mutation is a good prognostic factor and can be used as a gene to predict the prognosis in the bladder cancer patients.
Introduction
Bladder cancer is the ninth most common cancer worldwide, and each year over 430,000 new cases with bladder cancer were diagnosed. In developed developed country, the incidence rate of bladder cancer was 9.5/100,000, while more than 90% of these are urothelial carcinoma cases [1]. The incidence of bladder cancer is increasing with the development of the economy, and its recurrence rate has become a major economic burden on the health care systems [2]. In 2016, the standardized mortality rate for bladder cancer in males was 2–10/100,000 per year, and in females was 0.5–4/100000 per year [3]. The exact etiology of bladder cancer is still unknown. However, environmental factors, smoking, exposure to toxic industrial chemicals and gases, bladder inflammation caused by microorganisms, as well as gene mutations of bladder cells caused by drugs are associated with bladder cancer [4]. Gene mutation plays an important role in the occurrence and development of bladder cancer. It is well known that genes such as FGFR3, RB1, HRAS, TP53, TSC1 and so on can regulate the normal cell cleavage, and avoid generation of tumor cells. Hence, mutations in these genes can cause cancer [5]. Nickerson et al. [6] sequenced genes of 54 bladder cancer patients in the USA, and for the first time found that 15% of the patients had BAP1 mutation, and this led to the change in BRCA pathway, enabling the feature of papillary histological in bladder cancer. Font et al. [7] studied the correlation between the expression of BRCA1 mRNA and cisplatin based neoadjuvant chemotherapy response and prognosis, and found that the expression of BRCA1 mRNA could predict the sensitivity to chemotherapy and improve the prognosis in patients with bladder cancer. BRCA gene constitutes of BRCA1 and BRCA2 genes. Their main function is to repair genes from damage and prevent tumors from gene mutations, but they have different roles on the targets. The amino acid end of BRCA1 gene including histone H2AX can be phosphorylated by infrared exposure for a short period of time, repairing the damage of dsDNA and promote the remodeling of chromatin. Therefore, histone H2AX remains the major molecule for enabling BRCA1 gene to repair gene mutations [8]. Meanwhile, BRCA2 gene is performs the abovementioned repair through RAD51 instead of H2AX. A normal expression of RAD51 ensures its repair process, while overexpression or silence caused by BRCA2 gene mutation causes failure of the repair process [9].
The structure of the BRCA2 gene is complex and little is known about it at present. BRCA2 is a tumor suppressor gene, which plays an important role in the repair of DNA damage and regulation of cell growth. There is considerable evidence that BRCA2 gene was closely related to the development and prognosis of multiple tumors, such as breast cancer [10], ovarian cancer [11] and prostate cancer [12]. BRCA2 mutations fail to repair DNA duplex through homologous recombination, resulting in increased gene errors. Thus, BRCA2 mutation deteriorates the genomic stability and predisposes to malignant transformation [13]. It is still unclear whether the mutation state of the BRCA2 gene can be used as a prognostic factor in patients with invasive urothelial carcinoma of the bladder [13]. TCGA is a large research program initiated by National Cancer Institute of the United States and National Human Genome Research Institute organized by National Institutes of Health, which collected a large number of clinical information, tumor tissues and corresponding tissue samples for comprehensive analysis of genomic data [14]. Therefore, this study aimed to use the data from the TCGA database to explore the relationship between BRCA2 gene mutation and prognosis in patients with invasive urothelial carcinoma of the bladder.
