
Abstract
BACKGROUND:
The role of molecular biomarkers in oropharyngeal squamous cell carcinoma (OPSCC) has recently been increasingly recognized. There is conflicting evidence in the literature with regards to the prognostic value of p53 and Bcl-xL.
OBJECTIVE:
The purpose of this study was to investigate the association between p53 and Bcl-xL expression profiles and survival outcomes in OPSCC.
METHODS:
Patients diagnosed with OPSCC and treated with curative intent between 1998 and 2009 were included in the study. Patient demographics, disease, treatment, and oncologic outcomes were collected prospectively. A tissue microarray (TMA) from patients’ biopsies or surgical specimens was retrospectively constructed. The expression levels of p53, Bcl-xL, and p16 were digitally quantified and correlated to patient survival outcomes.
RESULTS:
One hundred and sixty-six patients were included (mean age 56.7 years; standard deviation (SD)
CONCLUSIONS:
This study suggests that biomarker profiling using Bcl-xL and p53 levels may be of prognostic value in select patients with OPSCC.
Introduction
Head and neck cancers remain a major cause of cancer related mortality and morbidity despite significant advancements in treatment modalities. While the incidence of some head and neck cancers has declined in recent decades, the incidence of oropharyngeal squamous cell carcinoma (OPSCC) continues to rise most developed countries [1, 2, 3]. OPSCC clinically categories into two fundamentally distinct cohorts with widely disparate tumor biology, those that are human papillomavirus (HPV) associated and those that caused by alcohol consumption and tobacco use [4, 5, 6]. Traditional risk factors and virally mediated events induce abnormal molecular processes that eventually manifest as malignancies, with oncologic outcomes influenced by known prognostic factors including disease stage, tumor grade and smoking. HPV positivity in OPSCC is strong and independent predictor of improved treatment responses and survival outcomes [7, 8, 9, 10, 11, 12].
OPSCC biomarkers which have received the most significant attention in recent years involve cell cycle regulation and cell signaling pathways. The most important biomarker is p16, a protein that blocks cell cycle progression, which is clinically utilized as a surrogate marker of the HPV-positive disease [13, 14, 15, 16]. Other biomarkers including epidermal growth factor receptor (EGFR), B-cell lymphoma extra-large (Bcl-xL), p53, and Ki67 have been shown to have prognostic significance OPSCC but have received less attention [17, 18, 19]. Bcl-xL is an antiapoptotic protein that has been demonstrated to be associated with survival outcomes in head and neck malignancies with variable results [13, 17, 20, 21]. p53 is a tumor suppressor which was has been associated with poor prognosis in some studies but not in others [22, 23, 24, 25].
While it is generally agreed on that p16 predicts prognosis in patients with OPSCC, it remains unclear in the literature whether other biomarkers may be utilized in combination to more accurately and reliably identify those most at risk of disease recurrence. The aim of this study was to review a large cohort of patients with curable oropharyngeal squamous cell carcinomas to determine whether p53 and Bcl-xL may predict nodal disease at presentation and survival outcomes as single markers and as combined markers. This may help identify high risk patients who are likely to develop subsequent recurrences and who may benefit from more extensive treatment regimen, and/or more aggressive surveillance for the assessment of disease relapse.
Patients and methods
Patient cohort
Institutional Research Ethics Board approval from the University of Alberta Health Research Ethics Board was obtained for this study (Pro00016426). All patients diagnosed with OPSCC at the University of Alberta Hospital between January 1
A retrospective chart and pathology review was performed to collect relevant patient information from the Alberta Cancer Registry (ACR). Information related to patient demographics, disease, treatment, and oncological outcomes were collected. Patients were stratified by smoking status and p16 status. Patients were classified as smokers if they had a tobacco use history
Tissue microarrays
Tissue microarrays (TMAs) were constructed from either pre-treatment biopsies or primary surgical specimens, as recently described [18, 27, 28]. Formalin-fixed paraffin-embedded (FFPE) tumor tissue blocks were retrieved for TMA construction. Hematoxylin and eosin-stained (H&E) slides were obtained from surgical specimens and reviewed by a Head and Neck pathologist (L.P.) to confirm the diagnosis of OPSCC. Each TMA was assembled from duplicate or triplicate 0.6 mm cores randomly sampled from the tumor-containing area of each FFPE block. Cases with inadequate tissue and/or tumor were excluded from the analysis, however excluded cases were not deemed to be significantly different from the remaining cohort as previously reported [7]. Five TMAs were constructed with duplicate cores of FFPE blocks, per the TMA protocol previously described [7]. Five negative controls were incorporated on the arrays using FFPE tissue blocks from placenta, kidney, pancreas, liver, and HPV-negative tonsils. Three HPV-positive control tissue from HPV-infected cervical intraepithelial neoplasia were included for reference intensity staining determined by HPV16/18 by in situ hybridization and p16 positivity detected by chromogenic IHC staining by 2 pathologists.
