
Abstract
Background/Aim:
Lymph node density is a parameter used to more accurately predict tumor recurrence and patient survival. However, its association with surgical outcome in pyriform sinus carcinoma remains unclear. The purpose of this study was to assess the prognostic value of lymph node density in advanced pyriform sinus carcinoma.
Patients and Methods:
A total of 87 patients with pyriform sinus carcinoma treated between 2008 and 2015 were enrolled. Then, 5-year overall survival, 5-year disease-specific survival, 5-year disease-free survival, and 5-year regional recurrence-free survival were utilized to assess the prognostic significance of lymph node density.
Results:
With a median follow-up period of 31.8 months, 5-year overall survival, disease-specific survival, disease-free survival, and regional recurrence-free survival were 37.9%, 46.0%, 41.4%, and 54.0%, respectively. Univariate analysis revealed that lymph node density ≥ 0.093 was a significant predictor of poor 5-year overall survival (P = .005), disease-specific survival (P = .008), disease-free survival (P = .0013), and regional recurrence-free survival (P = .003). Furthermore, multivariate analysis demonstrated that lymph node density was negatively associated with adverse 5-year overall survival (hazard ratio = 1.62, 95% CI: 1.15-2.29, P = .006), disease-specific survival (hazard ratio = 1.86, 95% CI: 1.24-2.80, P = .003), disease-free survival (hazard ratio = 0.45, 95% CI: 0.24-0.85, P = .014), and regional recurrence-free survival (hazard ratio = 2.97, 95% CI: 1.43-6.17, P = .004).
Conclusion:
Taken together, these results reveal that lymph node density is a powerful prognostic factor for patients with T3 and T4 pyriform sinus carcinoma, and the median lymph node density cutoff values ≥ 0.093 are associated with a greater risk of recurrence and poorer survival.
Introduction
In North America, pyriform sinus carcinoma (PSC) accounts for 65% to 85% of all hypopharyngeal squamous cell carcinomas (HPSCCs), 1 with approximately 70% to 85% of cases presenting with cervical lymph node metastasis (LNM) in stage III or IV 2 ; even more than 50% early stage cases (T1-T2) show occult nodal metastases. 3 Lymph node metastasis, one of the most important tumor features, has been used as a significant prognostic factor in head and neck cancers, 4 suggesting that the lymph node status may be a key indicator for predicting recurrence and survival in HPSCC.
Lymph node density, or lymph node ratio, is considered a potential prognostic factor after surgery in patients with prostate, pancreatic, gastric, and esophageal malignancies. 5 -8 Indeed, LND is more advantageous than the tumor-node-metastasis (TNM) classification system nodal staging system in predicting disease-specific survival (DSS), 9 recurrence-free survival, and overall survival (OS). 10 Likewise, in the head and neck region, LND also plays a predictive role for patients with oral cavity, thyroid, and laryngeal cancers. 11 -13 All the aforementioned studies have revealed that LND is a significant factor and an independent predictor of tumor recurrence and survival. In addition, in a few retrospective studies of patients with HPSCC, LND could help otolaryngologists or oncologists devise more optimized postoperative treatment modalities. 14 -16
Anatomically, the hypopharynx consists of 3 subsites: the pyriform sinus, posterior pharyngeal wall, and post-cricoid area. In HPSCC, LNM route and frequency vary depending on the anatomy of the subsite. Pyriform sinus carcinoma prefers level III and IV cervical nodes, while cancers of the posterior pharyngeal wall are more likely to metastasize to retropharyngeal lymph nodes. 17 Meanwhile, post-cricoid tumors spread most often to level III and IV nodes. The different metastatic routes of nodes could cause different node yields and metastatic involvements, both of which significantly affect the accuracy of LND. Therefore, analyses based on the hypopharyngeal subsite would decrease the interference of confounding factors and provide a more accurate cutoff value for LND.
To the best of our knowledge, no study has assessed the prognostic value of LND in patients with HPSCC with pyriform sinus cancer. The aim of this study was to evaluate the prognostic significance of LND for 5-year OS, DSS, disease-free survival (DFS), and regional recurrence free survival (RRFS) and determine clinicopathologic prognostic factors in patients with T3 and T4 PSC.
