
Abstract
BACKGROUND:
Endometrial cancer is one of the most common tumor of the woman genital organs.
OBJECTIVE:
The goal of this study was to determine the lipocalin-2 levels in patients with endometrial cancer compared to those with normal endometrium or mild endometrial pathologies.
METHODS:
Study included 123 patients with BMI
RESULTS:
Significantly lower median NGAL serum levels were found in a group of patients with normal endometrium compared to the endometrial cancer group,
CONCLUSIONS:
Our preliminary studies demonstrate that lipocalin-2 may be of value in the diagnostics of uterine body cancers.
Introduction
Endometrial cancer is widely prevalent, especially in the developed countries. Obesity is the main factor influencing its development. Adipose tissue is involved in metabolism, immune response and plays an endocrine function. In 2007 adipose tissue was shown to produce a glycoprotein – neutrophil gelatinase-associated lipocalin (NGAL), also known as siderocalin or lipocalin-2 [30]. It was first identified in active neutrophils as a protein covalently bound to human neutrophil gelatinase, hence the name. This 178-amino acid protein belongs to the family of extracellular matrix proteins. It is a risk factor for insulin resistance, diabetes, and chronic or acute inflammatory conditions [38, 41, 44]. It also participates in oncogenesis [9, 10, 20].
Elevated expression of lipocalin-2 was demonstrated in tissues obtained from tumors of the breast, colon, ovary or pancreas [11, 17, 22, 29, 39, 40, 42, 43, 45]. Reduced expression of E-cadherin and resultant increased mobility and invasiveness of tumor cells was noted in colorectal cancer cell lines overexpressing lipocalin-2 [17]. Recent studies on endometrial cancer showed that lipocalin-2 contributes to progression of this tumor. Immunohistochemical studies confirmed greater expression of lipocalin-2 in endometrial cancer compared to atypical endometrial hyperplasia [21, 27, 28]. The goal of this study was to evaluate NGAL diagnostic value in diagnosing endometrial cancer in patients with abnormal bleeding and pathological endometrium changes in the USG image.
Material and methods
Study included 123 patients with BMI
Patients with endometrial cancer – Patients with normal endometrium – Patients with endometrial polyps – Patients with submucosal leiomyomas –