Patient flowchart.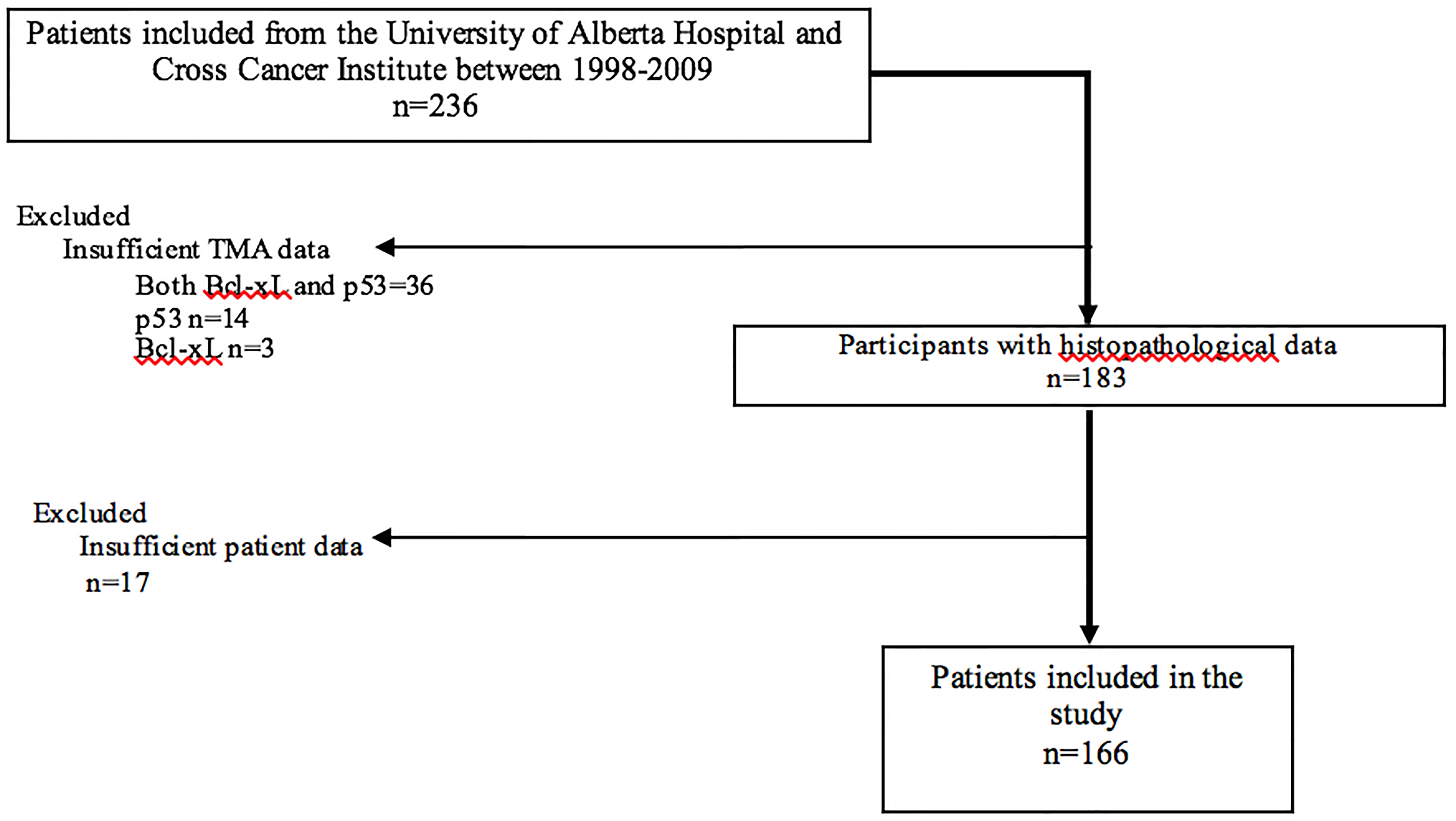
Each TMA was deparaffinized in xylene, rinsed in ethanol, and rehydrated with water. Heat-induced epitope retrieval for Bcl-xL was achieved by heating slides to 121 degrees Celcius in an EDTA-containing Target Retrival Solution (pH 9.0) (DAKO) for 3 minutes, and each slide was stained for Bcl-xL using rabbit monoclonal anti-Bcl-xL (1:500 dilution, Cell Signalling). Rabbit Envision
Histological examination of the tumor tissues was done by one experienced head and neck pathologists (L.P.) who were blinded to the clinicopathological data and oncologic outcomes of the patients. Each TMA was scanned by HistoRxTM PM-2000 and analyzed using AQUAnalysis
For Bcl-xL and p53 expression, values that were above the median value calculated for the entire cohort of 166 specimens were deemed positive. For p16, cores that expressed
Statistical analysis
Statistical analyses were performed using SPSS (version 21.0 SPSS Inc., Chicago, IL, USA) and Microsoft Excel. All p-values were two-tailed and a
The independent data were compared using
Characteristics of oropharyngeal cancer patients included in this study, comparing all patients to those with high or low Bcl-xL and p53 levels
Characteristics of oropharyngeal cancer patients included in this study, comparing all patients to those with high or low Bcl-xL and p53 levels
*Denotes statistical significance.