BRCA2 mutation sites and mutation types.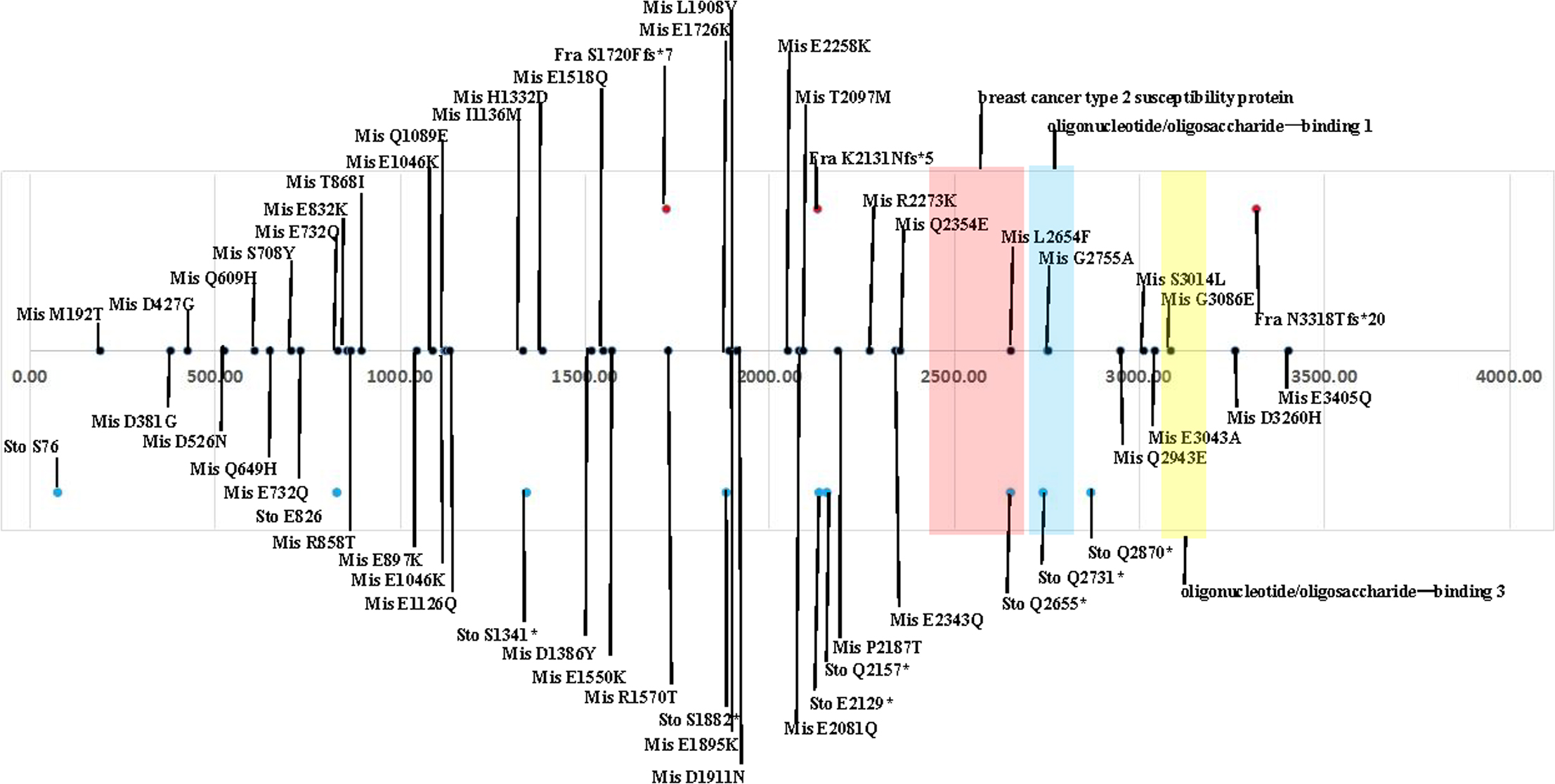
General information
In March 2018 the clinical prognostic data of patients with pathologically confirmed bladder cancer were downloaded from the TCGA website. This included clinical data of 354 bladder cancer patients and their corresponding general information (data without survival time were excluded), which were used for survival analysis. In addition, 412 patients obtained from TCGA were enrolled for genetic diversity analysis as well as gene set enrichment analysis. Inclusion criteria were as follows: (1) age at diagnosis
Statistical analysis
Statistical analyses were performed using SPSS 17.0 software. Measurement data were expressed as (
General information of the enrolled population