Population data characteristics of patients from control and examined group
In each of the subgroups patients were considered for hormonal status and depending on the BMI. BMI was calculated using following formula:
Among the group of patients with endometrial cancers we identified 47 patients with endometrioid endometrial carcinoma, and 5 patients with non-endometrioid endometrial carcinoma.
Patients from the endometrial cancer group were divided according to tumor grading into G1
FIGO 1 and 2 patients, FIGO 3 and 4 patients,
Five milliliters of blood was collected from each patient for protein levels determination on the occasion of routine preoperative testing and centrifuged. The serum was subsequently frozen and stored at
The relationship between NGAL and BMI in the whole group of patients.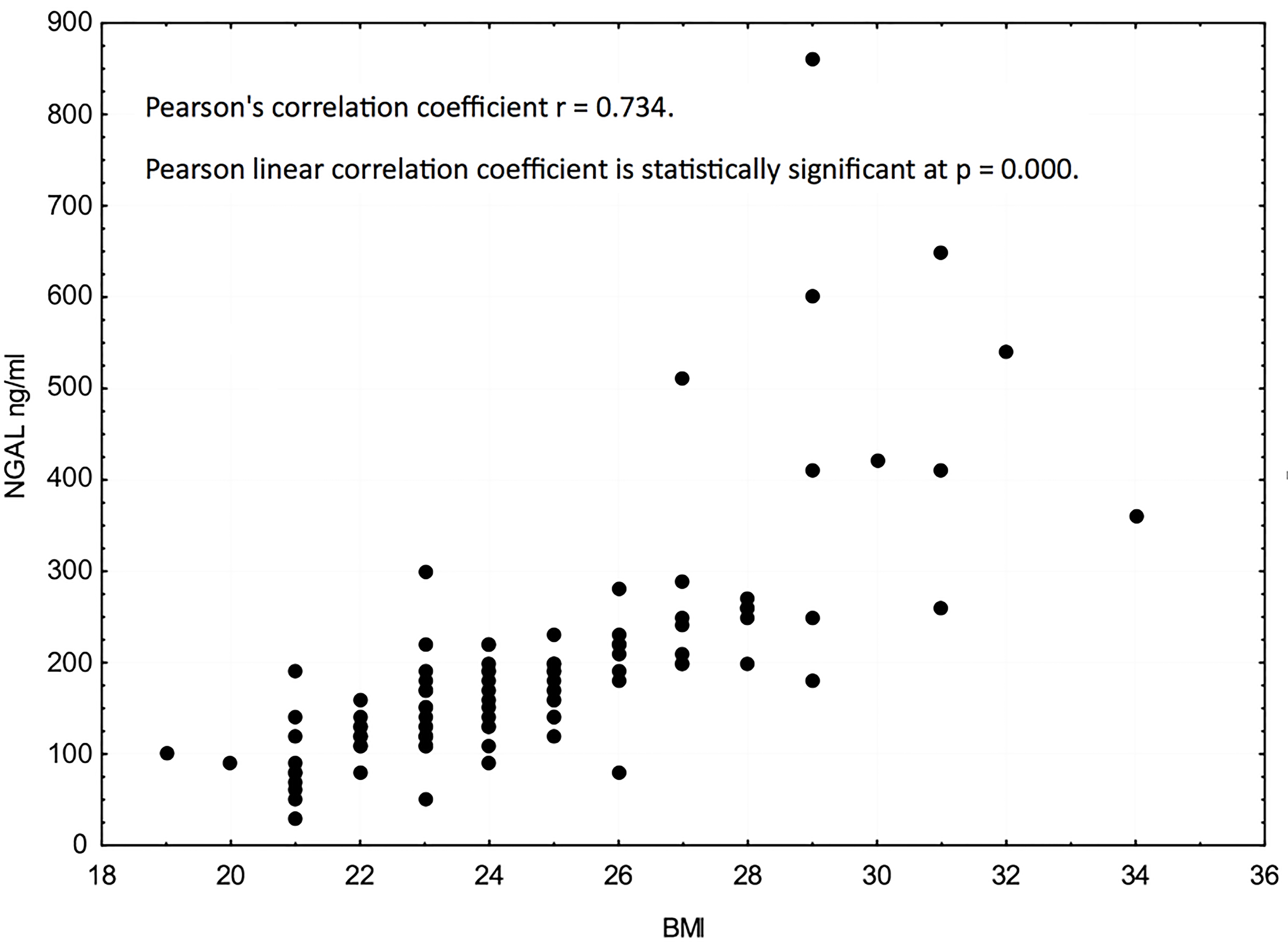
Lipocalin-2/NGAL concentrations were quantified in serum by fluorescent bead-based immunoassays (Luminex Corporation, Austin, TX, USA) using commercial Human Cardiovascular Disease (CVD) Magnetic Bead Panel 2 (Merck Millipore, Billerica, MA, USA). CA125 was determined using ARCHITECT CA 125 II assay [Reagent Kit No 2K45], Abbott Diagnostics, Illinois, USA. Analytical sensitivity was 1.0 U/mL. Serum HE4 concentrations were measured using the Elecsys ECLIA assay [Kit No 05950929190], Roche Diagnostics Ltd, Rotkreuz, Switzerland running on the cobas e 601 analyzer. Detection limit – 15.0 pmol/L. Statistical analysis was performed using STATISTICA 9.1 PL software. Descriptive characteristics of the examined population of patients were prepared, including the minimum, maximum, mean and median values. Because the distributions of the study traits were not normal, for evaluation positional parameters such as median were used. Non-parametric tests with Kruskal-Wallis test and Dunn’s post-hoc test for comparisons between three groups were used and Mann-Whitney’s U-test for comparison between two groups in terms of distribution compatibility of analyzed variables were used.
Protein concentrations distribution in the individual subgroups
Protein concentrations distribution in the individual subgroups
NGAL – neutrophil gelatinase associated lipocalin, HE4 – human epididymis protein 4, CA125 – cancer antigen 125, SD – standard deviation.