Kaplan-Meier Survival Curves for OPSCC stratified by p16 and smoking status.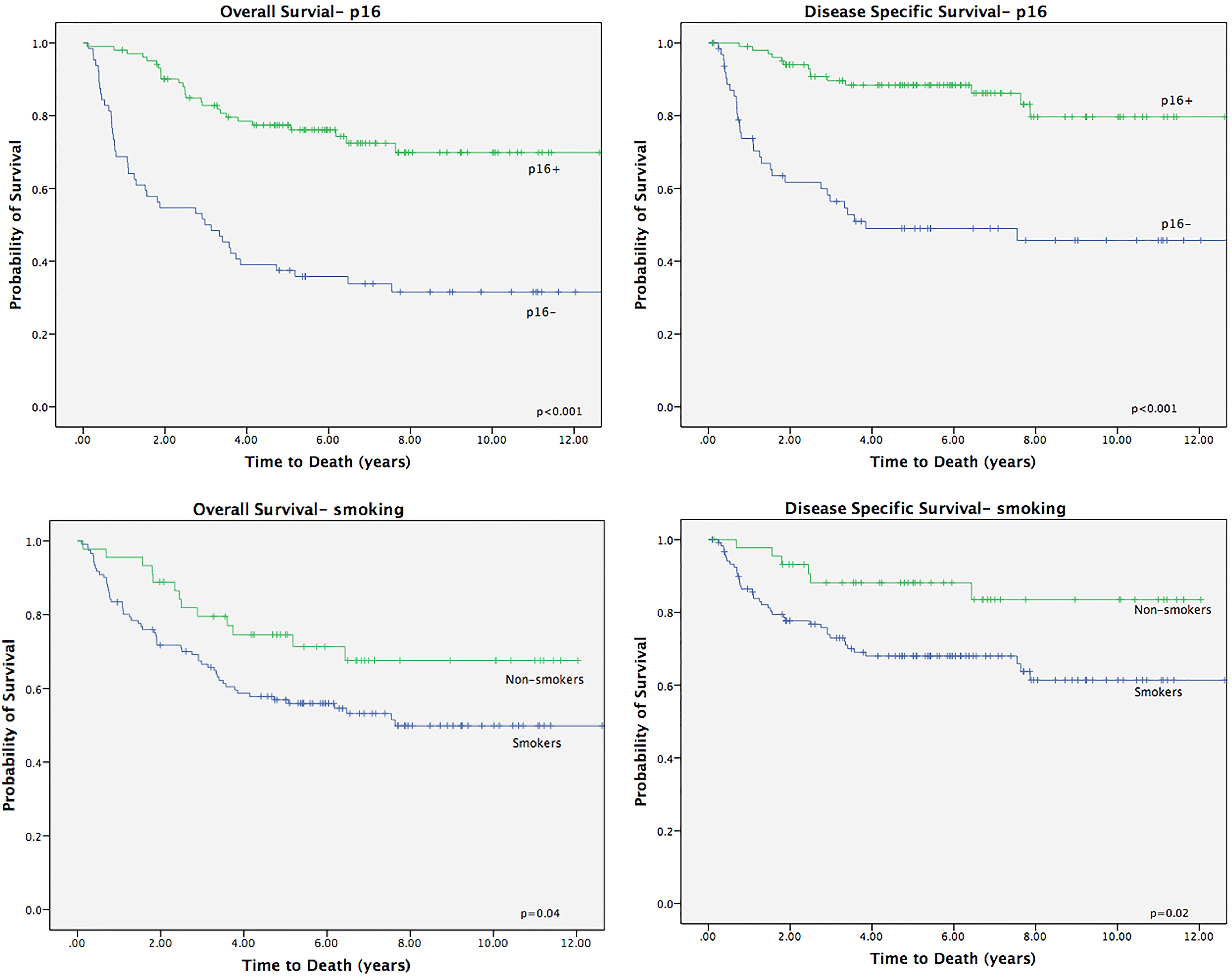
Kaplan-Meier Survival Curves for Bcl-xL expression in OPSCC (stratified by smoking status).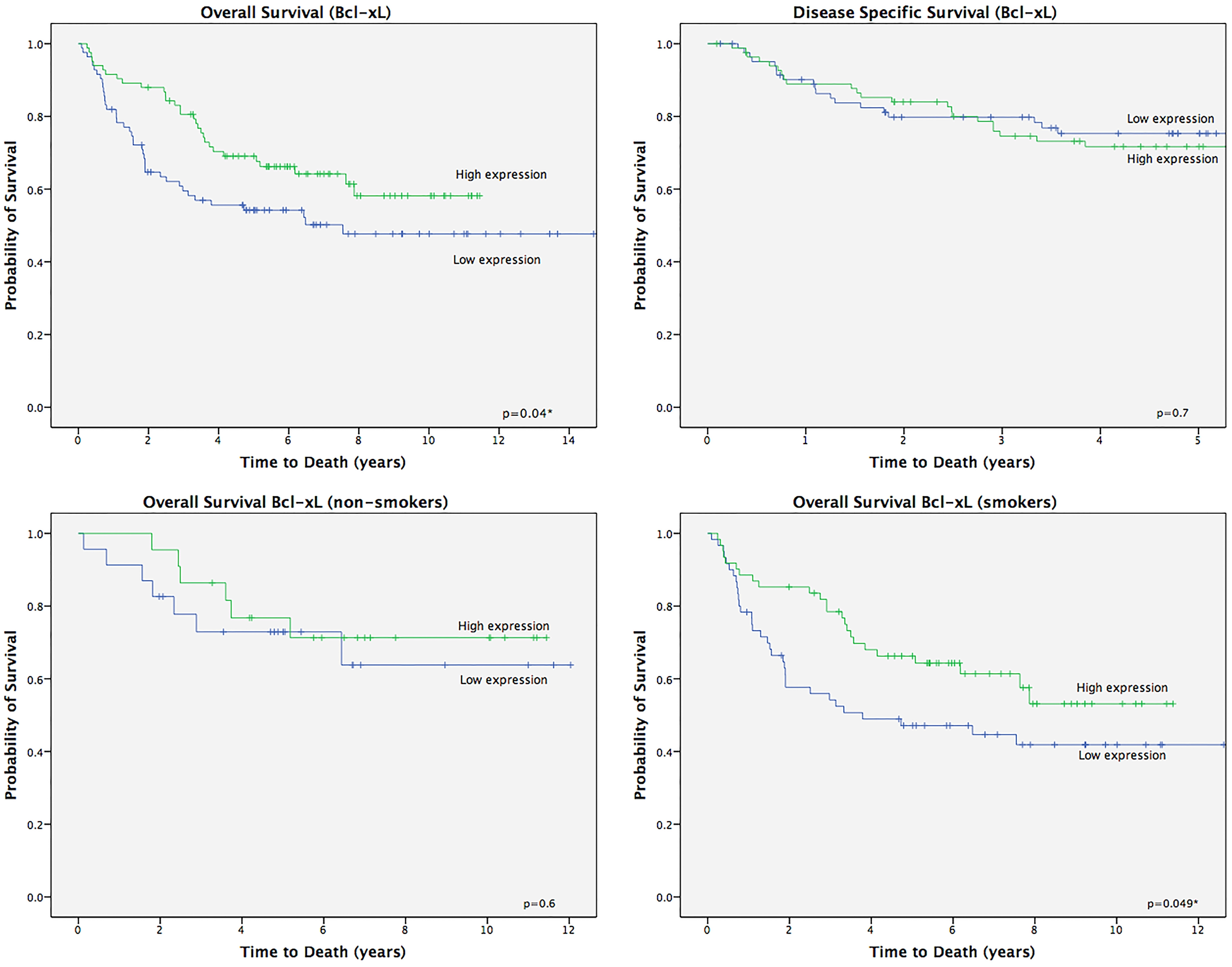
Chi-squared analysis of p53 and Bcl-xL with nodal disease at presentation and development of distant metastases in OPSCC patients treated with all modalities
*Denotes statistical significance.
Kaplan-Meier analysis of biomarker expression and 5-year survival outcomes in OPSCC patients
*Denotes statistical significance.
One hundred and sixty-six patients were included in our study with sufficient tumor tissue available for generation of Histoplat analysis (Fig. 1). Table 1 describes relevant demographic and clinical variables. The mean age of the patients was 56.7 years (SD
Cox regression analysis of biomarker expression with overall survival
Cox regression analysis of biomarker expression with overall survival
*Denotes statistical significance.