Materials and Methods
Study Design and Patient Selection
Patients with HPSCC who met the following criteria were enrolled: (1) clinical resectable T3 or T4 hypopharyngeal carcinoma in the pyriform sinus [based on the 2010 American Joint Committee on Cancer (AJCC) TNM staging system]; (2) curative treatment with primary surgery between January 1, 2008, and December 31, 2015; (3) biopsy-evidence of squamous cell carcinoma (SCC); (4) no distant metastases at presentation; (5) not radiotherapy, chemotherapy, or other treatments before surgery. Patients with incomplete data for evaluating the lymph nodal status, a history of neck dissection in other hospitals, or second neck dissection for tumor relapse were excluded. The clinical charts of patients with HPSCC treated in the Department of Otolaryngology and Head and Neck Surgery, Southwest Hospital, Army Medical University (Third Military Medical University) were assessed. A total of 87 patients newly diagnosed with T3 or T4 HPSCC in the pyriform sinus were included. Medical records were reviewed and related data were retrieved, including clinicopathologic characteristics, surgical therapy, follow-up, and surgical outcomes. Follow-up after treatment was performed every 1 to 3 months during the first year, every 3 to 6 months in the subsequent 2 years, and annually thereafter. Survival patients who did not show up at the scheduled check-up were reminded by phone.
Histopathologic examination of primary tumor and neck dissection samples was performed by an experienced head and neck pathologist according to the guidelines for the examination and reporting of head and neck cancer specimens (Ver. 3.0, 2010). Lymph node density was defined as the number of metastatic cervical lymph nodes divided by the total number of lymph nodes excised. Outcome variables included 5-year OS, DSS, DFS, and RRFS. Overall survival was defined as the time from the day of surgery to death from any cause. Disease-free survival was defined as the time from surgery to first relapse or death from any cause. Disease-specific survival was defined as the interval from surgical treatment to death from HPSCC or treatment toxicity. Regional recurrence-free survival was defined as the period from the day of surgery to the time of relapse in the regional nodes according to clinical and/or radiographic evidence.
Statistical Analysis
All statistical analyses were performed with the SPSS ver. 24.0 software package (IBM Corporation). Numeric data are mean ± standard deviation. The cutoff value for LND in patients with HPSCC with or without tumor recurrence was calculated using a time-dependent receiver operating characteristic (ROC) curve. The χ2 test was used to assess categorical variables, and survival analyses were performed by the Kaplan–Meier method and log-rank test. Multivariate survival analysis was performed using a Cox proportional hazard model. Hazard ratios (HRs) and 95% CIs were calculated to determine the effects of putative HSC variables on study outcomes. P < .05 was considered statistically significant.
Results
Patient Characteristics
Of all 236 hypopharyngeal cancer cases reviewed, 166 (70.3%) were newly diagnosed with stage T3 or T4 disease. A total of 79 patients were excluded for non-PSC, nonsurgical therapy, no neck dissection, non-SCC, distant metastasis, and/or incomplete clinical data or follow-up. Finally, 87 patients with stage T3 and T4 HPSCC in the pyriform sinus were included based on the abovementioned eligibility criteria. Postoperative follow-up was until December 2016. The median postoperative follow-up period for survivors who underwent surgery was 31.8 months (range, 2-120 months).
The 87 eligible patients included 82 men and 5 women, aged 58.77 ± 6.86 years (ranging from 43 to 75 years). Their demographic and clinicopathologic characteristics are presented in Table 1. As for tumor cell differentiation status, there were 13, 49, 17, and 8 well differentiated, moderately differentiated, poorly differentiated, and unknown cases, respectively. T3 and T4 disease stages were found in 51 and 36 cases, respectively; pN stage distribution was 9 for N0, 32 for N1, 4 for N2a, 16 for N2b, 18 for N2c, and 8 for N3.
Demographic Profiles of Patients With T3 and T4 Pyriform Sinus Carcinoma (n = 87).