For the selected groups, the receiver operating characteristic (ROC) curves were obtained and the area under curve (AUC) was calculated with 95% confidence intervals according to the nonparametric method of DeLong [12]. A
The study used a logit model, where
The differences between the NGAL medians in groups.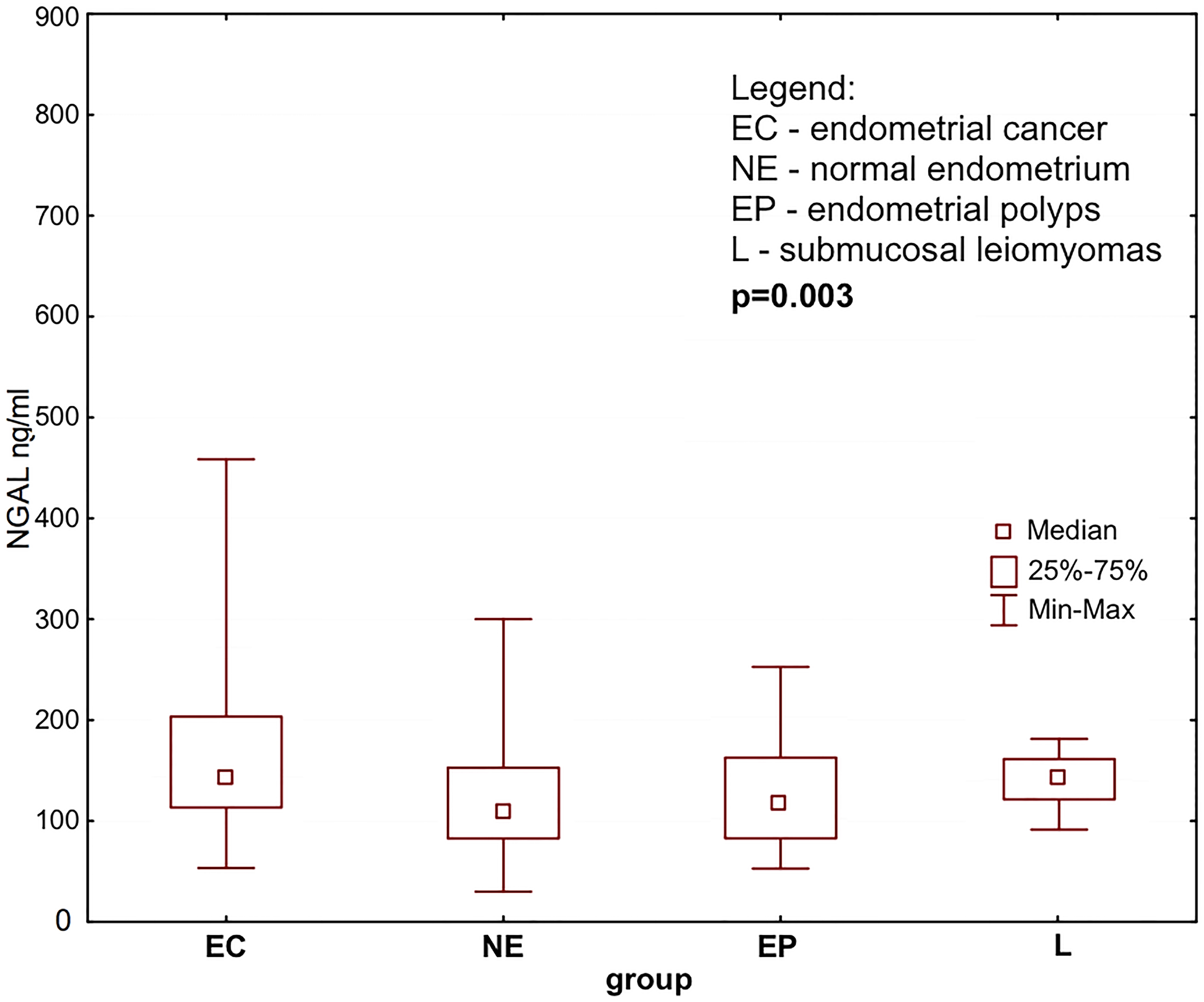
Resolution number: KB-0012/77/12 of the Bioethics Committee of the Pomeranian University of Medicine in Szczecin of 13 October 2012. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Written informed consent was provided by the patients as well as the physician. All the patients have signed informed consent for the study, which has been signed and initialed by the doctor on each side. Patients read carefully the information and were able to ask questions.
Consent for publication
All patients included in the study signed conscious consent.
Results
The Kruskall-Wallis test show no differences in age distributions in the populations of the study groups. Statistically significant correlations were noted between patient BMI and concentrations of lipocalin-2 protein (
There was no correlation between patient BMI and serum concentrations of HE4 and CA125. We observed statistically significant differences in mean serum levels of lipocalin-2, HE4 and CA125 between the group of endometrial cancer patients and the group of patients with benign changes endometrium, both as regards the entire study population and after stratification based on BMI and menopausal status. The distribution of protein concentrations in the individual subgroups are shown in Table 2.
