Soluble LAG3 acts as a potential prognostic marker of gastric cancer and its positive correlation with CD8 + T cell frequency and secretion of IL-12 and INF- γ in peripheral blood
Free accessResearch articleFirst published online August, 2018
Soluble LAG3 acts as a potential prognostic marker of gastric cancer and its positive correlation with CD8 + T cell frequency and secretion of IL-12 and INF- γ in peripheral blood
Gastric cancer (GC) is the second most common lethal cancer worldwide and lymphocyte-activation gene 3 (LAG3) as a therapeutic target for cancers has been investigated. Herein, our study is to clarify the value of peripheral blood (PB) soluble LAG-3 (sLAG3) in GC.
METHODS:
Peripheral serum samples of GC patients and healthy people were collected for the measurement of serum levels of sLAG3, carcinoembryonic antigen (CEA), IL-12 and IFN-. Additionally, ROC and Kaplan-Meier curves were adopted to identify the diagnostic and prognostic values of sLAG-3 in patients with GC. Then, GC-bearing mice were treated with recombinant sLAG3. The tumor volume was measured, and CD8T cell frequency was detected in PB and tumor-ininfiltrating area. Additionally, the expression of IL-12 and IFN- in T cells was assayed and the overall survival of mice was analyzed.
RESULTS:
sLAG3 in PB was poorly expressed and its expression was positively correlated with IL-12 and IFN- expression in GC patients. sLAG3 was proved to have a higher diagnostic value than CEA in GC. Moreover, high sLAG-3 expression is found in relation to a better prognosis in GC. The in vivo experiments indicated that sLAG-3 might inhibit the tumor growth, and promote the secretion of CD8T cells, IL-12 and IFN-. Furthermore, sLAG-3 was able to prolong overall survival and increase survival rate of GC-bearing mice.
CONCLUSION:
Based on these findings, we conclude that sLAG3 positively regulates CD8T cells, IL-12 and IFN-, and function as a prognostic marker for GC, which might be a potential target in the treatment of GC.
Gastric cancer (GC) is known as one of the primary cancers and still one of the leading causes of morbidity and mortality in malignant diseases [1]. In 2012, about 140,000 people have been confirmed as GC in European, which makes it the sixth most common diagnosed cancer [2]. GC is described as a heterogeneous disease, accompanied with alternative pathways of carcinogenesis and diverse environmental factors [3]. It is estimated that the proportion of young GC patients is between 2% and 9% with an age less than 40, and the majority of the patients were over 35 years [4]. The risk factors for GC include non-modifiable and modifiable respects, such as radiation, genetic predisposition in some families, and history of Epstein-Barr virus infection, as well as Helicobacter pylori infection, smoking, pernicious anemia, diet and geography [5]. The following treatments are applied in GC, involving local tumor resection, chemotherapy, chemoradiotherapy, laparoscopic gastrectomy and surgery [6]. It has been suggested that gastrectomy is the most accepted treatment of GC, but the prognosis is still poor especially for the patients in the advanced stage and the mortality rate is also high [7]. For example, patients with GC after gastrectomy treatment would probably suffer various physical issues, such as hypoglycemia, reflux, diarrhea, dumping syndrome, and activity limitation [8]. Recently, lymphocyte activation gene 3 (LAG3) is reported to play a crucial role in the complicated regulation of immunologic functions [9].
LAG3 is a membrane glycoprotein belonging to the immunoglobulin (Ig) superfamily and functions as an immune checkpoint receptor. LAG3 is a cell surface localized protein expressed in activated T cells and human natural killer cells, and a soluble LAG3 (sLAG3) variant could activate immune cells [10, 11]. The expression of surface LAG3 is elevated in activated human T cells through the activation of interleukin (IL)-2, IL-7, and IL-12, and could be observed in all human T cells for two to three days after activation [12]. A higher level of LAG3 is needed to regulate overt activation and restrict the autoimmunity onset [13]. In addition, Huang et al. found that LAG3 and programmed death-1 (PD-1) co-existed in CD8T cell activation in vitro at the lysosomes, trans-Golgi vesicles, microtubule organizing center, and early/recycling endosomal compartments [14]. It is reported that CD8T cells play a key role in tumor control [15]. The expression of PD-1 and LAG-3 on both CD8T cells and CD4T cells increased and may be associated with damaged cell-mediated immunity after GC surgery [16]. In this study, we are going to verify the hypothesis that soluble LAG3 was as a potential prognostic marker in gastric cancer patients and its association with CD8T cell frequency and secretion of IL-12 and INF- in peripheral blood.
Materials and methods
Ethics statement
All participants signed documents of informed consent and the study was carried out in strict accordance with the standard of clinical research and approved by the ethics committee of Affiliated Tumor Hospital of Xinjiang Medical University. The animal experiment was carried out in strict accordance with the recommendations in the Guide for the Care and Use of Laboratory Animals.
Study subjects
Between March 2015 and March 2017, a total of 308 GC patients admitted to Gastroenterological Surgery of Affiliated Tumor Hospital of Xinjiang Medical University were selected as the case group, including 177 patients of Han nationality and 131 of Uygur nationality (212 males and 96 females) with a mean age of 60.40 10.78 years. Among them, 182 patients were with infiltration of GC cells to serosal layer while 126 were not, and 107 were with lymphatic metastasis while 201 were not. Besides, 192 patients were with gastric antral cancer, 67 with gastric corpus cancer and 49 with gastric cardia cancer. According to the histopathological classification, there were 132 patients of differentiated adenocarcinoma (high differentiation and middle differentiation), and 176 cases of low differentiated adenocarcinoma. Based on the 7 edition of the Union for International Cancer Control-American Joint Committee on Cancer (UICC/AJCC) staging standards, 161 patients were at stage I II and 147 patients were at stage III IV. Inclusion criteria were as follows: all patients received no chemotherapy or radiotherapy before the operation, and all patients with GC were confirmed pathologically after operation. Exclusion criteria were as follows: patients with GC were with coronary heart disease, hypertension, diabetes, liver and renal function impairments after asking for medical history, physical examination and laboratory examination. Additionally, peripheral blood (PB) was collected from 291 healthy people as the control group, which consisted of 148 people of Han nationality, 143 of Uygur nationality including 207 males and 84 females with a mean age of 57.96 9.88 years. A total of 10 mL peripheral venous blood was extracted from the case group at the next morning after hospitalization and the control group the day of physical examination, respectively. Then the blood was centrifuged for 5 min at 4000 r/min, separated and stored at 80C. The 308 patients with GC were followed up for 6–32 months, and complete follow-up data were obtained from all patients. Besides, the survival time of each patient was recorded, and the relationship between sLAG-3 in PB and prognosis of GC was analyzed.
Enzyme-linked immunosorbent assay (ELISA)
The concentration of sLAG-3, IL-12 and IFN- in serum was determined by solid-phase sandwich ELISA, the specific steps were in accordance with the instructions of sLAG-3, IL-12 and IFN- ELISA Kits (Wuhan USCN Sciences Co., Ltd., Wuhan, Hubei, China). The standard products were diluted as ten times continuously, the serum samples were diluted (1:5 dilution), and the corresponding reagents were diluted according to the instructions successively. The standard well (added with standard products), the blank well (without any reagent), the sample well (added with sample) were set, and the sample well was considered as duplicated well. Different concentrations of 100 L standard product solution and the diluted sample were added into the wells, and incubated at 37C for 2 h. The liquid was removed, accompanied with the addition of 100 L solution A into the wells, and incubated at 37C for 1 h. Liquids in the plate were removed, the reaction plate was washed by washing liquid and dried on the thick absorbent paper. The plate was washed for 3 times, added with 100 L solution B and incubated for 30 min. After washing the plate for 5 times, 90 L substrate solution was added into each well, and developed for 15–25 min at 37C, devoid of light. Each well was added into 50 L stop solution, mixed gently, and the blue was turned into yellow. A microplate reader (Thermo Fisher Scientific, Waltham, MA, USA) was adopted to measure the optical density (OD) value of each well at the wavelength of 450 nm. The OD value of the standard products was set as abscissa and the concentration of the standard products was as the ordinate. Standard curve was drawn, concentrations of unknown samples were calculated using standard curve method, and 3 duplicates were set for each sample.