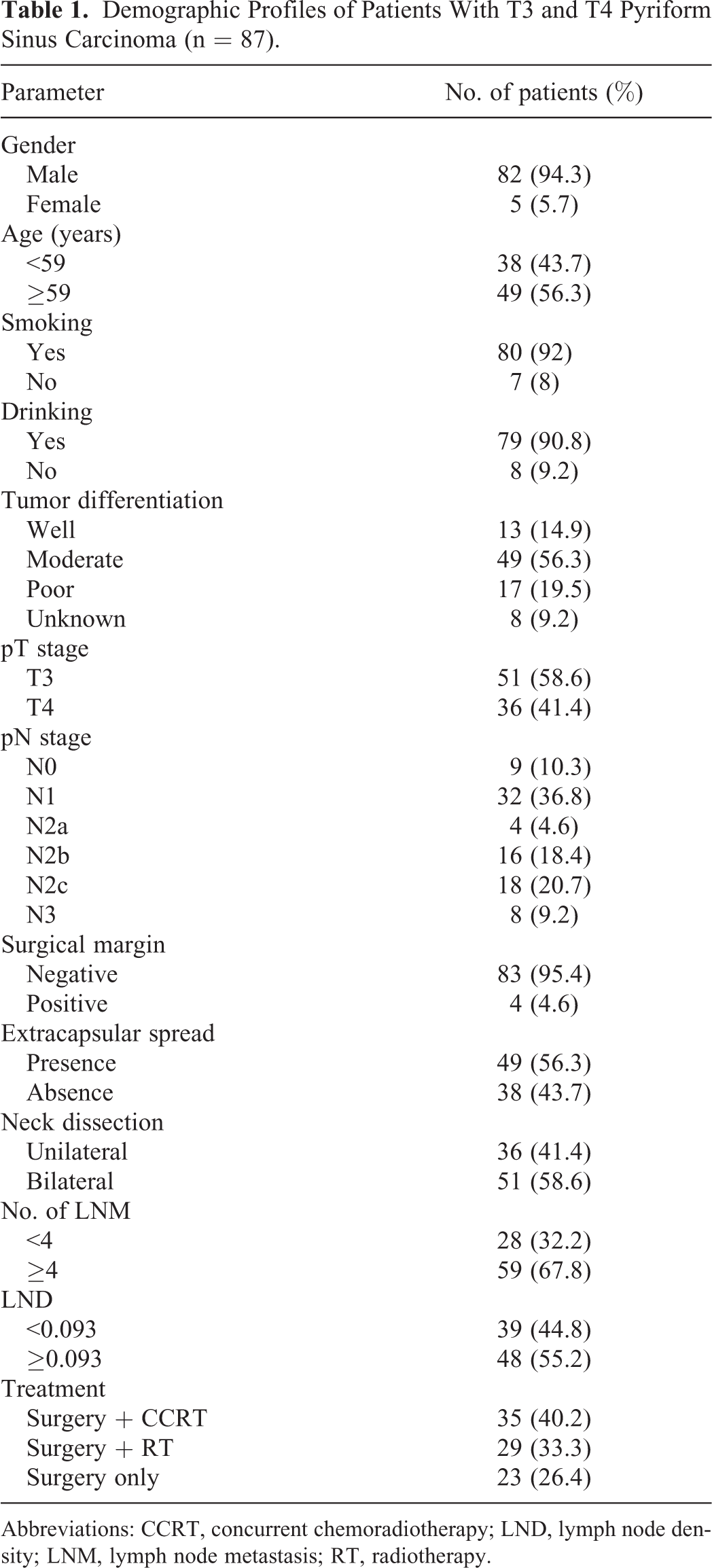
Abbreviations: CCRT, concurrent chemoradiotherapy; LND, lymph node density; LNM, lymph node metastasis; RT, radiotherapy.
Nodal Status and LND Cutoff Value
Of the 87 patients who underwent primary surgery with neck dissection, 36 (41.4%) received unilateral neck dissection and 51 (58.6%) underwent bilateral neck dissection; therefore, there were 138 (36 plus 102) sides of the neck to be included. A total of 3481 lymph nodes were examined, and 339 (9.74%) were positive. The median number of lymph nodes after lymph node dissection was 40.5 (range, 0-75), for a median number of metastatic lymph nodes of 3.91 (range, 0-28). In the study cohort, < 4 LNM (positive lymph nodes) in 28 (32.2%) patients, with ≥ 4 in 59 (67.8%) patients (Table 1).
The median LND was 0.123 ± 0.174 for all patients, and LND distribution among the patients with pathologic neck examination according to the (pN) classification is shown in Figure 1: 9 (10.3%) patients with pN0, 32 (36.8%) patients with pN1, 46 (52.9%) patients with pN2/3, respectively. Without the patients with N0, an LND value of 0.093 was defined as the optimal cutoff point based on the Youden index (Table S1) in time-dependent ROC curve analysis for 5-year OS; an area under the curve of 0.818 ± 0.047 (P < .0001) was obtained, with sensitivity and specificity of 60.8% and 92.6%, respectively (Figure 2A and B).