The distribution of lipocalin-2 was compared in patients group with normal endometrium and in group with endometrial cancer. A statistically significant difference was found between the distributions (
Protein concentration behavior depending on the clinical stage and cancer histopathological differentiation
Protein concentration behavior depending on the clinical stage and cancer histopathological differentiation
NGAL – neutrophil gelatinase associated lipocalin, HE4 – human epididymis protein 4, CA125 – cancer antigen 125, FIGO – Fédération Internationale de Gynécologie Obstétrique (International Federation of Gynecology and Obstetrics), G [1–3] – grading,
NGAL ROC curve of endometrial cancers and endometrium benign changes comparison with NGAL ROC curve of endometrium cancers and normal endometrial.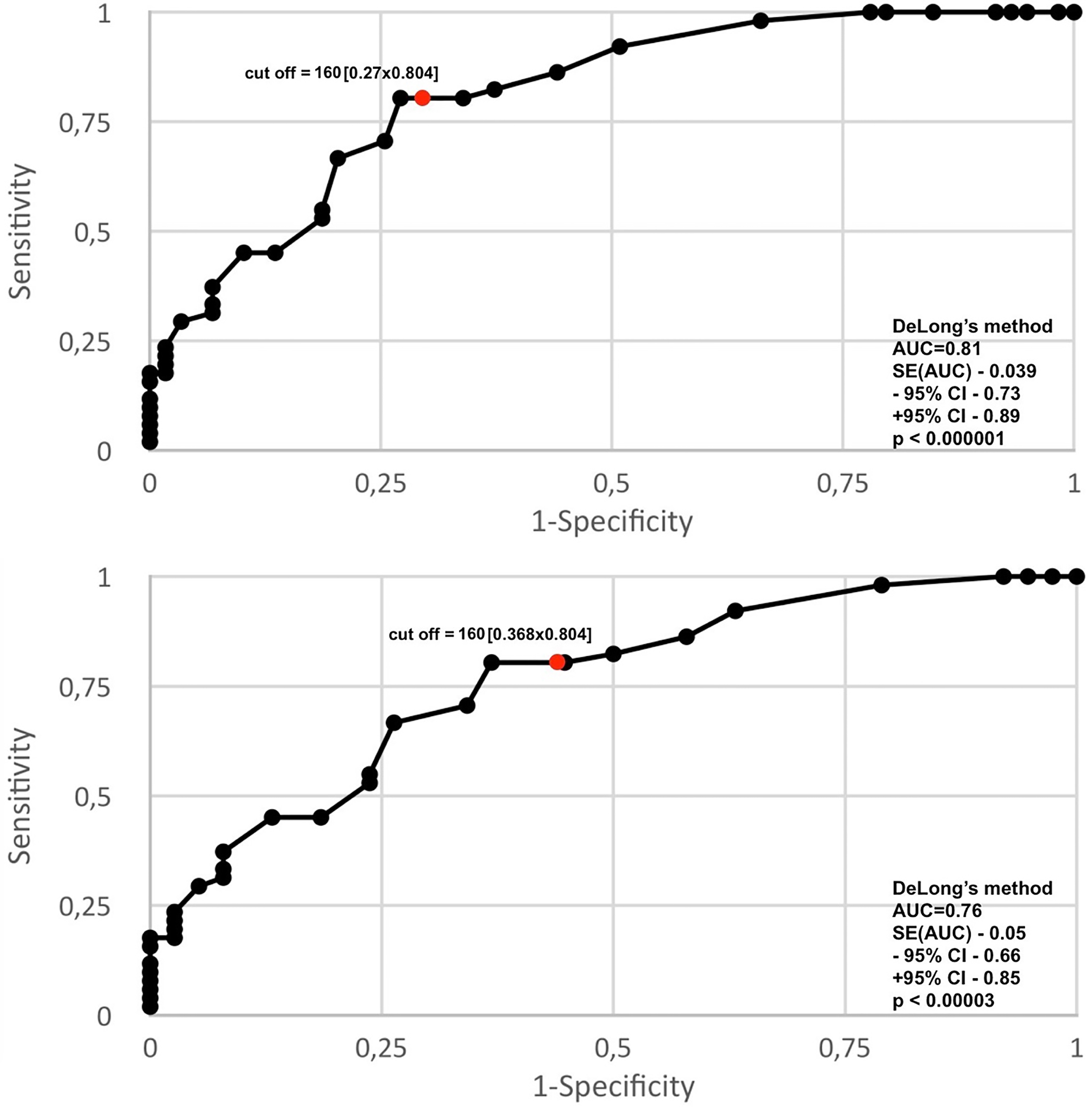
HE4 and CA125 ROC curves for endometrial cancers and endometrium benign changes.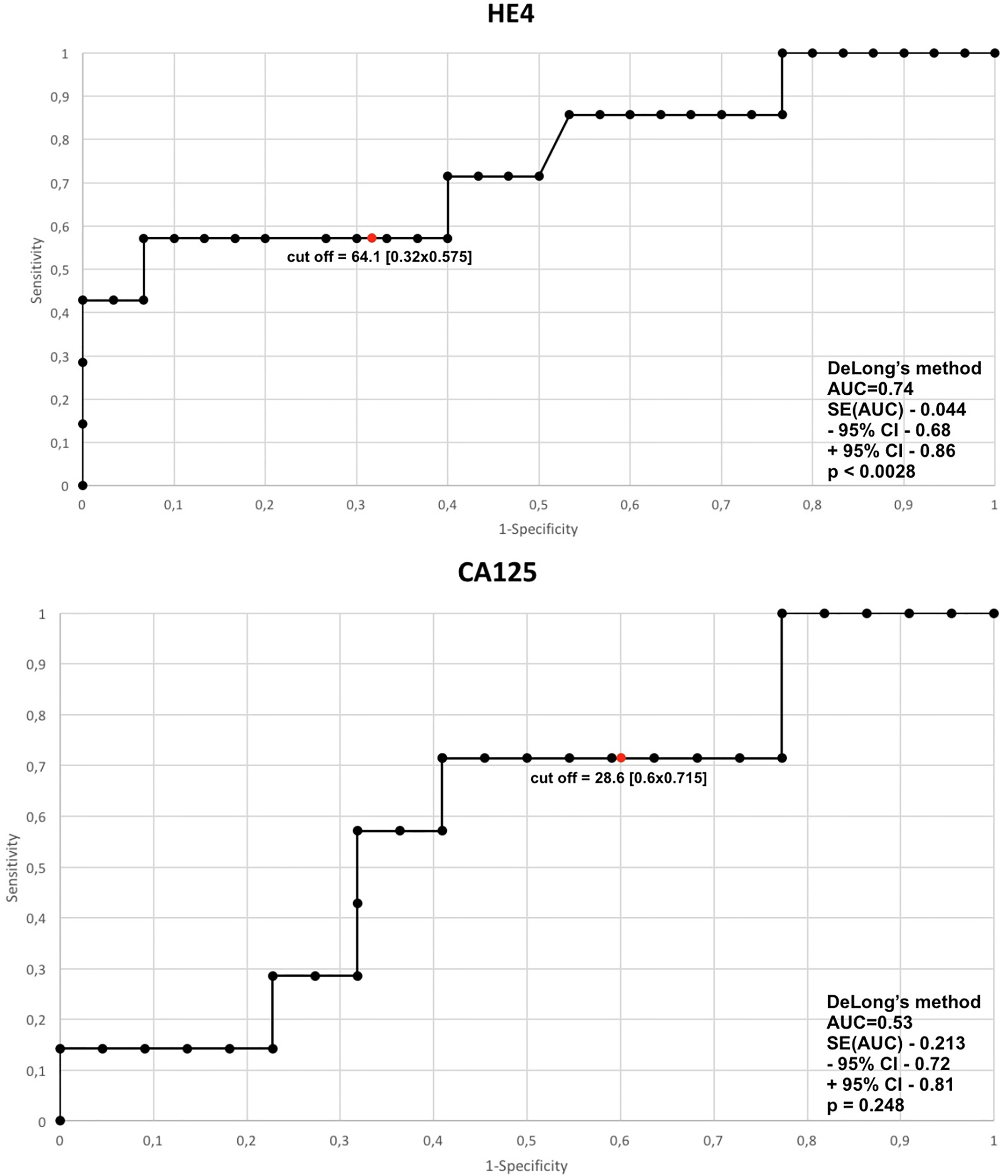
In order to evaluate the diagnostic values of lipocalin-2, HE4 and CA125, ROC curves were plotted and the areas under the ROC curves (AUC) were calculated. Area under ROC curves for lipocalin-2 protein as a diagnostic test, differentiating between endometrial cancer and other benign changes endometrium is AUC – 0.81 (
Table 4 shows the sensitivity and specificity values for lipocalin-2, HE4, and CA125 based on hormonal status. We found higher sensitivity of lipocalin-2 protein for all analyzed women (84%) and for premenopausal and postmenopausal women (82%/81%) compared to the HE4 marker (66% and 64%/67% respectively) and CA125 (52%, 63% and 54%). The HE4 marker showed a greater specificity compared to lipocalin-2 and CA125 in two study group and was: 93% vs 78% vs. 54% among all analyzed women, 90% vs 80% vs 59% in premenopausal women and 85% vs 87% vs. 64% in the postmenopausal group.