Electrochemiluminescence (ECL)
The detection was performed according to the carcinoembryonic antigen (CEA) kit (Roche Diagnostics GmbH, Mannheim, Germany) and instructions of Roche Cobas e601 immunoassay analyzer (Roche Diagnostics GmbH, Mannheim, Germany). The results were confirmed based on instructions ( 5 ng/mL was positive), and 3 duplicates were set for each sample.
Animal treatment
Forty specific-pathogen-free (SPF) 615 mice (age: 5–6 weeks; weight: 15–20 g) were purchased from Animal center of the Institute of cancer research, Chinese Academy of Medical Sciences (Beijing, China) (Animal license number: SCXK [Beijing] 017). Mouse forestomach carcinoma (MFC) cell line was provided by Shanghai Institute of Biochemistry and Cell Biology, Chinese Academy of Sciences. MFC cell lines were treated and passaged in the 1640 medium containing 10% bovine serum, 100 U/mL penicillin and streptomycin. After that, cells in the logarithmic growth phase were extracted into 1 10 mL cell suspension. The RPMI l640 medium was purchased from Gibeo Laboratories (Grand Island, NY, USA), and the newborn bovine serum was purchased from Sijiqing Bioengineering Materials Co., Ltd., Hangzhou, Zhejiang, China. Recombinant sLAG-3 was purchased from IMMUTEP S.A. (Orsay, France) and dissolved in phosphate buffered saline (PBS) containing 50 mmol/L arginine and 50 mmol/L glutamates. And then, the 0.1 g/mL PBS containing recombinant sLAG-3 solution was prepared, stored in at 80C, and defrosted on the ice before using.
Model establishment
Mice were subcutaneously injected with wild-type MFC cells at their right back with 5 10 cells (0.5 mL) for each mouse. A hard nodule of grain size appeared in the right back subcutaneous of mice was considered as a successful model. Thirty successfully modeled mice were selected and randomly allocated into the sLAG-3, negative control (NC) and blank groups with 10 mice in each group. Each mouse in the sLAG-3 group was subcutaneously injected with 0.1 g recombinant sLAG-3 at left back of mouse at the same time-point of 5–7 day after inoculation of MFC cells [17]. Each mouse in the NC group was subcutaneously injected with 1 mL pure PBS at right back of 615 mice at the same time-point of 5–7 day after inoculation of MFC cells. Each mouse in the blank group received no treatment. The tumor volume (TV) of mice was measured once every 3 days after tumor formation. The maximum diameter (a) and minimum diameter (b) of the tumors in mice were measured using a vernier caliper. The TV was calculated according to the formula, TV 0.5 a b. The experiment lasted for 31 days, the survival rate of mice was recorded at the end of the experiment. Subsequently, all mice were treated with cervical dislocation, and the tumor was separated and the tumor weight was obtained. The mean weight and inhibition rate of tumor were calculated. The tumor inhibition rate (%) (the mean weight of tumor in the blank/NC group the mean weight of tumor in the sLAG-3 group)/the mean weight of tumor in the blank/NC group 100%.
Flow cytometry
Mice were sacrificed at the end of the experiment. Eyeball blood of 5 mL was collected from mice, put into the anticoagulant tubes containing ethylenediaminetetracetic acid (EDTA), and mixed. The tumor area was separated from nude mice, and tumor-infiltrating tissues were separated around the solid tumor and homogenized. Subsequently, 1 g tissue homogenate was then transferred to a centrifuge tube. Ficoll-Paque lymphocyte separation solution (Amersham Biosciences, Uppsala, Sweden) was added in a centrifuge tube, following the addition of 1 mL anticoagulant venous blood and centrifugation for 10 min at 1200 r/min. The liquid of middle-layer was extracted into a new tube, 5 mL normal saline was added to wash, and centrifuged for 5 min at 1000 r/min. And then, the supernatant was discarded, 1 mL normal saline was added to re-suspend cells, which was lymphocyte suspension with a density of 1 10 cell/mL. The lymphocyte suspension (1 mL) was added with 0.1 mL CD8 mouse anti-human monoclonal antibody (BioLegend, San Diego, CA, USA), incubated at room temperature for 30 min, mixed uniformly with 10 mL PBS, and centrifuged for 5 min at 1000 r/min. Subsequently, the supernatant was discarded. The cells were then added with 100 L goat anti-mouse FITC-IgG secondary antibody (Jackson Immunoresearch Laboratories, West Grove, PA, USA), incubated at room temperature for 30 min, devoid of light. After that, the cells were washed with 10 mL PBS, centrifuged with supernatant discarded to remove the fluorescence labeled unbound secondary antibody. Then the cells were mixed uniformly with 1 mL PBS, and placed on the master sample machine to measure after filtering by 300 meshes. Before the measurement, red blood cells were as the standard sample to adjust the coefficient of variation (CV) value within 5%. The flow cytometer (FACS420, BD Biosciences, San Jose, CA, USA) was used to excite 2 W argon laser, with an output power of 300 W and excitation wavelength of 488 nm. The measured data and graphics were input to the HP-300 Consort30 computer, and the corresponding programs were employed to analyze the data. The experiment was repeated 3 times.
Detection of levels of Interleukin-12 (IL-12) and interferon- (IFN-) in tumor-bearing mice
Spleens of mice were extracted under sterile conditions, and splenic lymphocytes of mice were separated using lymphocyte separation solution, added with 5 mL RPMI-1640 medium, and percussed evenly by straw, with a cell density of 2 10–5 10 cells/mL. RPMI-1640 complete medium was used to cover the 96-well plates, and cell suspension was added into the plate, 100 L for each well. Then, the suspension was cultured in a 95% humidity incubator with 5% CO at 37C for 48 h. After 48 h, the cell cultures were transferred into a sterile centrifuge tube using the glass capillary, centrifuged for 20 min at 2500 r/min. The supernatant was collected. IL-12 and IFN- in the supernatant of splenic lymphocytes (time of determination was less than 24 h) were determined according to instructions of ELISA Kit (Jingmei Biotechnology Co., Ltd., Shenzhen, China). Three duplicates were set for each sample.
Statistical analysis
Data were analyzed by SPSS21.0 software (IBM Corp. Armonk, NY, USA). The measurement data were based on normal distribution and represented by mean standard deviation. The -test was employed for mean value comparisons between two groups while One-way Analysis of Variance (ANOVA) was used for comparisons among multiple groups. The enumeration data was expressed by percent (%) while chi-square test was used for comparisons between groups. Receiver operating characteristics (ROC) curve was applied to calculate each variable to diagnose the best boundary value of GC, and the area-under-the-curve (AUC), diagnostic thresholds, diagnostic sensitivity and specificity were identified. The survival rate was calculated by the Kaplan-Meier method, and tested by the log-rank test. 0.05 was considered statistically significant.