General information of the enrolled population
A: Effect of BRCA2 mutation on survival function; B: Effect of BRCA2 expression on survival function.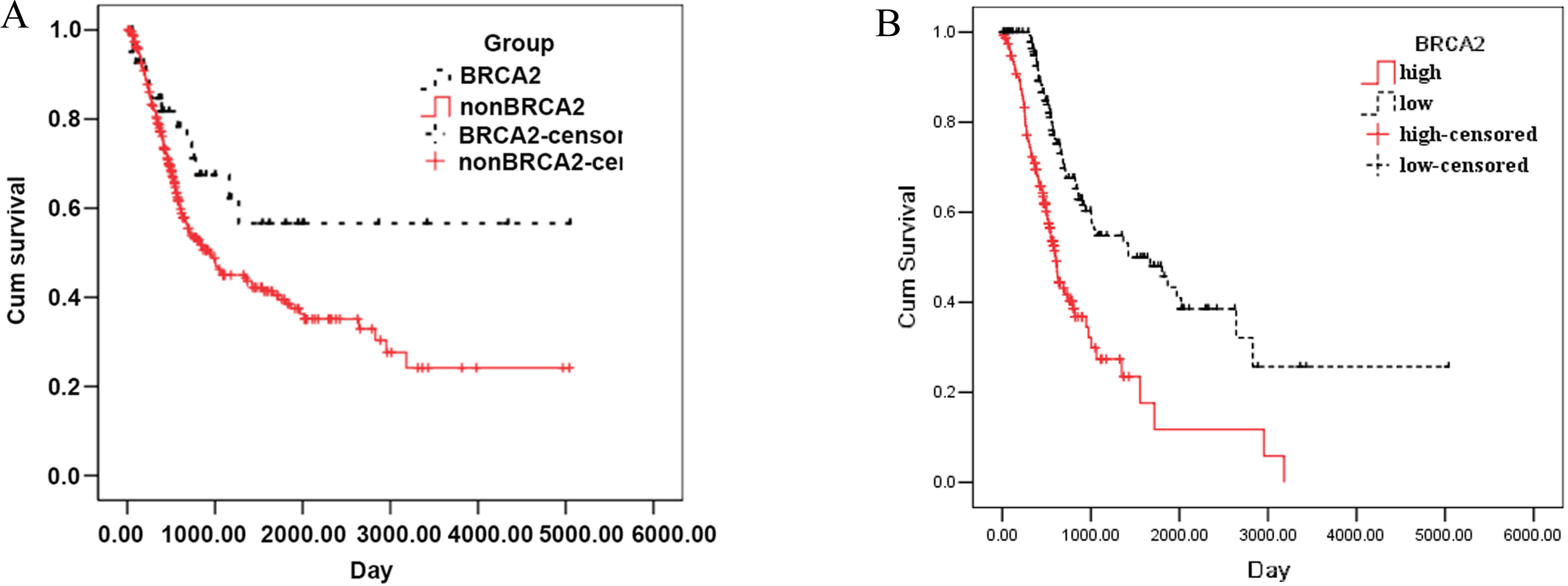
Heat map of genes expression higher in BRCA2 mutation group than BRCA2 non-mutation group.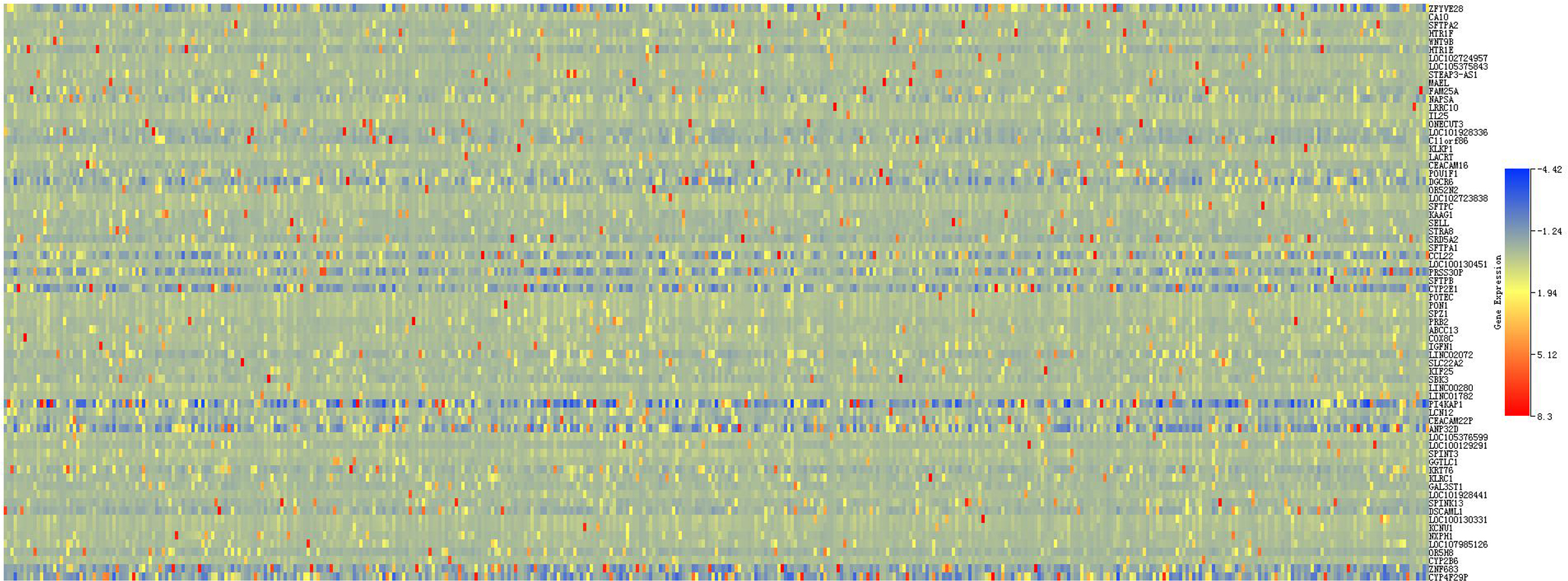
General information
According to the mutation of BRCA2 gene, patients were divided into non-mutation group (
Survival analysis of the BRCA2 mutation group and non-mutation group
The average survival time of 312 patients with non-BRCA2 gene mutation was 1965.594
Survival analysis of the low BRCA2 expression group and high expression group
The average survival time of 156 patients with low BRCA2 gene expression was 2214.902