Kaplan-Meier Survival Curves for p53 expression in OPSCC (stratified by smoking status).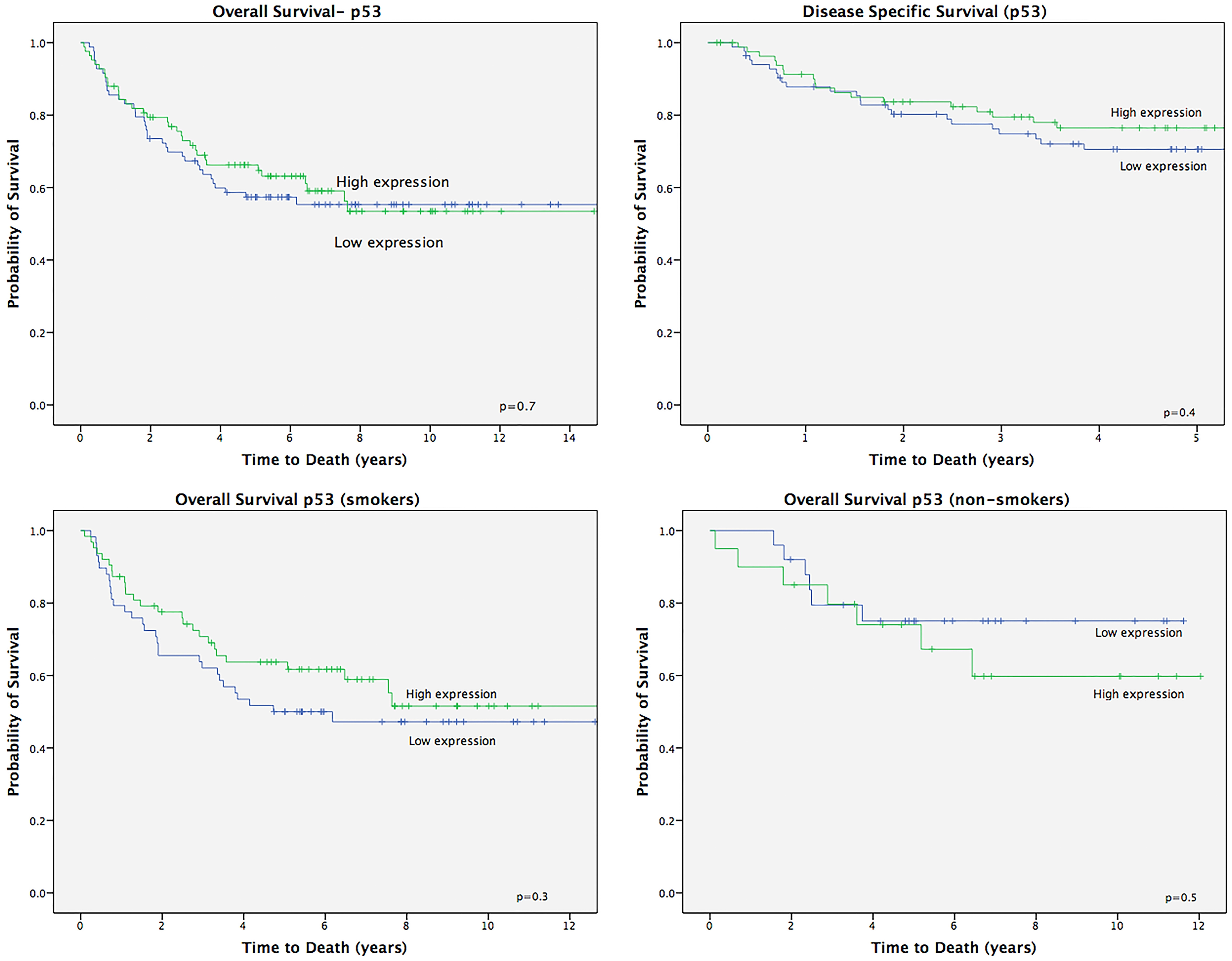
Kaplan-Meier Survival Curves for combined Bcl-xL and p53 expression in oropharyngeal squamous cell carcinoma. Survival curves are shown for A) all OPSCC included, B) stratified according to smoking status and C) stratified by p16 status.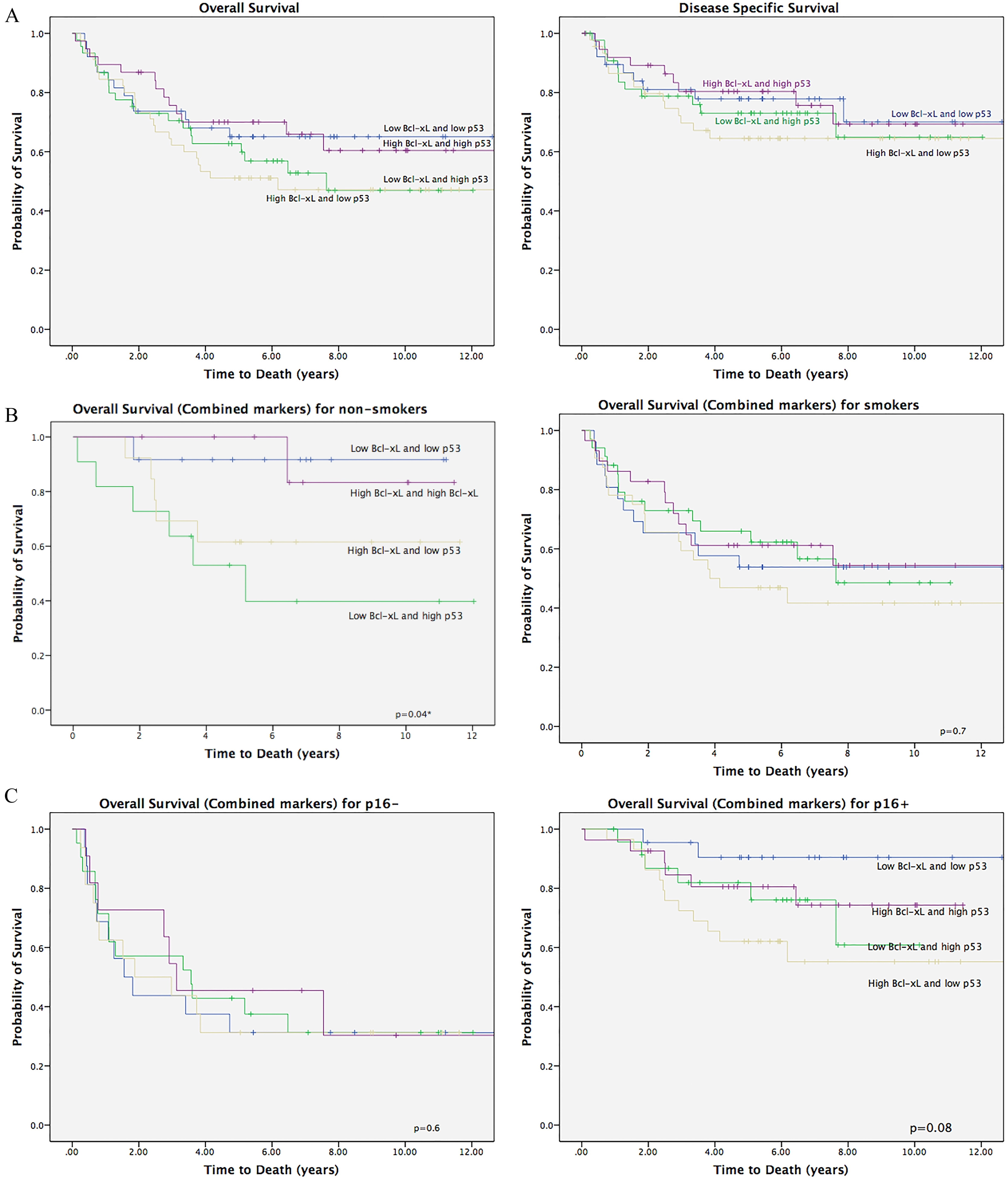
The median follow-up time was 5.22 (SD
p16 positivity was confirmed in 102 patients (61%). High p16 expression was not associated with nodal disease at presentation (
Of the 219 specimens with TMA data, 166 had data on both Bcl-xL and p53 biomarkers. Chi-squared analyses demonstrating the relationship between biomarker expression and nodal disease at presentation are demonstrated in Table 2.
High Bcl-xL expression was associated with positive nodal disease at presentation (
Cox regression analysis of biomarker levels with overall survival when compared to known prognosticators for overall survival
*Denotes statistical significance.