Comparisons of the clinical data in patients with GC between the case group and the control group
Clinicopathological factors
Case group ( 308)
Control group ( 291)
Age (years)
0.088
0.767
60
172 (55.84%)
166 (57.04%)
60
136 (44.16%)
125 (42.96%)
Gender
0.378
0.539
Male
212 (68.83%)
207 (71.13%)
Female
96 (31.17%)
84 (28.87%)
Nationality
1.623
0.105
Han nationality
177 (57.47%)
148 (50.86%)
Uygur nationality
131 (42.53%)
143 (49.14%)
Drinking
2.232
0.135
Yes
136 (44.16%)
111 (38.14%)
No
172 (55.84%)
180 (61.86%)
Smoking
0.749
0.387
Yes
177 (57.47%)
157 (53.95%)
No
131 (42.53%)
134 (46.05%)
Family history
10.440
0.001
Yes
73 (23.70%)
39 (13.40%)
No
235 (76.30%)
252 (86.60%)
Note: GC, gastric cancer.
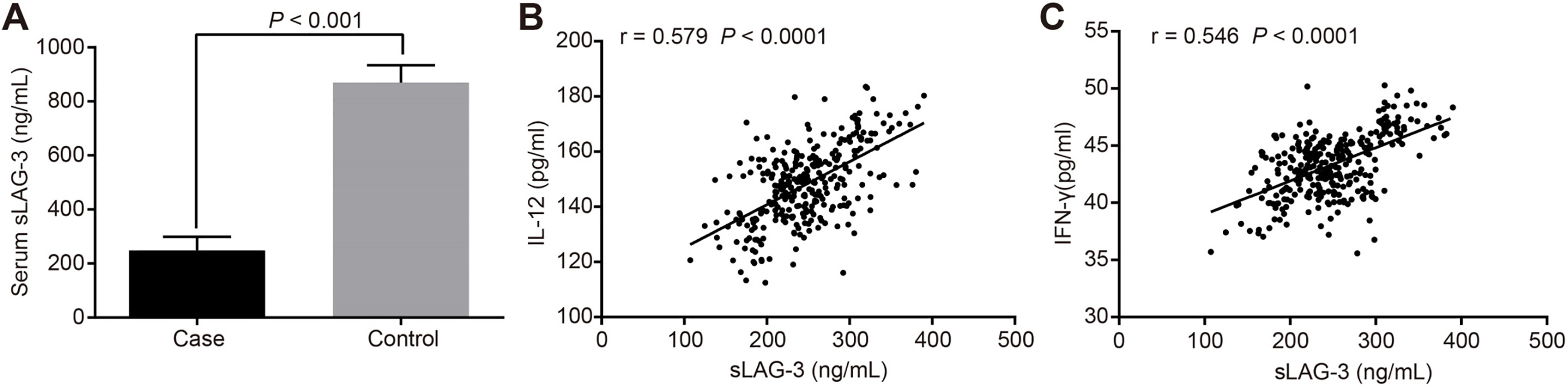
sLAG-3 presented a lower level in the case group than that in the control group, and sLAG-3 was positively correlated with IL-12 and IFN- levels in GC patients. A: ELISA showing serum sLAG-3 level in case and control groups; B: Pearson correlation analysis showing the correlation between sLAG-3 and IL-12 level in GC patients; C: Pearson correlation analysis showing the correlation between sLAG-3 and IFN- level in GC patients. sLAG-3, soluble lymphocyte activation gene-3; GC, gastric cancer. IL-12: interleukin-12; IFN-: interferon-.
Results
Family history accounts for a great factor for GC
The clinical data of the case and control groups are shown in Table 1. No significant difference was found in age, gender, nationality, drinking and smoking composition in the case and control groups (all 0.05). However, the proportion of positive family history was at a higher level in the case group than that in the control group (23.70% vs 13.40%, 0.05).
Correlations between serum sLAG-3 level and clinicopathological factors in patients with GC
Serum sLAG-3 is positive correlated with IL-12 and IFN- level in patients with GC
ELISA was performed to measure the serum sLAG-3, IL-12 and IFN- levels in the case and control groups. The serum sLAG-3 level in the case and control groups was 247.52 51.28 ng/mL and 869.46 64.35 ng/mL, respectively. As shown in Fig. 1, the serum sLAG-3 presented a lower level in the case group than that in the control group ( 0.05). It has been suggested that serum sLAG-3 is expressed at a low level in patients with GC. Moreover, the serum IL-12 and IFN- levels in the case group were 148.15 13.82 ng/mL and 43.29 2.74 ng/ml, respectively, and those in the control group were 232.64 16.23 ng/mL and 72.41 4.38 ng/ml, respectively, indicating that IL-12 and IFN- were poorly expressed in GC patients. Pearson correlation analysis showed that sLAG-3 was positively correlated with IL-12 and IFN- expression ( 0.579, 0.546, all 0.0001).
Serum sLAG-3 expression is closely correlated with TNM stage, depth of tumor invasion and tumor differentiation degree
The correlation between serum sLAG-3 expression and clinicopathological factors in patients with GC was analyzed, included age, gender, nationality, tumor-node-metastasis (TNM) stage, differentiation degree, tumor size, tumor location, depth of tumor invasion and lymphatic metastasis (Table 2). The concerned clinicopathological factors including age, gender, nationality, tumor-node-metastasis (TNM) stage, differentiation degree, tumor size, tumor location, depth of tumor invasion and lymphatic metastasis The expression of serum sLAG-3 in patients with GC presented a higher level in stage I–II than that in stage III–IV ( 0.05). Besides, serum sLAG-3 expression in patients with GC who had not been invaded in the serosa exhibited a higher level while a lower level in patients who had been invaded in the serosa ( 0.05). The expression of serum sLAG-3 in patients with GC with middle and high differentiation was higher than those in patients with low differentiation ( 0.05). And no significant correlation was found between serum sLAG-3 expression and the concerned clinicopathological factors, such as age, gender, nationality, tumor size, tumor location and lymphatic metastasis (all 0.05). As shown in Table 2, the expression of serum sLAG-3 was closely correlated with the TNM stage, depth of tumor invasion and tumor differentiation degree.