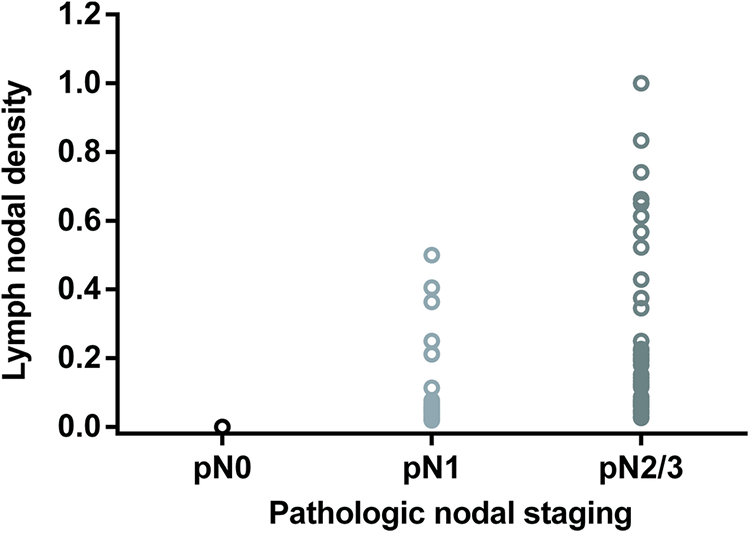
Lymph node density is significantly different among the 3 histopathologic nodal stages (P < .001).
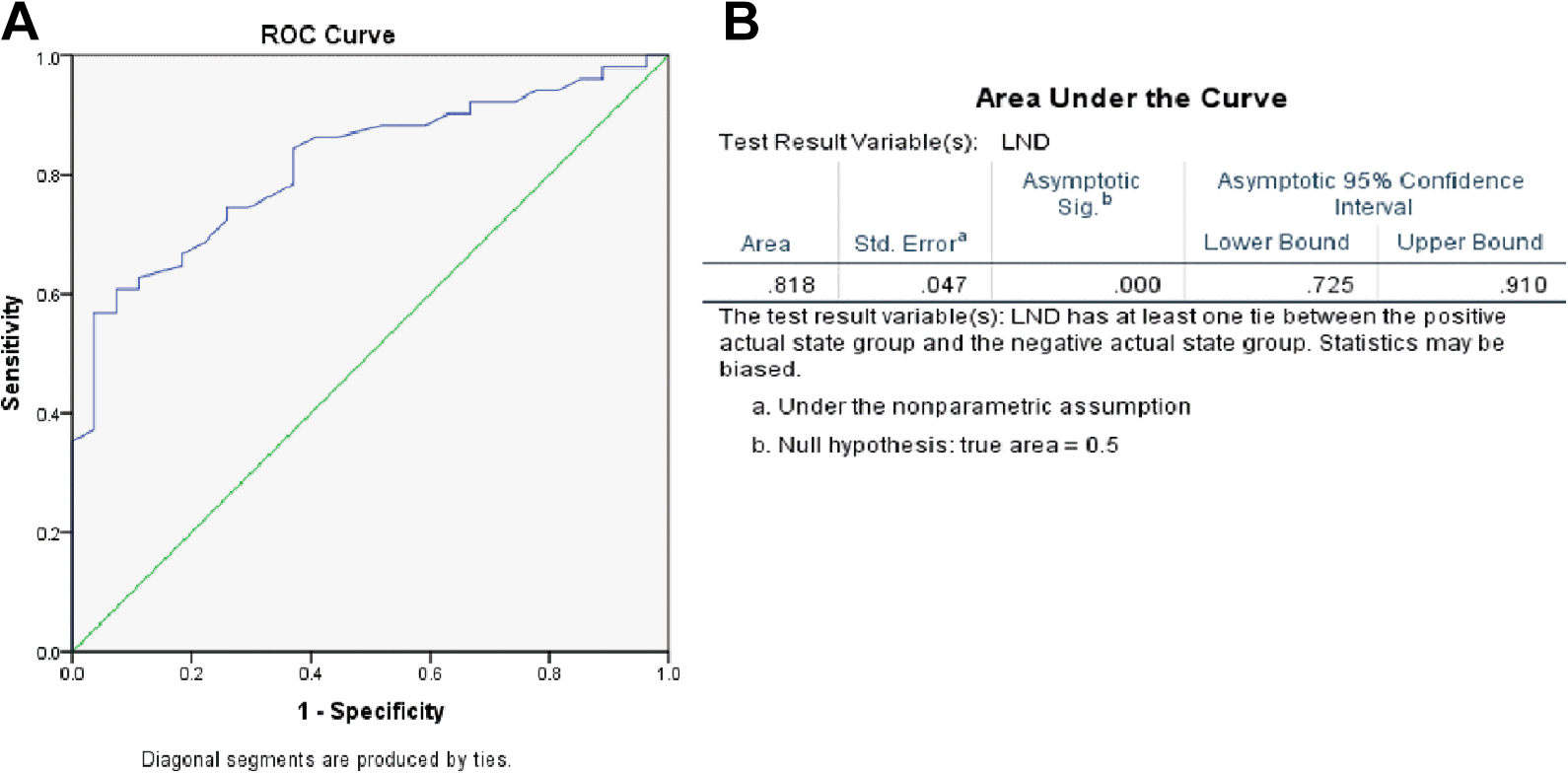
Receiver operating characteristic (ROC) curve and Youden’s index generated by SPSS software for LND for 5-year OS in patients with T3 and T4 pyriform sinus carcinoma; 0.093 was selected as the best cutoff value.