There was no statistically significant association between p53 expression and nodal disease at presentation (
Chi-squared analyses revealed no significant association between the combined expressions of Bcl-xL and p53 biomarkers with nodal disease at presentation (
Kaplan-Meier Analysis for OS for high Bcl-xL/high p53 and low Bcl-xL/low p53 vs. high Bcl-xL/low p53 and low Bcl-xL/high p53.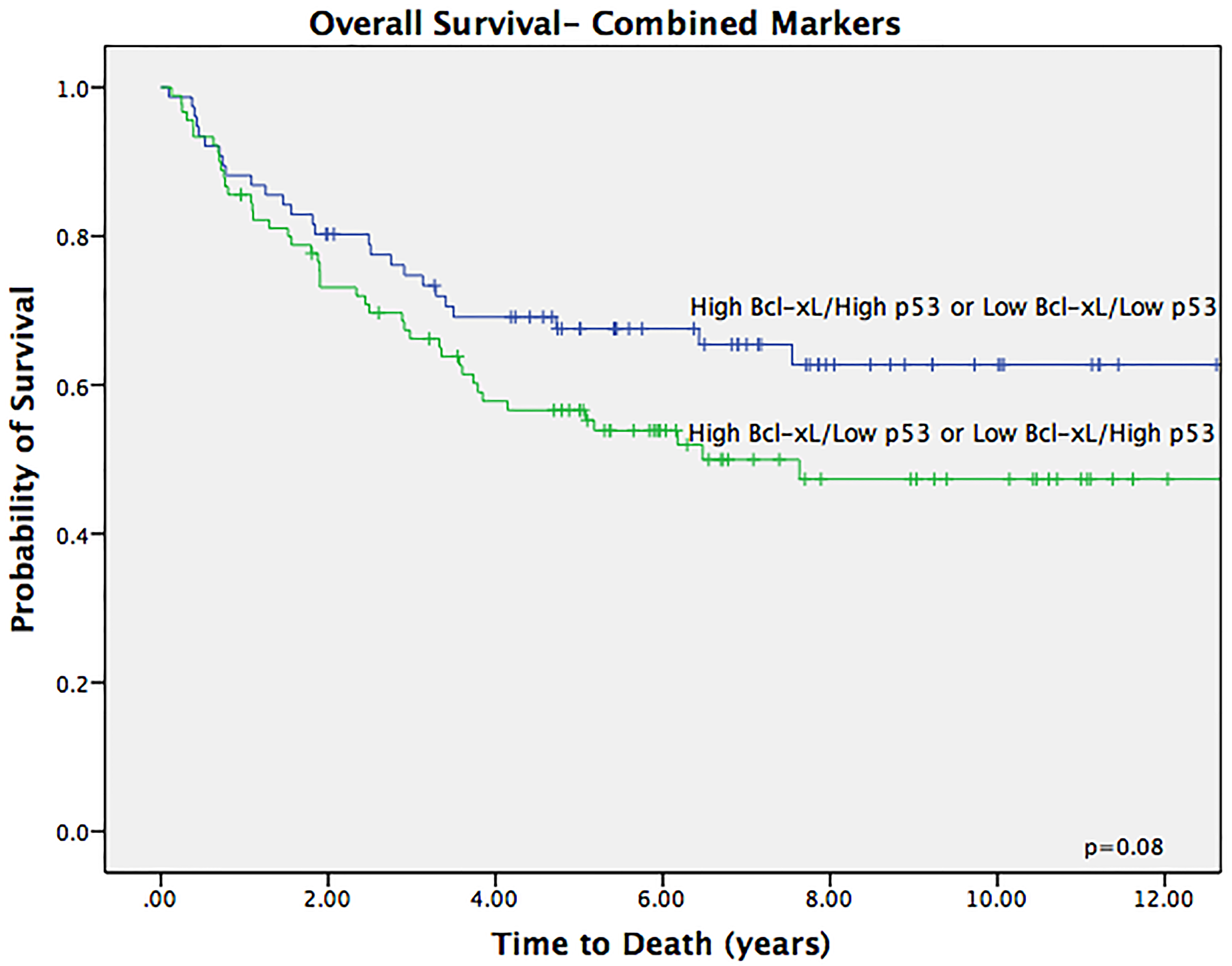
Although not statistically significant, the Kaplan-Meier analyses showed trends towards improved OS for patients with high Bcl-xL expression and high p53 expression, and those with low Bcl-xL and low p53 expression compared to those with high Bcl-xL and low p53 expression, or those with low Bcl-xL expression and high p53 expression (Fig. 5A). The trend became more apparent when stratified by p16 status, and smoking. There was a significant overall survival benefit of combined markers in non-smokers (Fig. 5B). This trend became more apparent in patients with p16 positive SCC (Fig. 5C). Patients with p16 positive disease with low Bxl-xL expression and low p53 expression had higher overall survival compared to the other different combinations (Fig. 6).
In the present study, we observed that in patients with OPSCC, combined Bcl-xL and p53 expression had a survival benefit in a select population of non-smokers with p16 positive disease. Bcl-xL expression was independently associated with nodal disease at presentation and poor overall survival. Consistent with other studies, p16 and non-smoking status were associated with nodal disease at presentation and favourable survival outcomes [6]. Our study was successful in identifying patients at risk of more advanced disease and poor oncologic control. Bcl-xL and p53 may serve as biomarkers of aggressive disease, which could be of clinical utility in identifying patients who may benefit from more intensive treatment regimens.