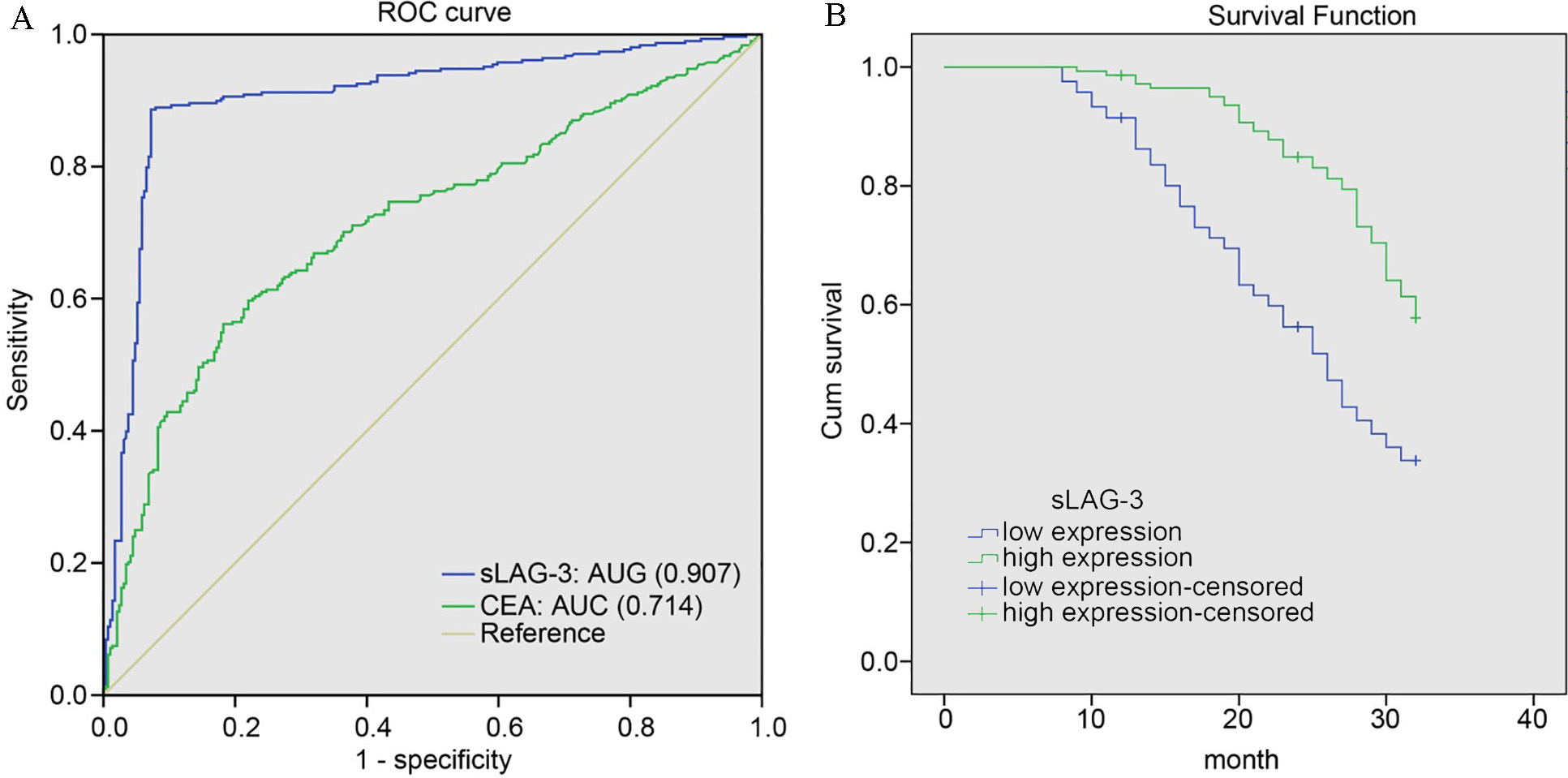
ROC curve results suggest that high sLAG-3 level correlates with longer survival time and better prognosis to GC patients. A: comparison of AUC between serum sLAG-3 and CEA levels in GC patients; B: Kaplan-Meier curve of the relationship between sLAG-3 level and survival time of GC patients. ROC, operating characteristics; AUC, area under curve; sLAG-3, soluble lymphocyte activation gene-3; GC, gastric cancer; CEA, carcinoembryonic antigen.
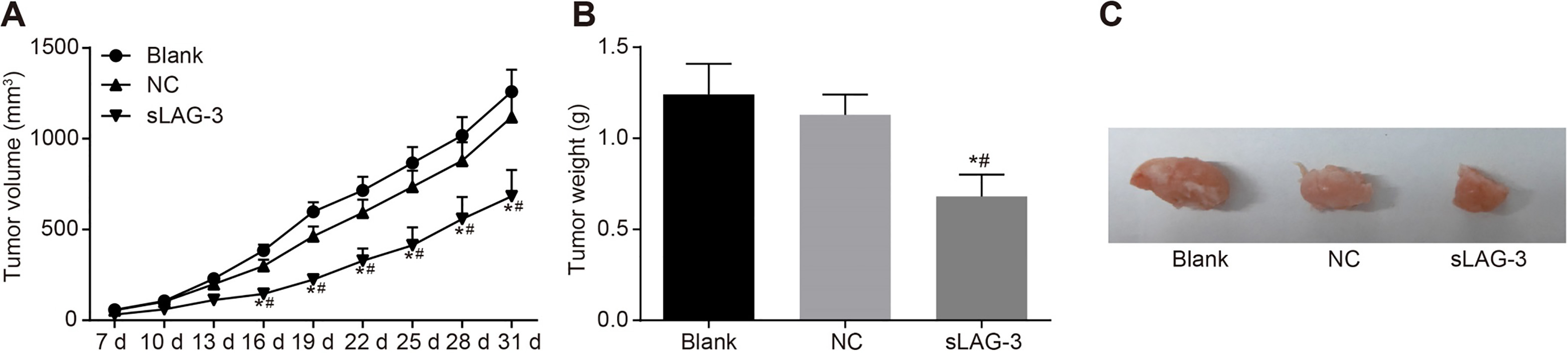
Tumor volume (A), weight (B) and size (C) of mice showed a lower level in the sLAG-3 group than that in the blank and NC groups. NC, negative control; sLAG-3, soluble lymphocyte activation gene-3; , 0.05 compared with the blank group; , 0.05 compared with the NC group.
sLAG-3 is a marker with diagnostic and prognostic value in patients with GC
ROC curve was adopted to identify the expression of serum sLAG-3 and CEA in patients with GC. As illustrated in Fig. 2A, the best boundary value of serum sLAG-3 was 378.330 ng/mL, while the best boundary value of CEA was 21.755 ng/mL. sLAG-3 had an AUC value of 0.907 (the 95% confidence interval (CI) was 0.880–0.934), which was remarkably larger than CEA with the AUC of 0.714 (the 95%CI was 0.673–0.755) ( 0.05). Difference of sensitivity, specificity and accuracy of sLAG-3 and CEA in diagnosis of patients with GC were also analyzed by ROC curve. Compared with CEA, sLAG-3 showed increased sensitivity (88.60% vs 56.20%) and accuracy (90.65% vs 68.61%) in the diagnosis of patients with GC (both 0.05). No statistical difference was found in the specificity between sLAG-3 and CEA in the diagnosis of patients with GC (92.80% vs 81.80%) ( 0.05). These findings indicate that sLAG-3 has a higher diagnostic value in GC. The follow-up of 308 GC patients showed that sLAG-3 is also correlated with the prognosis of GC. According to the ROC curve, the cut-off point for serum sLAG-3 level was 378.33 ng/mL, and then patients were divided into high expression censored group and low expression censored group. Kaplan-Meier survival analysis and Log-rank test were carried out to determine the relationship between sLAG-3 and survival time of GC patients. The results of Kaplan-Meier survival analysis (Fig. 2B) suggested that the overall survival in high expression censored group was longer than that in low expression censored group ( 0.05).
The recombinant sLAG-3 suppresses the growth of GC cells in vivo in mice
The vernier caliper was used to measure the volume of tumor in mice. As shown in Fig. 3, the volume of tumor in the sLAG-3 group was smaller than that in the blank and NC groups ( 0.05). Tumor growth in the sLAG-3 group was inhibited ( 0.05) while no statistical difference was found in the blank and NC groups ( 0.05). What’s more, the weight of tumor was (0.68 0.12) g in the sLAG-3 group, presented a lower level than those in the blank group (1.24 0.17) g and the NC group (1.13 0.11) g (all 0.05). The inhibition rate of tumor was 39.82% in the sLAG-3 group with the NC group as control. In conclusion, the recombinant sLAG-3 could suppress the growth of GC cells in vivo in mice models.