Known function/phenotype of Protein-protein interaction analysis of differential genes between BRCA2 mutation group and BRCA2 non-mutation group
Known function/phenotype of Protein-protein interaction analysis of differential genes between BRCA2 mutation group and BRCA2 non-mutation group
Heat map of genes expression higher in BRCA2 non-mutation group than BRCA2 mutation group.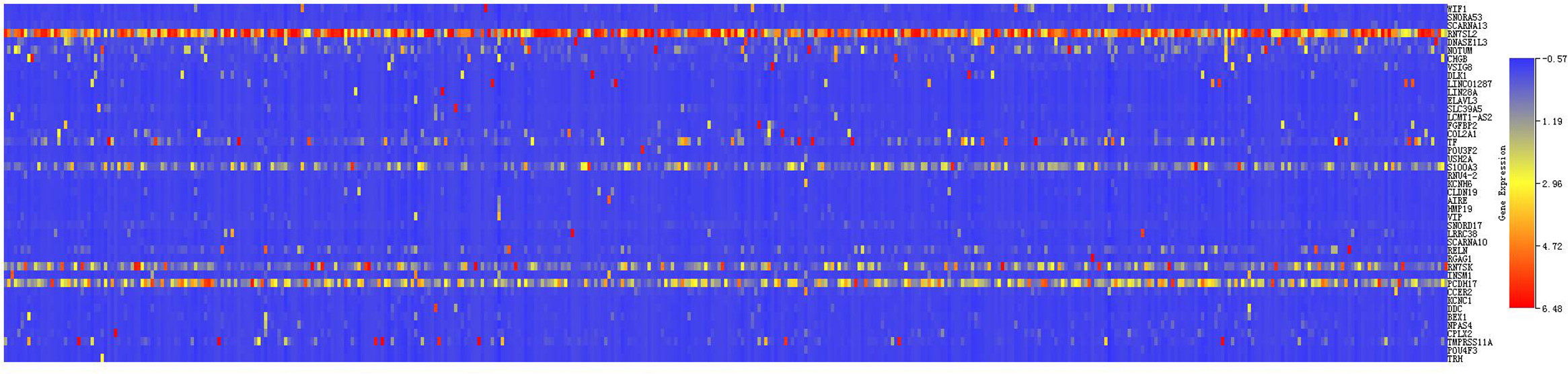
Protein-protein interaction analysis of differential genes between BRCA2 mutation group and BRCA2 non-mutation group.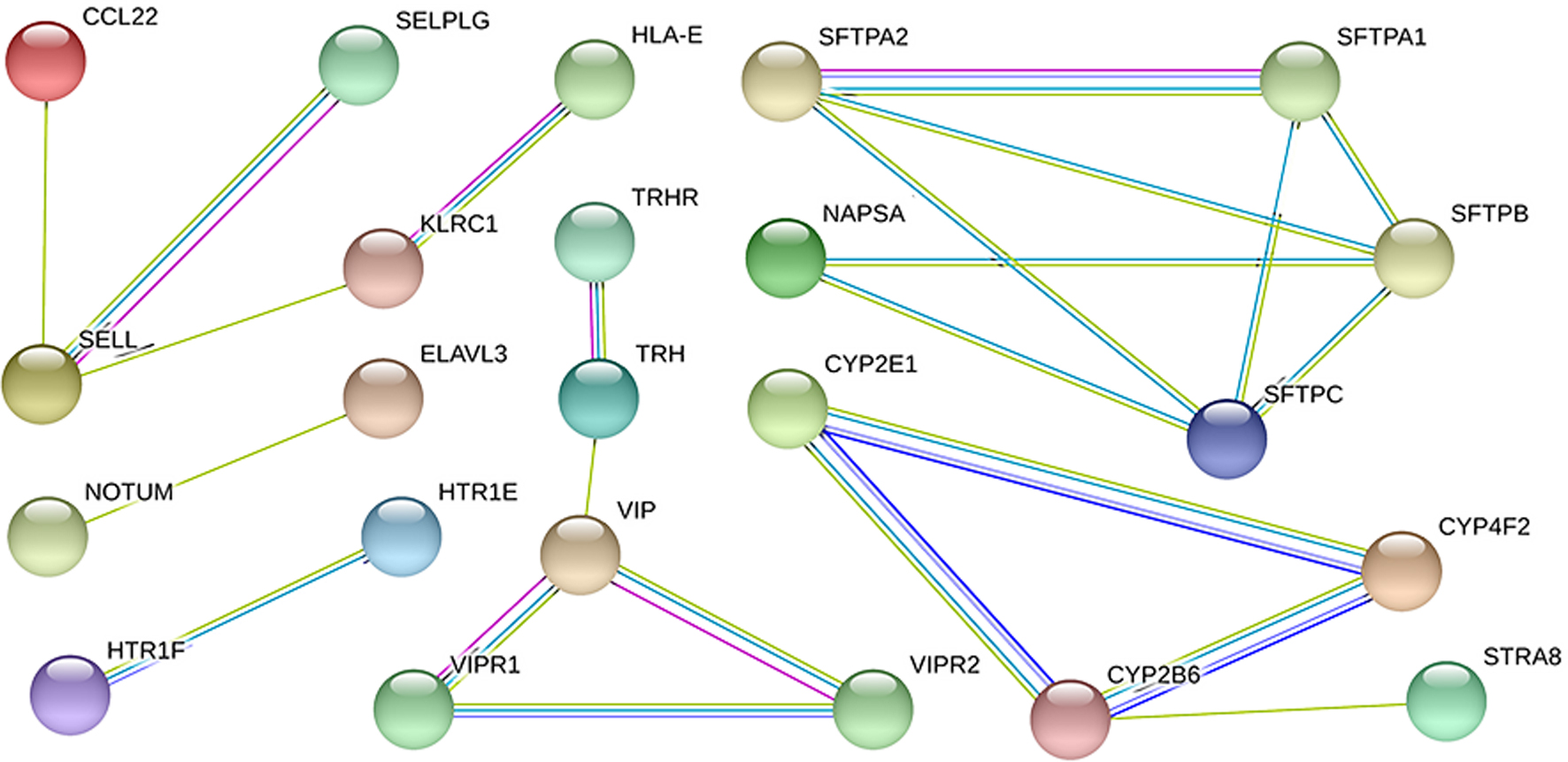
Several Significantly Altered KEGG Pathways in the BRCA2 mutation Patients. A: Cell cycle; B: DNA replication; C: Homologous recombination; D: Oocyte meiosis; E: Ubiquitin-mediated proteolysis; F: Base excision repair; G: Progestin mediated oocyte maturation; H: Basal transcription factor; I: Biosynthesis of N polysaccharide; J: Mismatch repair; K: Spliceosome; L: Purine metabolism; M: P53 signaling pathway; N: Neurotrophic factor signaling pathway.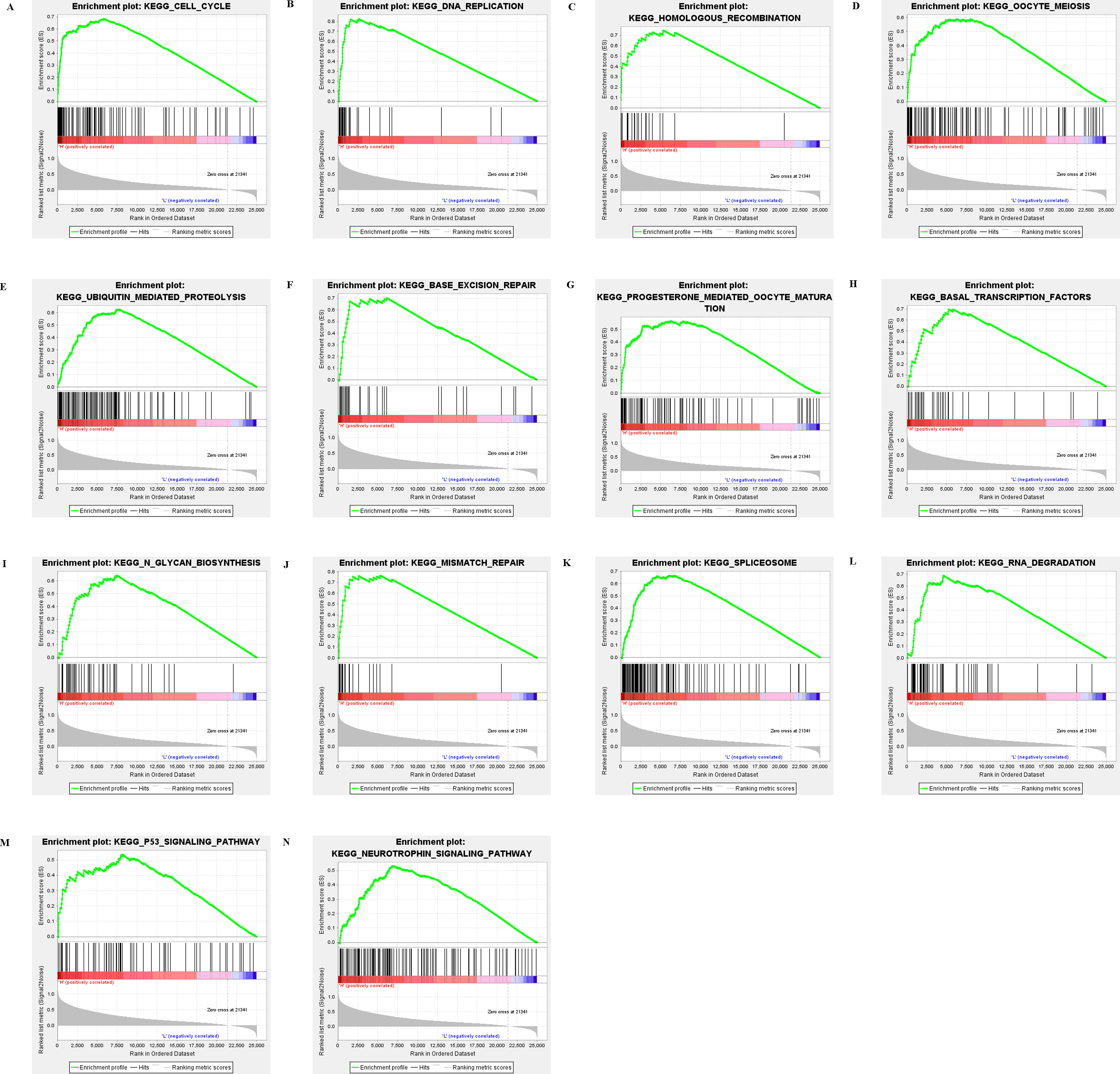
From the grouping of BRCA2 gene mutation and expression of differential genes, a total of 113 genes that were significantly correlated between the two groups were detected (43 genes of positive correlation and 70 genes of negative correlation) (Figs 3 and 4). Subsequently, genes with significant difference in the expression underwent protein interaction network analysis (Fig. 5), where the circles represented genes, and lines represented interaction between genes. The colors of lines represented differential evidence for interaction between proteins, where the red color referred to gene fusion, green color referred to adjacent genes, blue color referred to co-occurrence genes, and black color referred to co-expression genes. These results revealed that among the down-regulated genes, the following genes showed significant interactions: CCL22, CYP2B6, CYP2E1, CYP4F2, HTR1E, HTR1F, KLRC1, NAPSA, SELL, SFTPA1, SFTPA2, SFTPB, SFTPC and STRA8, while among the up-regulated genes, the following genes showed significant interactions: ELAVL3, NOTUM, TRH and VIP. Known function/phenotype of Protein-protein interaction analysis of differential genes between BRCA2 mutation group and BRCA2 non-mutation group see Table 2.