Survival Analysis
In this study, 5-year OS, DSS, DFS, and RRFS rates in the 87 HPSCC were 37.9%, 46.0%, 41.4%, and 54.0%, respectively. Of the 54 (62.1%) cases of death accounting for the 5-year OS, 51 and 3 died from HPSCC and other diseases, respectively. As for 5-year DFS during the follow-up period, recurrence or metastasis was observed in 47 (54.0%) cases, including 10 patients with neck recurrence or metastasis, 13 with both regional recurrence and distant metastasis, 23 cases with distant metastases, and 1 with local and regional recurrence.
According to pathologic examination and the cutoff value of 0.093, the study patients were categorized into 3 groups: pN0 (group A; n = 9, 10.3%); LND < 0.093 (group B; n = 30, 34.5%) with); LND ≥ 0.093 (group C; n = 48, 55.2%). The characteristics of these 3 groups were compared and showed that pN status was only factor of significant differences (P < .01; Table 2). Five-year OS rates in groups A, B, and C were 55.6%, 43.3%, and 31.3%, respectively (P = .028; Figure 3A); while 5-year DSS in groups A, B, and C were 66.7%, 50.0%, and 39.6%, respectively (P = .007; Figure 3B); 5-year DFS in groups A, B, and C were 66.7%, 46.7%, and 33.3%, respectively (P = .012; Figure 3C); and 5-year RRFS in groups A, B, and C were 77.8%, 64.5%, and 42.6%, respectively (P = .007; Figure 3D). In subgroup analysis, 5-year OS rates in patients with LND < 0.093 and ≥ 0.093 were 46.2% and 31.3%, respectively (P = .016; Figure 4A); 5-year DSS rates were 53.8% and 39.6%, respectively (P = .002; Figure 4B), 5-year DFS rates were 51.3% and 33.3%, respectively (P = .005; Figure 4C), and 5-year RRFS rates were 67.5% and 42.6%, respectively (P = .002; Figure 4D).