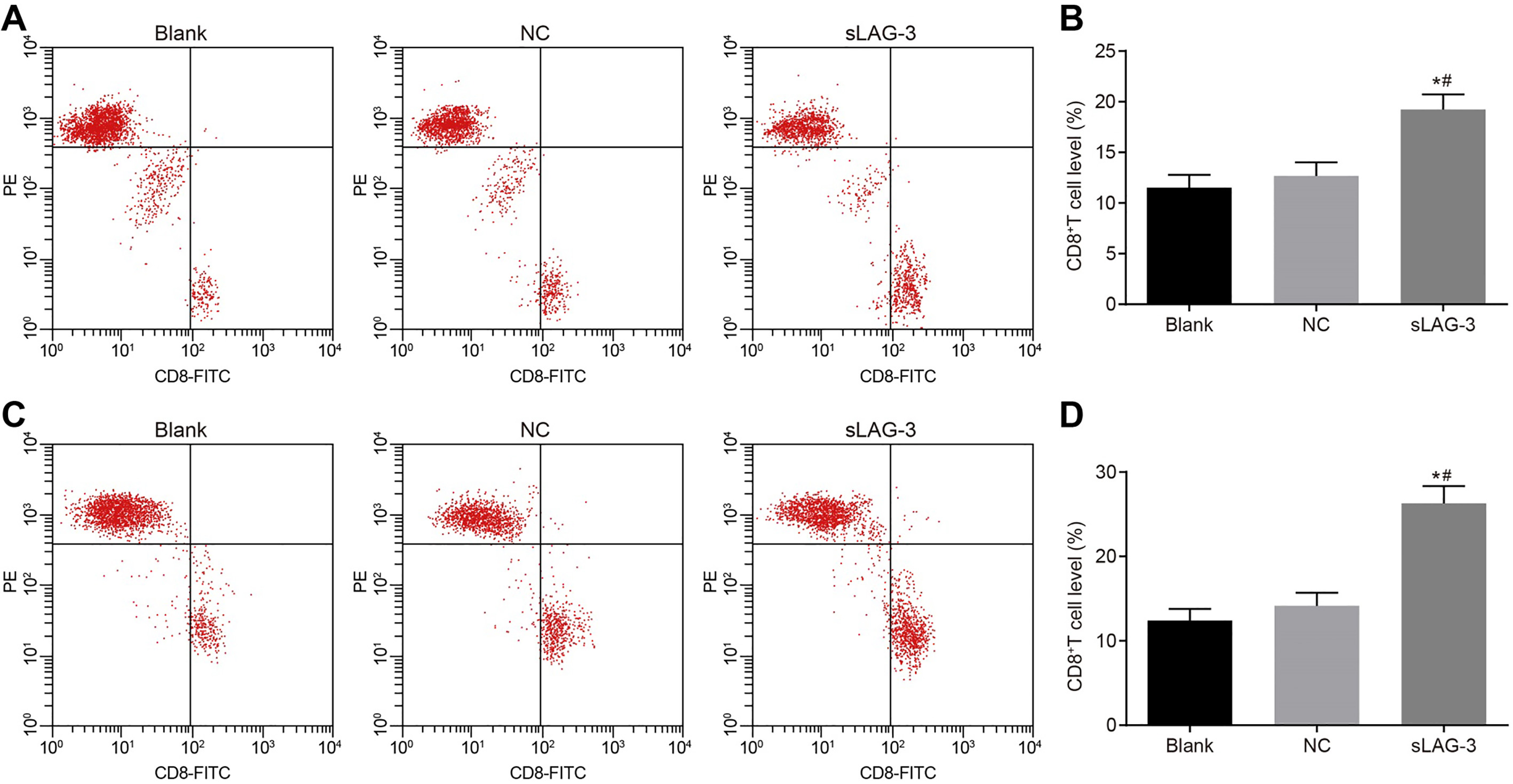
Flow cytometry results demonstrate that sLAG-3 increased CD8T cells in PB and tumor infiltrating area in tumor-bearing mice, thereby promoting specific immune response in GC. A and B: CD8T cell level in PB detected by flow cytometry; C and D: CD8T cell level in tumor-infiltrating area in tumor-bearing mice detected by flow cytometry; NC, negative control; sLAG-3, soluble lymphocyte activation gene-3; , 0.05 compared with the blank group; , 0.05 compared with the NC group.
sLAG-3 increases the number of CD8T cells and promotes specific immune response
Flow cytometry was conducted to verify the CD8T cell level. CD8T cells were detected in both PB (Fig. 4A) and tumor-infiltrating area (Fig. 4B) in tumor-bearing mice. As shown in Fig. 4, the CD8T cell level in PB in the blank, NC and sLAG-3 groups were (11.51 1.28)%, (12.67 1.34)% and (19.24 1.47)%, respectively. The CD8T cell level in tumor-infiltrating area in the blank, NC and sLAG-3 groups were (12.42 1.36)%, (14.16 1.54)% and (26.29 2.05)% respectively. In comparison to the blank and NC groups, the sLAG-3 group had markedly elevated CD8T cell level in PB and tumor infiltrating area (both 0.05), whereas, no significant variance was observed between the blank and NC groups ( 0.05). These results demonstrate that sLAG-3 may increase the expression of CD8T cells in tumor-bearing mice, thus promoting specific immune response.