Lipocalin-2 protein concentrations analysis depending on the degree of histopathological differentiation and clinical stage of the cancer
We demonstrated statistically significant correlation between serum concentrations lipocalin-2 among patients with various degrees of histopathological tumor differentiation (G3 versus G1)
FIGO and lipocalin-2 logistic regression model
A logistic regression model for the lipocalin-2 protein was created regarding FIGO. The odds ratio is 3.66. The model created reveals that the chances of a patient being in a more advanced group is higher for increased level of lipocalin-2. The model is statistically significant,
Individual proteins sensitivity and specificity depending on hormonal status
Individual proteins sensitivity and specificity depending on hormonal status
NGAL – neutrophil gelatinase associated lipocalin, HE4 – human epididymis protein 4, CA125 – cancer antigen 125, PM – premenopausal, M – postmenopusal.
In 80% of cases endometrial cancer is associated with overweight or obesity. Adipose tissue plays an endocrine role, excreting adipokines, which play various activities in the body. Lipocalin-2 plays a role in development of insulin resistance, glucose intolerance and chronic inflammation. Developing inflammatory process leads to increased production of proinflammatory cytokines [8].
There are similar reports in the literature saying that obese and overweight patients have higher concentrations of lipocalin-2 [30, 38, 41, 44]. In obese patients the paracrine signaling loop becomes dysregulated. High concentrations of adipocytokines begin to interact, weakening the role of adipose tissue as an immune organ and leads to augmented cell migration and endothelial damage.
Endometrial actions of lipocalin-2 have not been fully investigated. In their study on endometrial cancer cell lines Lin et al. observed reduction in initiated apoptosis, change in cell proliferation and stimulation of cytokine secretion, especially interleukin 8 and 6, after 24 hours of incubation. It was shown in the above studies that secretion of lipocalin-2 also depends on sex hormones, particularly estrogens, which are related to proliferation and apoptosis periodically taking place in the endometrium of menstruating women. Elevated levels of lipocalin-2 are noted in patients with higher serum glucocorticoid and estrogen concentrations [23].
Our study revealed augmented lipocalin-2 levels in patients with leiomyomas compared to those with normal endometrium. Lipocalin-2 elevation may result from higher concentrations of estrogens among patients with leiomyomas. Lipocalin-2 is also considered an acute phase protein [18]. The peak of incidence of endometrial cancer is observed in the perimenopausal age, which is associated with relative hyperestrogenism and resultant increase in lipocalin-2 expression. Moreover, lipocalin-2 production takes place in the adipose tissue. The greater the BMI, the higher serum lipocalin-2 concentration. Greater amounts of fat tissue are associated with more extensive aromatization of adrenal androstendione to estrone – the main type of estrogen in postmenopausal women.
Considering the carcinogenic effects of lipocalin-2 and its production in follicular tissue, we have decided to investigate the diagnostic potential of this protein as a marker in endometrial cancer.
We have shown that the cut-off point for serum concentration of lipocalin-2 that differentiates endometrial benign changes from endometrial cancer is 160 ng/ml. The sensitivity of the test protein was greater than the sensitivity of the HE4 and CA125 markers in the whole patient population, as well as the hormone status of the patients. The sensitivity and specificity of the HE4 marker was significantly higher than CA125, which corresponds to Liu et al. reports. Comparing early detection opportunities of endometrial cancer with CA125 and HE4, they have shown that the HE4 marker is more sensitive and specific regardless of the age of the patients and their hormone status [25].