Comparison of Characteristics Among Groups A, B, and C.

Abbreviations: CCRT, concurrent chemoradiotherapy; RT, radiotherapy.
a Indicates a significant difference, P < .05.
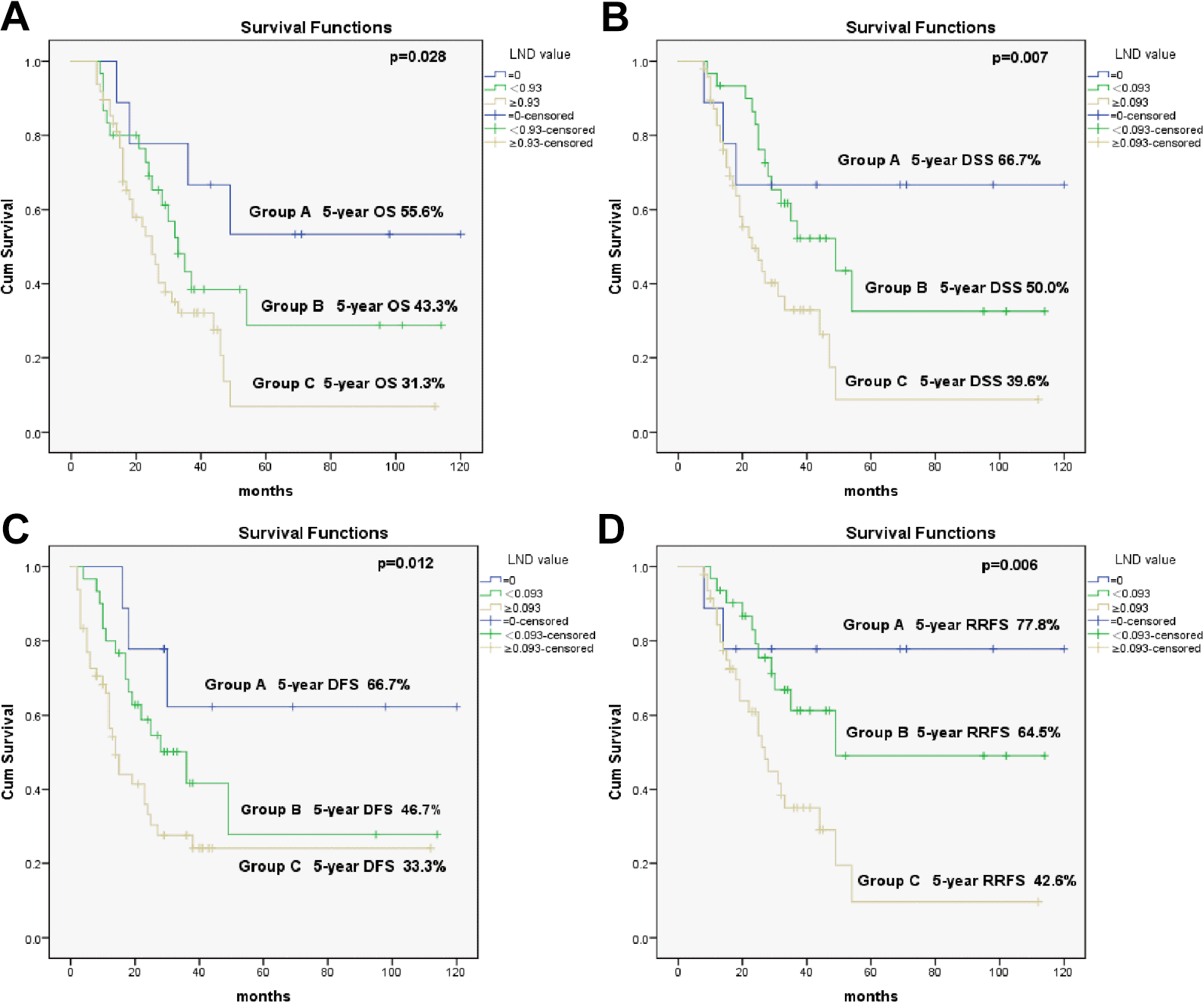
Kaplan–Meier curves for 5-year overall survival (OS) (A), disease-specific survival (DSS) (B), disease-free survival (DFS) (C), and regional recurrence-free survival (RRFS) (D) in patients with T3 and T4 pyriform sinus carcinoma. Group A, LND = 0; group B, LND < 0.093; group C, LND ≥ 0.093.
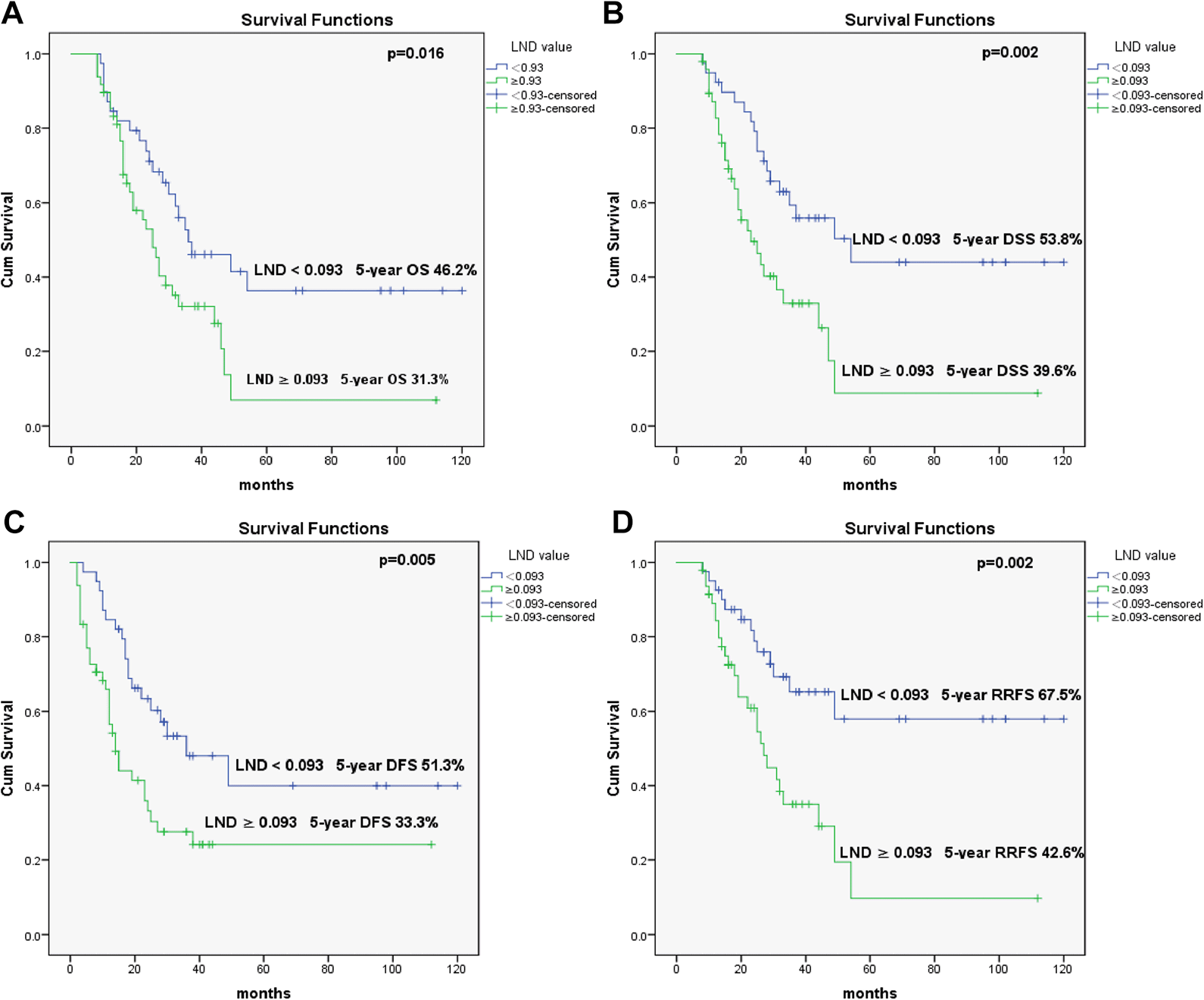
Kaplan–Meier curves for 5-year overall survival (OS) (A), disease-specific survival (DSS) (B), disease-free survival (DFS) (C), and regional recurrence free survival (RRFS) (D) in patients with T3 and T4 pyriform sinus carcinoma showing LND < 0.093 and ≥ 0.093.
The prognostic values of clinicopathological variables in the 87 patients with PSC were also assessed. In Kaplan–Meier survival curves, pT stage, pN stage, treatment, extracapsular spread, ≥4 positive lymph nodes, and LND ≥ 0.093 were significant prognostic predictors. However, further multivariate analysis using the Cox proportional hazard model showed that only pN stage, extracapsular spread, ≥ 4 LNM, and LND ≥ 0.093 were independent risk factors for 5-year OS, DSS, DFS, and RRFS. Only pT stage and treatment were significant risk factors for 5-year DSS and DFS (Table 3).
Univariate and Multivariate Analysis of 5-Year OS, DSS, DFS, and RRFS.

Abbreviations: CCRT, concurrent chemoradiotherapy; HR, hazard ratio; LND lymph node density; RT, radiotherapy.