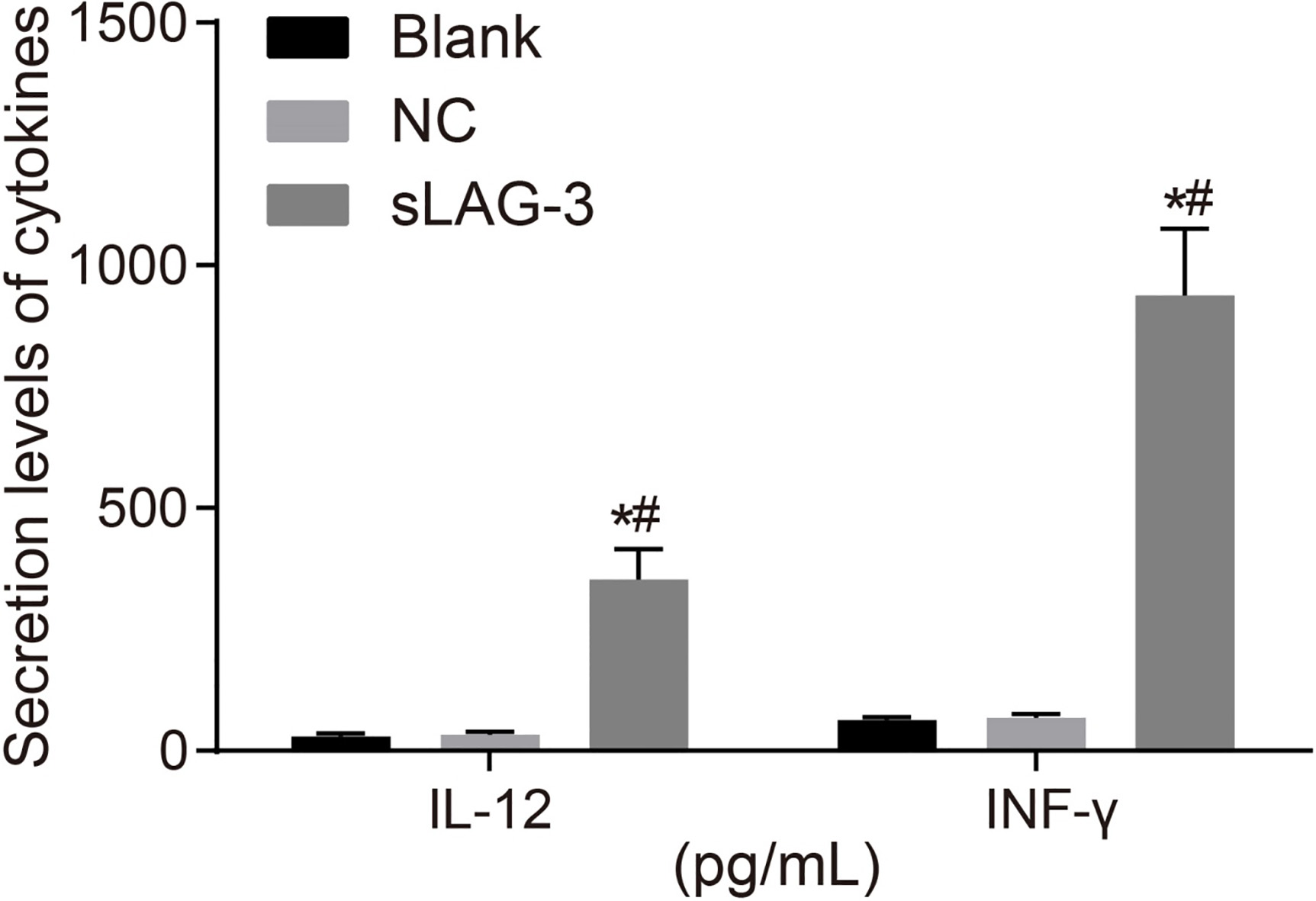
sLAG-3 enhances the secretion levels of IL-12 and INF- in T cells
ELISA was performed to determine the secretion levels of IL-12 and INF- in the supernatant of T cells. The obtained results showed that the secretion levels of IL-12 in the blank, NC and sLAG-3 groups were (29.17 6.26) pg/mL, (32.53 6.44) pg/mL and (352.76 62.41) pg/mL, respectively. The secretion level of IL-12 in the sLAG-3 group exhibited a higher level than that in blank and NC groups (both 0.05), while no statistical difference was found between the blank and NC groups ( 0.05). Meanwhile, the secretion levels of INF- in the blank, NC and sLAG-3 groups were (62.72 7.16) pg/mL, (68.47 7.52) pg/mL and (938.23 137.46) pg/mL, respectively. The secretion level of INF- in the sLAG-3 group presented a higher level than that in blank and NC groups (both 0.05), while no statistical difference was found between the blank and NC groups ( 0.05) (Fig. 5). Taken together, these findings provide evidence that sLAG-3 enhances the secretion levels of IL-12 and INF- in T cells.
ELISA results reveals that sLAG-3 up-regulates secretion levels of IL-12 and INF-. NC, negative control; sLAG-3, soluble lymphocyte activation gene-3; IL-12, interleukin-12; IFN-, interferon-; , 0.05 compared with the blank group; , 0.05 compared with the NC group.
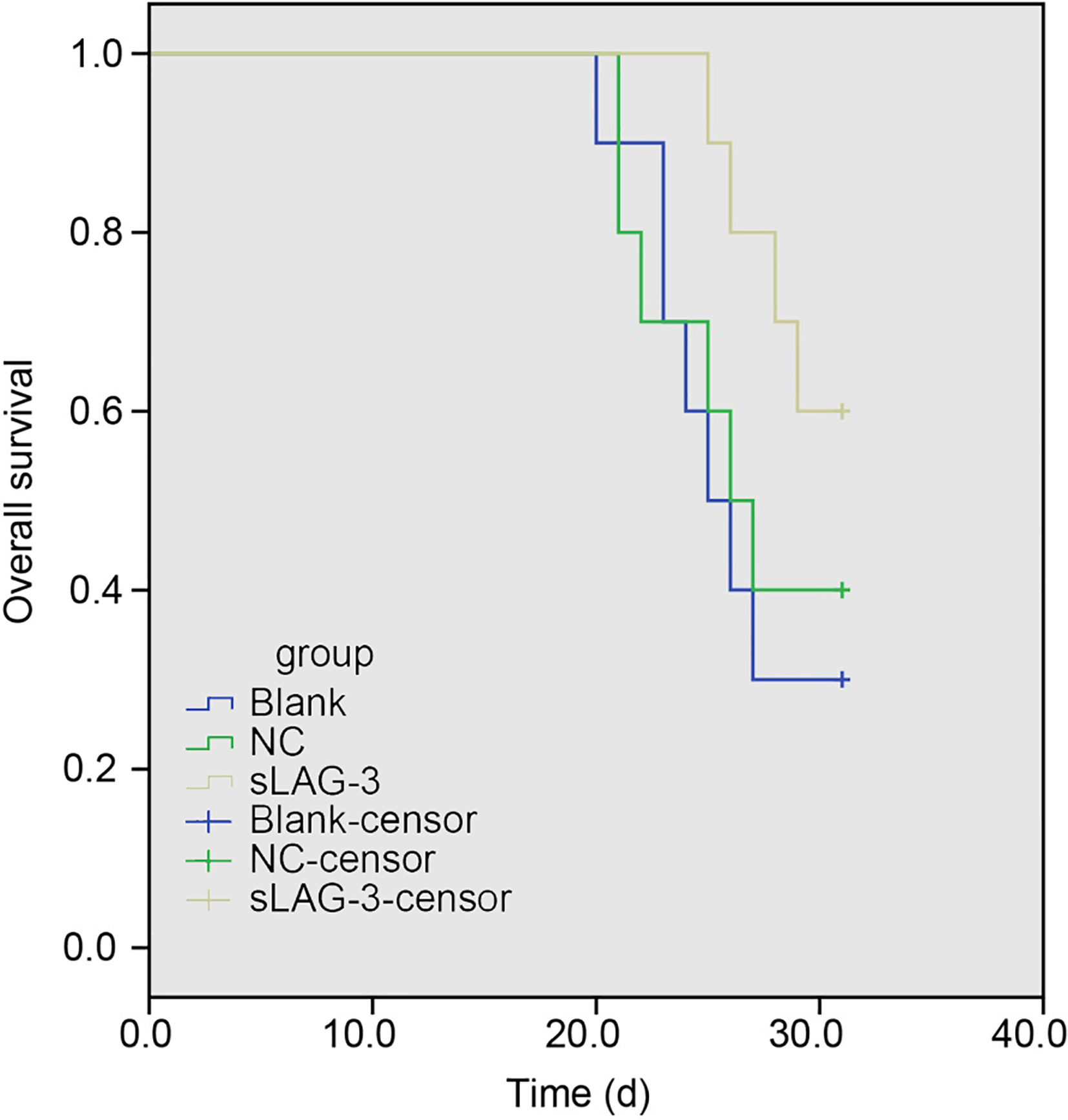
sLAG-3 increases the survival rates of tumor-bearing mice
Log-rank test was utilized to evaluate the survival rates of tumor-bearing mice in the blank, NC and sLAG-3 groups. The overall survival ratio was 26.10 1.16, 26.60 1.28 and 29.40 0.69 in the blank, NC and sLAG-3 groups, respectively. As opposed to the blank and NC groups, the overall survival was up-regulated substantially in the sLAG-3 group (both 0.05). However, no statistical difference was found between the blank and NC groups ( 0.05). At the same time, the survival rates in the blank, NC and sLAG-3 groups were 30%, 40% and 70%, respectively. And the survival rate presented a higher level in the sLAG-3 group than that in the blank and NC groups (both 0.05), while no statistical difference was found between the blank and NC groups ( 0.05) (Fig. 6). It is revealed that sLAG-3 could prolong the overall survival of tumor-bearing mice, thus increasing the survival rates of tumor-bearing mice.