Comparison of functional gene enrichment set between BRCA2 mutation group and BRCA2 non-mutation group
GSEA results prompted that the following gene sets were enriched into the BRCA2 mutation group: cell cycle, DNA replication, homologous recombination, oocyte meiosis, ubiquitin-mediated proteolysis, base excision repair, progestin mediated oocyte maturation, basal transcription factor, biosynthesis of N polysaccharide, mismatch repair, spliceosome, purine metabolism as well as P53, neurotrophic factor signaling pathway, etc. (Fig. 6).
Discussion
Bladder cancer is a tumor caused by multiple factors. A number of genes play an important role in the occurrence and development of the bladder cancer. Recent studies have found that the main mechanisms of bladder carcinogenesis involve overexpression of oncogenes and mutations in the tumor suppressor genes [15]. Past studies revealed E2F3, FGFR3, MMP, HER-2 and erbB-2 played a promoting role in the development of bladder cancer [16, 17, 18, 19], while PTEN, Rb, p53, DMBT1, p27 and other genes played an inhibitory role [20, 21, 22]. The effect of BRCA2 gene mainly lies in repair of DNA and maintenance of gene stability [23]. BRCA2 encodes a protein that consists of 3418 amino acids, including the conservative c region and a bundle of repeated fragments called BRC, while the BRC fragments can regulate the expression of RAD51 gene [9]. For cells without BRCA2 gene, the RAD51 gene cannot be localized in the nuclei, but RAD51 plays an important role in the double-stranded DNA repair. When the double-strand of DNA breaks, the protein with RAD51 expression of increased. RAD 51 is combined with the damaged site of DNA to form RAD 51 nucleoprotein at the DN A3’ to participate in the transfer and replacement between the damaged strand and the homologous sister strand [24]. From the abovementioned BRCA2 gene studies, it was found that the normal expression of the BRCA2 gene was of great significance in the prevention of gene mutation. In the present study, the gene mutation data in patients with bladder cancer was collected from the TCGA, and were divided into BRCA2 mutation group and non-BRCA2 mutation group. Results showed no significant differences in age, sex, pathological staging, clinical staging and degree of differentiation between the two groups. Analysis of survival time demonstrated that the prognosis of the BRCA2 mutation group was better than that of the non-BRCA2 mutation group. Meanwhile, differential analysis revealed the differential genes between the two groups, which included CCL22, CYP2B6, CYP2E1, CYP4F2, HTR1E, HTR1F, KLRC1, NAPSA, SELL, SFTPA1, SFTPA2, SFTPB, SFTPC, STRA8, ELAVL3, NOTUM, TRH and VIP. Literature review found that the genes associated with bladder cancer could be divided into: (1) Cytochrome P450 (CYP) gene: Cytochrome that participates in the phase 1 reaction of drug degradation in liver and in the elimination of many endogenous substances and enzymes by different drugs [25]. (2) 5-hydroxytryptamine receptor genes (HTR1E and HTR1F): Some studies have shown that the gene inhibits the transcriptional activity of the erbB2 promoter and plays a role in the occurrence of the tumor [26]. (3) CCL22 belongs to chemokine family, which is expressed in macrophages, T cells, NK cells and other immunocytes, and plays a role in the monitoring of tumor [27]. We hypothesized that the mutation of BRCA2 may increase the effect of chemotherapeutic drugs, influence cell proliferation and enhance the cell tumor immunity to achieve better survival time, but the specific underlying mechanism needs further discussion.