aIndicates a significant difference, P < .05.
Discussion
For patients with HPSCC with T3 and T4 disease stages, there are limitations in the current curative treatments and prognostic factors, and survival outcomes remain unsatisfactory, suggesting the need for applicable and reliable methods or parameters for more effective disease management.
Moderate and poor differentiation, pN2 and N3, extracapsular spread, and bilateral cervical LNM are more common in patients with stage T3 and T4 PSC (Table 1 and Figure 1), revealing very refractory treatment in these patients. The Kaplan–Meier method and log-rank test showed that the 5-year OS rate of pN0 cases (group A) was almost twice for patients with LND = 0 compared to those with LND ≥ 0.093 (group C; 55.6% vs 31.3%), as well as 5-year DSS (66.7% vs 39.6%), DFS (66.7% vs 33.3%), and RRFS (77.8% vs 42.6%; Figure 3A-D). In addition, patients with LND ≥ 0.093 had worse 5-year OS, DSS, DFS, and RRFS compared with those with LND < 0.093 (all P < .05; Figure 4A-D). The results indicated that the PSC patients with an LND of 0.093 or higher had significantly worse treatment outcomes. Even after adjustment by multivariate analysis using the Cox proportional hazard model, LND ≥ 0.093 remained an independent risk factor for 5-year OS (HR = 1.62, 95% CI: 1.15-2.29, P = .006), DSS (HR = 1.86, 95% CI: 1.24-2.80, P = .003), DFS (HR = 0.45, 95% CI: 0.24-0.85, P = .014), and RRFS (HR = 2.97, 95% CI: 1.43-6.17, P = .004). Together these data suggest that the PSC patients with a higher LND, especially for LND ≥ 0.093, would fare worse than patients with a lower LND.