Discussion
GC consists of the cardia and non-cardia types, ranks the second major cause of cancer-related mortality globally [18]. It is estimated that approximately two-thirds of GC deaths and cases occur mostly in less developed countries [19]. It has been revealed that the secretion level of IL-10 induced regulatory T cells might be defined as CD4CD25Foxp3T cells which express both the early growth response gene-2 (EGR2) and LAG3 [11]. The study was performed with the objective to explore the value of LAG3 had in the diagnosis and prognosis of GC and its association with CD8T cells. Of crucial importance, we identified that serum sLAG3 played a key role in GC, serving as a diagnostic and prognostic marker with higher expression, and LAG3 had positive correlation with the CD8T cell frequency and secretion of IL-12 and INF- in peripheral blood.
The study illustrated that sLAG3 had a predictive value in diagnosis and prognosis of GC. A recent study reported by Deng et al. indicated LAG3 to be a prognostic factor for head and neck squamous cell carcinoma independent of tumor size and pathological grades [20]. LAG3 belongs to a member of the Ig superfamily protein and combines with MHC class II followed by high affinity, and is also an effective immune checkpoint suppressor of activated T cells, with immunomodulatory functions [21, 22]. Regulatory T cell-mediated immunosuppression is a symbol of one of the important mechanisms of tumor immune evasion and is a primary restriction for successful treatment of tumor immunotherapy [23]. Deviant immunity could boost tumors, while suitable immune responses may repress or remove tumors through the immunosurveillance system of cancer [24]. LAG3 provides a potential target for cancer immunotherapeutic, acting as a negative regulatory role of T cells and because of its capacity, to mediate exhaustion state binding to PD1 [13]. It has been indicated that LAG-3 could be expressed on specific HIV CD8T cells [9].
Another critical finding of our study was that CD8T cell frequencies in PB and tumor-infiltrating area were regulated by LAG3 in GC. CD8T cells play an important role of immunity to cancer and infection [25]. Previous study demonstrates that cells of GC repress cell metabolism of CD8T through the CD155/TIGIT signaling pathway, which inhibits CD8T cell impaired functions, leading to hypo-responsive antitumor immunity [26]. It has been reported that up-regulation of intratumoral CD8 Foxp3T lymphocytes are related to tumor stage and may affect functions of CD4T cell, which provides a novel insight for developing immunotherapy against GC [27]. Furthermore, CD8CD28 cells are expressed at higher levels in patients with GC, and up-regulation of CD8CD28 cells may lead to immunosuppression induced by tumor [28]. CD8T cell activation played a significant role in the immune response in human papillomavirus 16-infected cervical cancer [29]. This study found that sLAG3 up-regulation increased CD8T cell level in PB and tumor infiltrating area. Thus, we considered sLAG3 overexpression may also promoted immune response by activating CD8T cells. The relationship between LAG3 and CD8T cells has been studied recently. For example, the co-inhibitory molecules of LAG3 and PD1 could work together to restrict CD8T cell signaling and inhibit antitumor immunity in ovarian cancer [14]. Song et al. suggest that 4-1BB-agonist immunotherapy has connection with a lower level expression of the repressed receptors PD-1 and LAG3, which are located on tumor-infiltrating CD8T cells, a molecular phenotype correlated with further tumor growth attenuation [30].
In addition, the present study also illustrated that sLAG3 was positively correlates with the secretion of IL-12 and INF-, and administration of recombinant sLAG3 further facilitated the secretion levels of IL-12 and INF- in T cells. IL-12, an important cytokine in relation to cell-mediated immunity, can directly enhance the functionality of multiple end modulators such as CD4 and CD8 cells [31]. INF- was an important stimulating factor enhancing the immune function of alveolar macrophages in vitro [32]. CD8T cells were believed to have the ability to produce effector cytokines such as INF- [33]. sLAG-3 is beneficial to the restoration of immunogenicity in tumor vaccines and tumor immunity, providing an adjuvant therapeutic target for T cell responses [34]. Similarity, a previous study indicates that sLAG-3 might participate in the regulation of mycobacterium tuberculosis, especially in the immune response of an anti-bacterial [35]. IMP321 is described as a fusion protein of recombinant sLAG-3 Ig, which combines with MHC class II, accompanied with high avidity and regulates antigen presenting cell (APC) and then antigen-experienced memory CD8T cell activation [36]. Meanwhile, antigen-loaded dendritic cell (DC) produces a large number of immune-modulating cytokines, including IL-12 and IL-15, and a high level of co-stimulatory molecule expression are needed to boost CD8T cell effector differentiation and prevent tumor-related suffering [37].
In conclusion, the study shows that sLAG3 is a significant diagnostic and prognostic marker in GC, and it also had positive correlation with the CD8T cell frequency and secretion of IL-12 and INF- in peripheral blood. These findings suggested that sLAG3 might be a potential therapeutic agent for GC implicated with tumor immunity. However, more statistics are necessary to provide some more credible results, and a more specific mechanism of sLAG3 affecting the frequency of CD8T cells in GC is waiting to be discovered.
Footnotes
Acknowledgments
This work was supported by the Scientific Research Innovation Fund of Xinjiang Medical University (XYDCX201561). We would like to acknowledge the helpful comments on this paper received from our reviewers.
Conflict of interest
None.
References
1.
de MartelC.FormanD. and PlummerM., Gastric cancer: epidemiology and risk factors, Gastroenterol Clin North Am42(2) (2013), 219–240.
2.
WaddellT.VerheijM.AllumW.CunninghamD.CervantesA.ArnoldD., O. European Society for Medical, O. European Society of Surgical, R. European Society of and Oncology, Gastric cancer: ESMO-ESSO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up, Eur J Surg Oncol40(5) (2014), 584–591.
3.
WangK.KanJ.YuenS.T. et al., Exome sequencing identifies frequent mutation of ARID1A in molecular subtypes of gastric cancer, Nat Genet43(12) (2011), 1219–1223.
4.
NakamuraR.SaikawaY.TakahashiT.TakeuchiH.AsanumaH.YamadaY. and KitagawaY., Retrospective analysis of prognostic outcome of gastric cancer in young patients, Int J Clin Oncol16(4) (2011), 328–334.
5.
DhallaF.da SilvaS.P.LucasM.TravisS. and ChapelH., Review of gastric cancer risk factors in patients with common variable immunodeficiency disorders, resulting in a proposal for a surveillance programme, Clin Exp Immunol165(1) (2011), 1–7.
6.
A. Japanese Gastric Cancer, Japanese gastric cancer treatment guidelines 2010 (ver. 3), Gastric Cancer14(2) (2011), 113–123.
7.
SunM.XiaR.JinF.XuT.LiuZ.DeW. and LiuX., Downregulated long noncoding RNA MEG3 is associated with poor prognosis and promotes cell proliferation in gastric cancer, Tumour Biol35(2) (2014), 1065–1073.
8.
JeonB.H.ChoiM.LeeJ. and NohS.H., Relationships between gastrointestinal symptoms, uncertainty, and perceived recovery in patients with gastric cancer after gastrectomy, Nurs Health Sci18(1) (2016), 23–29.