In our studies, the CA125 AUC was 0.53 and HE4 AUC was 0.74, which was comparable to the results presented by Angioli et al., where the AUC was 0.54 and 0.86 respectively [4]. Angioli in the summary review of 5 studies found that all authors found statistically significantly higher HE4 concentration in the group of patients with endometrial cancer compared to the control group. The ROC and AUC curves for HE4 are in range from 0.78 to 0.88, which in each case contained the HE4 marker criteria for a good diagnostic test. Moreover, in studies of three independent authors, differences in HE4 serum levels were also statistically significant between the control group and the stage I group [3].
Two authors in their work suggest that in the case of CA125 marker, its serous level increases only in 10% of patients with early stage of endometrium cancer (I and II) [34, 35]. Based on their studies, Angioli and Plotti et al. recommended creation of REM or refined REM B algorithm, according to HE4 marker level and endometrium thickness, which was intended to stratify patients to low or high endometrium cancer risk groups [1, 32, 33].
The specificity of lipocalin-2 was slightly poorer than HE4 marker for the whole group of patients and premenopausal patients, whereas in the postmenopausal patients group, the lipocalin-2 specificity was higher than HE4 specificity and was respectively 87%/85%. The cut-off limit for HE4 between the benign endometrial lesions and endometrial carcinomas in our study was 64.1 pmol/l and was slightly higher than the cut-off point for HE4 in studies by Gasiorowska et al. (58.08 pmol/l) [15]. For CA125 maker cut-off was at level of 28.6 U/ml, opposed to meta-analysis cut-offs from Patsner and Yim (20 U/ml) for early stage of endometrial carcinoma [31]. Hu et al. emphasizes the fact that the HE4 marker is more sensitive than CA125, but the results of these markers as diagnostic tests are not satisfactory [16].
Angioli et al. confirmed that the HE4 level over 70 pmol/l at diagnosis had 67% sensitivity and 53% specificity in predicting recurrences of endometrial cancer [2, 5]. Lipocalin-2 concentration was analyzed in relation to tumor size, advancement and presence of metastases [24]. It was demonstrated that elevated lipocalin-2 expression in endometrial cancer is tightly correlated with greater tumor aggressiveness and poorer prognosis [26]. Increased lipocalin-2 expression was noted in endometrial cancers compared to atypical or simple endometrial hypertrophy [27].
Miyamoto et al. proved in their studies that high expression of lipocalin-2 and its receptor SLC22A17 is associated with poorer prognosis in a group of patients with endometrial cancer [28].
High level of lipocalin-2 expression is associated with elevated concentrations of IL-8, which is responsible for increased cell proliferation, inhibition of apoptosis and cell migration. Our studies showed that higher clinical staging of endometrial cancer correlates with increase of lipocalin-2 serum concentration. Concentration of lipocalin-2 have been examined in other cancers as well. Observations regarding breast cancer demonstrate increasing lipocalin-2 expression with advancement of the disease [39]. Similar reports pertain to chronic myeloid leukemia [19, 20]. Expansion of tumor mass with increasing lipocalin-2 expression has also been described [6]. Moniaux et al. reported that lipocalin-2 might be a marker for early detection of pancreatic cancer [29]. Patients with elevated levels of lipocalin-2 are characterized by worse prognosis in esophageal and stomach cancer, although some publications report protective function of lipocalin-2 in thyroid and renal cancer [6, 7, 13, 14, 19, 36, 37, 42].
The high sensitivity of lipocalin-2 with comparable specificity to HE4 allows us to believe that lipocalin-2 will prove to be useful in the endometrium cancer diagnosis.
Lipocalin-2 as a protein that combines the features of a metabolic factor and proliferative factor has a multidirectional ability to participate in the development of endometrial cancer. Proliferative effects of lipocalin-2 are both direct and indirect, through interaction with extracellular matrix metalloproteinases.
In our research, the relationship between BMI and lipocalin-2 raw materials has been confirmed. The results obtained by us are consistent with the reports of other authors [38]. In a group of obese patients, the sensitivity of lipocalin-2 protein differing endometrium benign changes from endometrium cancer may be slightly lower, but still meets the criteria of a good diagnostic test.
Studies on a larger group of patients will unambiguously answer question whether or not lipocalin-2 serum concentration will allow us to isolate patients with high risk of endometrial cancer and subject them for endometrial sampling.
Conclusion
Our preliminary studies demonstrate that lipocalin-2, which reaches significantly higher levels in patients with endometrial cancer, may be of value in the diagnostics of uterine body cancers.