Due to simultaneous determination by the number of positive lymph nodes, nodal yield, and nodal staging, LND is more instructive for diagnosis than the TNM staging system, 11 and increasing attention has been paid to its predictive role for OS, DSS, and regional control in patients with head and neck cancers. 13,18 To date, a few studies have demonstrated that LND is a reliable parameter in predicting the outcomes of surgical therapy and neck dissection in patients with HPSCC. In 105 patients with HPSCC, Joo et al used 0.055 as a cutoff value for analyzing 5-year OS and DSS. 15 Similarly, Yu et al found significant differences between the LND ≥ 0.14 and LND < 0.14 groups in 5-year DFS, DSS, and OS. 16 Very recently, Lo et al assessed 120 patients with stage 4 HPSCC, and reported that LND ≥ 0.113 reflects worse 5-year OS, DSS, and DFS. 19 However, the HPSCC cases recruited in the 4 studies above all involved hypotharyngeal subsites.
The result of cutoff value of 0.093 is in accordance with an LND of 0.09 in Suzuki’s study, 14 which was significantly correlated with shorter both OS and DSS in patients with HPSCC. However, in most of abovementioned reports, cutoff values for LND ranged from 0.055 to 0.14, with large variation among studies, and differed from the cutoff value of 0.093 in this study. In patients with head and neck cancers (including HPSCC), LND particularly is subject to the harvesting protocol and the extent of neck dissection, 20 while harvested lymph nodes (nodal yield) is susceptible to surgical techniques and the surgeon’s preference. 21 Moreover, overall nodal yield >20 was shown to be related to a significantly increased likelihood of detecting positive lymph nodes in patients with HPSCC with stages T1 and T2 disease. 22 Indeed, several factors could affect positive lymph node detection and nodal yield: (1) individual patient, due to the variable anatomy of the neck; (2) surgeon, with variable surgical choice for neck dissection; (3) and pathologist, due to the variable thoroughness in histopathological workup; each of these steps may cause data loss and undermine the exact value of LND. In this study, all patients with PSC had undergone routine neck dissection, and pathologic nodal staging of nodes removed was conducted without considering the impacts of the clinical N classification or extent of involvement, which therefore guaranteed no bias in patient selection and provided unbiased LND values.
In the present study, extracapsular spread was also identified as a significant risk factor for 5-year OS, DSS, DFS, and RRFS, corroborating Ryu et al who demonstrated that presence of extracapsular spread has an adverse impact on recurrence and survival in 119 156 patients with laryngeal squamous cell carcinoma. 13 Similarly, Brasilino et al reported a significant correlation between extracapsular spread and poor survival in 170 patients with HPSCC or laryngeal cancer. 23
In conclusion, an LND cutoff of 0.093 did help predict the outcome of surgical resection and stratify patients with advanced PSC. A new stratification model incorporating LND into the TNM staging system may provide a valuable guide for predicting prognosis and devising postoperative therapy, as well as follow-up management. This study demonstrated that LND ≥ 0.093 has a high risk of tumor recurrence and mortality and an independent impact on surgical outcomes. Therefore, for patients with HPSCC with LND ≥ 0.093, potent adjuvant therapy and close observation after surgery are strongly recommended. Rigorous patient selection, experienced surgeons and pathologists, standardized surgical techniques and neck dissection, and optimized data analysis could minimize the potential subjective bias and improve the accuracy of LND. Such efforts should provide first-line of evidence for the treatment of patients with HPSCC.
The main limitations of this study include its retrospective nature, small cohort size and single institution involvement, and coexistence of T3 and T4 patients, which may lead to some bias of LND in the current results. Therefore, further studies with large cohorts or authoritative international database analyses are required to validate the prognostic value of LND and its cutoff value.
Supplemental Material
Supplemental Material, Table_S1-Youden_index - Prognostic Value of Lymph Node Density in Patients With T3 and T4 Pyriform Sinus Carcinoma
Supplemental Material, Table_S1-Youden_index for Prognostic Value of Lymph Node Density in Patients With T3 and T4 Pyriform Sinus Carcinoma by Lifeng Jia, Jingya Li, Ziyuan Zhou and Wei Yuan in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
L.F.J. designed the study, performed the statistical analysis, and wrote the manuscript. J.Y.L. assisted in collection of the clinical data. Z.Y.Z. helped to perform the statistical analysis. W.Y. conceived the study, supervised the experiments, and edited the manuscript. All authors read and approved the final manuscript. This retrospective study was approved by the Institutional Review Board and Ethics Committee of Southwest Hospital, and the requirement for informed consent was waived because of the anonymous nature of the data assessed. Trial registration number ChiCTR1800019377 (retrospectively registered), name of registry Chinese Clinical Trial Registry, date of registration 20181107.
Acknowledgments
The authors thank Dr Hui Lin at the Department of Cardiology, Xinqiao Hospital, Army Medical University for positive and constructive suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China [grant numbers 81470694 and 81271080] to Wei Yuan, and the Postdoctoral Science Foundation of China [grant number 2017M623367] to Lifeng Jia.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.