9.
PenaJ.JonesN.G.BousheriS.BangsbergD.R. and CaoH., Lymphocyte activation gene-3 expression defines a discrete subset of HIV-specific CD8+T cells that is associated with lower viral load, AIDS Res Hum Retroviruses30(6) (2014), 535–541.
10.
ShapiroM.HerishanuY.KatzB.Z.DezorellaN.SunC.KayS.PolliackA.AviviI.WiestnerA. and PerryC., Lymphocyte activation gene 3: a novel therapeutic target in chronic lymphocytic leukemia, Haematologica102(5) (2017), 874–882.
11.
OkamuraT.FujioK.SumitomoS. and YamamotoK., Roles of LAG3 and EGR2 in regulatory T cells, Ann Rheum Dis71(Suppl 2) (2012), i96–100.
12.
KotaskovaJ.TichyB.TrbusekM.FrancovaH.S.KabathovaJ.MalcikovaJ.DoubekM.BrychtovaY.MayerJ. and PospisilovaS., High expression of lymphocyte-activation gene 3 (LAG3) in chronic lymphocytic leukemia cells is associated with unmutated immunoglobulin variable heavy chain region (IGHV) gene and reduced treatment-free survival, J Mol Diagn12(3) (2010), 328–334.
13.
AndrewsL.P.MarciscanoA.E.DrakeC.G. and VignaliD.A., LAG3 (CD223) as a cancer immunotherapy target, Immunol Rev276(1) (2017), 80–96.
14.
HuangR.Y.EppolitoC.LeleS.ShrikantP.MatsuzakiJ. and OdunsiK., LAG3 and PD1 co-inhibitory molecules collaborate to limit CD8+T cell signaling and dampen antitumor immunity in a murine ovarian cancer model, Oncotarget6(29) (2015), 27359–27377.
15.
TakanoS.SaitoH. and IkeguchiM., An increased number of PD-1+ and Tim-3+ CD8+T cells is involved in immune evasion in gastric cancer, Surg Today46(11) (2016), 1341–1347.
16.
TakayaS.SaitoH. and IkeguchiM., Upregulation of Immune Checkpoint Molecules, PD-1 and LAG-3, on CD4+ and CD8+T Cells after Gastric Cancer Surgery, Yonago Acta Med58(1) (2015), 39–44.
17.
PrigentP.El MirS.DreanoM. and TriebelF., Lymphocyte activation gene-3 induces tumor regression and antitumor immune responses, Eur J Immunol29(12) (1999), 3867–3876.
18.
ShiY.HuZ.WuC. et al., A genome-wide association study identifies new susceptibility loci for non-cardia gastric cancer at 3q13.31 and 5p13.1, Nat Genet43(12) (2011), 1215–1218.
19.
DengH.HuangX.FanJ.WangL.XiaQ.YangX.WangZ. and LiuL., A variant of estrogen receptor-alpha, ER-alpha36 is expressed in human gastric cancer and is highly correlated with lymph node metastasis, Oncol Rep24(1) (2010), 171–176.
20.
DengW.W.MaoL.YuG.T.BuL.L.MaS.R.LiuB.GutkindJ.S.KulkarniA.B.ZhangW.F. and SunZ.J., LAG-3 confers poor prognosis and its blockade reshapes antitumor response in head and neck squamous cell carcinoma, Oncoimmunology5(11) (2016), e1239005.
21.
GoldenD.KolmakovaA.SuraS.VellaA.T.ManichaikulA.WangX.Q.BielinskiS.J.TaylorK.D.ChenY.I.RichS.S. and RodriguezA., Lymphocyte activation gene 3 and coronary artery disease, JCI Insight1(17) (2016), e88628.
22.
PhillipsB.L.MehraS.AhsanM.H.SelmanM.KhaderS.A. and KaushalD., LAG3 expression in active Mycobacterium tuberculosis infections, Am J Pathol185(3) (2015), 820–833.
23.
DengB.ZhuJ.M.WangY.LiuT.T.DingY.B.XiaoW.M.LuG.T.BoP. and ShenX.Z., Intratumor hypoxia promotes immune tolerance by inducing regulatory T cells via TGF-beta1 in gastric cancer, PLoS One8(5) (2013), e63777.
24.
LeeK.HwangH. and NamK.T., Immune response and the tumor microenvironment: how they communicate to regulate gastric cancer, Gut Liver8(2) (2014), 131–139.
25.
van der WindtG.J.EvertsB.ChangC.H.CurtisJ.D.FreitasT.C.AmielE.PearceE.J. and PearceE.L., Mitochondrial respiratory capacity is a critical regulator of CD8+T cell memory development, Immunity36(1) (2012), 68–78.
26.
HeW.ZhangH.HanF. et al., CD155T/TIGIT Signaling Regulates CD8(+) T-cell Metabolism and Promotes Tumor Progression in Human Gastric Cancer, Cancer Res77(22) (2017), 6375–6388.
27.
PengL.S.ZhuangY.ShiY. et al., Increased tumor-infiltrating CD8(+)Foxp3(+) T lymphocytes are associated with tumor progression in human gastric cancer, Cancer Immunol Immunother61(11) (2012), 2183–2192.
28.
ShenY.QuQ.X.ZhuY.B. and ZhangX.G., Analysis of CD8+CD28- T-suppressor cells in gastric cancer patients, J Immunoassay Immunochem33(2) (2012), 149–155.
29.
LiL.MaY.LiuS.ZhangJ. and XuX.Y., Interleukin 10 promotes immune response by increasing the survival of activated CD8(+) T cells in human papillomavirus 16-infected cervical cancer, Tumour Biol (2016).
30.
SongC.SadashivaiahK.FurusawaA.DavilaE.TamadaK. and BanerjeeA., Eomesodermin is required for antitumor immunity mediated by 4-1BB-agonist immunotherapy, Oncoimmunology3(1) (2014), e27680.
31.
KerkarS.P.MuranskiP.KaiserA. et al., Tumor-specific CD8+T cells expressing interleukin-12 eradicate established cancers in lymphodepleted hosts, Cancer Res70(17) (2010), 6725–6734.
32.
ZhouF.BiX.ZhangT. and HuangJ., Study of the antitumor activity of alveolar macrophages after transfected human INF-gamma gene, Zhongguo Fei Ai Za Zhi14(5) (2011), 452–455.
33.
TakataH.NarutoT. and TakiguchiM., Functional heterogeneity of human effector CD8+T cells, Blood119(6) (2012), 1390–1398.
34.
SierroS.RomeroP. and SpeiserD.E., The CD4-like molecule LAG-3, biology and therapeutic applications, Expert Opin Ther Targets15(1) (2011), 91–101.
35.
HeY.RivardC.J.RozeboomL.YuH.EllisonK.KowalewskiA.ZhouC. and HirschF.R., Lymphocyte-activation gene-3, an important immune checkpoint in cancer, Cancer Sci107(9) (2016), 1193–1197.
36.
BrignoneC.GutierrezM.MeftiF.BrainE.JarcauR.CvitkovicF.BousettaN.MedioniJ.GligorovJ.GrygarC.MarcuM. and TriebelF., First-line chemoimmunotherapy in metastatic breast carcinoma: combination of paclitaxel and IMP321 (LAG-3Ig) enhances immune responses and antitumor activity, J Transl Med8 (2010), 71.
37.
JacksonS.R.YuanJ. and TeagueR.M., Targeting CD8+T-cell tolerance for cancer immunotherapy, Immunotherapy6(7) (2014), 833–852.