Yang et al. [28] studied the effect of BRCA2 gene mutation in the prognosis of ovarian cancer, and found that the prognosis of patients in the BRCA2 mutation group was better than that in the non-BRCA2 mutation group. Baert et al. [29] revealed that BRCA2 mutation carriers were more sensitive to radiation. The main reason for this is that during the repair of DNA pathway, BRCA2 mainly plays a role in the S and G2 phases of cell cycle, and patients are most sensitive to radiation during these two periods [30]. Hence, bladder cancer patients with BRCA2 mutation might be more sensitive to radiotherapy, and hence the prognosis of patients with BRCA2 gene mutation was better than that of patients with non-BRCA2 mutation [31]. Due to the defects in BRCA2 gene mutations, the ovarian cancer cells failed to respond to the repair effect of cisplatins, thereby making the ovarian cancer cells more sensitive to chemotherapy [32]. Some cell experiments have also confirmed that the cell strains with BRCA2 gene mutations are more sensitive to chemotherapeutic drugs [33]. P53 gene is a classic tumor suppressor gene, which plays an important role in the cell apoptosis, cell cycle arrest, DNA repair and metabolism [34]. Can p53 gene mutation cause tumor cells to be more sensitive to radiotherapy and chemotherapy? However, few studies have shown that p53 gene mutation does not change the sensitivity of the tumor cells to radiotherapy and chemotherapy compared with BRCA2 gene mutation [31]. A study conducted in 112 patients with BRCA2 mutations demonstrated that 88% of the patients were sensitive to chemotherapy drugs, while only 71% of the patients without BRCA2 mutations were sensitive to chemotherapy drugs [35]. Shao et al. conducted a meta-analysis to study the correlation between BRCA2 mutation and the survival prognosis of breast cancer patients without mutation. The results found that the total survival time of breast cancer patients with BRCA2 mutation was significantly longer than that of the breast cancer patients without BRCA2 mutation, and the difference was statistically significant [36]. However, for patients with prostate cancer, the prognosis of patients with BRCA2 gene mutation was worse than that of the patients without BRCA2 gene mutation. Cui et al. [37] studied the effect of BRCA2 gene mutation on prognosis of 8988 prostate cancer patients, and found that the total survival time of the BRCA2 gene mutation was significantly lower than that of the non-mutatant group. Rytelewski et al. [38] studied the effect of inhibition of BRCA gene expression on the change of ovarian cancer cell metabolism, and found that inhibition of BRCA gene expression could reduce the metabolism of tumor cells, thereby playing a role in tumor growth inhibition. Therefore, the effect of BRCA2 gene mutation on the tumor needs to be rerecognized. The findings of the present study revealed that the BRCA2 gene mutation could improve the prognosis of bladder cancer patients, influencing the cell cycle, DNA replication, homologous recombination, base excision repair, basal transcription factor, mismatch repair, spliceosome, purine metabolism as well as P53 signaling pathway and other gene sets. This might be due to that the BRCA2 gene mutation affected the function of bladder cancer cells to repair the double-strand of DNA, improving the sensitivity to chemotherapy and radiotherapy, and thus improved the prognosis.
Although the bladder cancer patients enrolled in the two groups were comparable in terms of general information, these factors remained significant to influence the prognosis of patients. However, there are some limitations in our study: (1) Chemotherapy and radiotherapy are important factors that affected the prognosis and survival of patients with tumor. However, TCGA database does not record the information about the postoperative chemotherapy and radiotherapy, which in turn affect the accuracy of prognosis. (2) TCGA database does not explain the surgical method and the detection of the specimens by pathologists, which also affects the accuracy of the results. (3) The number of samples included in this study was relatively small, and there are only 42 patients with BRCA2 mutation. Therefore, in order to better verify the results, further studies with larger sample size are needed.
Conclusions
In summary, the present study initially found that the survival time of bladder cancer patients with BRCA2 gene mutation was significantly longer than that of the patients without BRCA2 gene mutation, and the difference was statistically significant. Although previous studies found that BRCA2 gene could inhibit the occurrence and development of cancer, BRCA2 gene mutation could improve the sensitivity of cancer patients to chemotherapy and radiotherapy for patients with breast cancer, ovarian cancer and bladder cancer. This in turn provided a certain value in improving the survival of patients. Therefore, we need to consider the mutation from a new point of view, and deliver a direction for the target therapy of tumors in the future.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest regarding the publication of this paper.