The role of biomarkers in the workup and surveillance of head and neck cancers remains unclear in the literature. This is due, in part, to varied methods of biomarker staining and quantification [13, 17, 23, 31, 32]. Various antibodies have been used to identify the same biomarker, with variable interpretation of expression levels that does not account for differences in nuclear and cytoplasmic staining. Some studies use the median value of the biomarkers to differentiate between high and low biomarker expression, while others quantify both the intensity and prevalence score to determine biomarker status. These differences, in addition to patient heterogeneity, may have concealed a survival advantage in those with low expression of biomarkers Bcl-xL and/or p53. This variability could be overcome using tissue microarrays and automated immunohistochemistry stains. Tissue microarrays method helps ensure objective quantitative immunohistochemical techniques such as the AQUAnalysis
When comparing with the literature, our results corroborate the established finding that p16 and smoking status hold prognostic value for overall survival and disease specific survival in OPSCC [17, 18, 26]. The prognostic value of the expression of Bcl-xL and p53 however are more ambiguous with some discrepant conclusions in the literature. Bcl-xL is an anti-apoptotic protein in the Bcl-2 family that has recently captured interest in the literature as a prognostic marker in head and neck cancer recurrence, and with treatment response [13, 25, 36, 37, 38]. With respect to oropharyngeal cancers specifically, our group previously reported a lack of association between Bcl-xL and disease recurrence; similar results were shown in a study by Michaud and colleagues in which Bcl-xL was not associated with risk of recurrence [18, 38]. However, our group previously demonstrated an independent association of Bcl-xL with nodal disease at presentation independent of p16. This was confirmed again in this present study, suggesting a dichotomous pathway for nodal spread wherein Bcl-xL is associated with the carcinogenically (and p53-) associated OPSCC.
p53 is a key regular of apoptosis and cell cycle progression, and has been implicated in more than half of head and neck cancers [39]. Traditionally, p53 expression has been associated with SCC and characterized by heavy use of tobacco and alcohol, and not with HPV associated malignancies [40, 41, 42]. p53 expression has also been shown to predict locoregional failure in the head and neck [43, 44, 45]. Rasmussen and colleagues found that high expression of p53 is associated with reduced risk of distant metastasis, but increased risk of locoregional failure [40]. However, this study cohort was heterogeneous in baseline patient characteristics between the two groups of patients, specifically with respect to p16 status.
The molecular pathways affecting disease spread are complex, with variability in the literature on whether a combined biomarker analysis could be used as a significant prognosticator. Kumar and colleagues suggested that the prognostic value for p53 was dependent on Bcl-xL expression status. They showed that the combination of high Bcl-xL expression with low p53 expression was associated with poor survival (overall- and and recurrence free-), and Bcl-xL expression alone was not associated with survival outcomes or treatment response. Similar associations were found with the effect of the combined biomarker expression on chemotherapy resistance in vitro [46]. Low Bcl-xL expression was most useful in patients with absent or low p53 expression [20]. This survival benefit was also demonstrated in our study wherein patients with low p53 with low Bcl-xL had trends towards improved survival compared to their counterparts with high p53 with low Bcl-xL expression.
In this cohort, Bcl-xL and p53 together trended towards patterns of outcome and survival, dependent on HPV and smoking status. This trend was statistically significant in patients who were non-smokers, or those with p16 positive disease. Similar patterns of survival were demonstrated in a study by Kumar and colleagues [17] demonstrating improved disease specific survival outcomes in patients with low p53/Bcl-xL, followed high p53/high Bcl-xL compared to those with high Bcl-xL/low p53 or low p53/high Bcl-xL. Patients low Bcl-xL and p53 had improved survival.
Determining the interrelated roles of multiple biomarkers will be necessary to further understand the mechanisms at play in regional disease and disease recurrence. When p53 function is impaired, Bcl-xL may cooperate in producing a p53 dependent cell cycle arrest [47]. These results in addition to our findings suggest a dichotomous pathway for nodal spread wherein Bcl-xL is associated with the carcinogenically non virally-mediated SCC, and p53-associated. Favourable outcomes of patients whose tumors have low p53 and low Bcl-xL may likely be secondary to p53-mediated apoptosis secondary to treatment-induced damage as observed in vitro [46].
Results of this study have limitations that affect its interpretation. It is a retrospective study susceptible to biases of such designs. This study involved both HPV positive and HPV negative oropharyngeal SCCs, both with unique biologic behaviors. Although we used p16 as a surrogate for viral induced SCC, stratifying by this and smoking status does limit the overall power of our study. Furthermore, our study groups were managed heterogeneously including combinations of both surgical and non-surgical treatments.
Conclusions
The present study is the largest study to ascertain the significance of combined Bcl-xL and p53 expression in patients with OPSCC. This study supports previous findings that high expression of Bcl-xL is associated with nodal disease at presentation and confer a survival disadvantage. Combined low Bcl-xL and p53 levels may also be associated with a survival benefit. The current study should serve as a basis for future studies that may prospectively enroll a larger number of patients to yield more robust survival estimates.
Footnotes
Acknowledgments
Funding was received from the University of Alberta Hospital Foundation and Alberta Head and Neck Centre for Oncology and Reconstruction Fund. We wish to thank Michelle Dean and Alex Klimowicz at the University of Calgary Tissue Imaging Unit for their assistance with tissue microarray construction.
Conflict of interest
The authors declare that they have no financial or other conflicts of interest in relation to this research and its publication.
Supplementary data
The supplementary files are available to download from