
Abstract
The aim of present study was to investigate the clinical significances of mannose receptor (MR) and CD163 in colorectal cancer (CRC). Enzyme-linked immunosorbent assay (ELISA) and immunohistochemistry (IHC) were utilized for this analysis. Preoperative serum MR and CD163 levels ranged from 0.153 to 0.804
Introduction
Colorectal cancer (CRC) is the third most frequently diagnosed malignancy among both men and women in the worldwide. In 2017, there are an estimated 135,430 newly diagnosed CRC patients and 50,260 deaths from this disease in the United States [1]. The morbidity and mortality rate of CRC present an increasing trend in China [2]. Five-year survival rate is great than 90% in CRC patients with early stage, whereas it drops to 69.2% and 11.7% for patients with regional spread and distant metastasis, respectively [3]. Indeed, the risk of postoperative recurrence, metastasis, and finally death of CRC patients is closely linked with the TNM stage at the time of first diagnosis. Therefore, early detection and intervention of CRC patients is widely regarded as an efficient way to considerably improve the outcome. Currently, many screening methods are commonly conducted to detect early stage CRC. Fecal occult blood test is an inexpensive and non-invasive screening tool, but it displays low sensitivity and specificity [4]. Colonoscopic examination is considered to be the most sensitive method for early detection of CRC patients. However, high cost, invasiveness and risk during the examination are limited factors for its application as a regular screening method [5]. CEA, CA19-9 and CA72-4 are currently regarded as the most important tumor markers for gastrointestinal cancers. For CRC, these three markers are frequently used for early diagnosis, predicting prognosis and monitoring recurrence after operation [6]. Unfortunately, the sensitivity of these markers for early CRC detection is relatively low. Thus, it is urgent to explore novel tumor markers for CRC.
Mannose receptor (MR), belongs to C-type lectin receptor family, is predominantly expressed in selected populations of macrophages and dendritic cells (DCs). As a phagocytic receptor, MR frequently mediates anti-pathogenic microorganism immunity by recognition of complex glycan structures expressed on the surface of several pathogens, such as bacteria, fungi [7]. Besides, MR expressed on lymphatic endothelium is accepted to participate in the attachment of various cancer cells to lymphatic endothelium and promote further lymphatic metastasis [8]. Presently, soluble mannose receptor has been successfully detected in serum [9]. Serum concentrations of MR are significantly increased in various infectious diseases, sepsis and critical illness [10, 11]. For malignancy, serum MR is elevated in multiple myeloma (MM) patients and identified as a prognostic marker for overall survival [12]. Recently, Liu et al. have been reported that MR is highly expressed in gastric cancer cells and identified as an adverse prognostic factor. They suggested that MR may be a novel molecular marker for gastric cancer [13]. Therefore, these results greatly inspire us to investigate the potential role of MR in patients with CRC. CD163, a hemoglobin scavenger receptor, together with MR, are considered to be macrophage activated markers and described to mediate anti-inflammatory and anti-pathogenic microorganism [14]. CD163 expressed on the surface of cytomembrane frequently experiences proteolytic cleavage after stimulating by inflammatory and then shed into serum as a soluble form [15]. Serum CD163 is elevated in inflammatory and critical diseases [11, 16]. Strikingly, serum CD163 levels are highly elevated in patients with leukemia, multiple myeloma, ovarian and liver cancers and increased expression of them are associated with shorter survival [17, 18, 19, 20]. M2 tumor-associated macrophages are considered to facilitate tumor angiogenesis, progression and metastasis [21]. MR and CD163 are recognized markers of M2 macrophage. Then, expression of MR and CD163 in cancer focus may be imported predictor for aggressiveness and prognosis of cancers [22]. Recently, our team reported preoperative serum MR and CD163 were significantly elevated in gastric cancer patients and identified as unfavorable prognostic markers. The paper has been accepted by magazine of Oncology Letters. As promising gastrointestinal biomarkers, the roles of CD163 and MR in CRC patients are still absence. In this study, we will investigate the potential applications of MR and CD163 in diagnosis as well as assessing prognosis of patients with CRC and expect the outcomes will benefit CRC patients in the future.
Materials and methods
Clinical samples
We recruited 82 patients with colon cancer (CC), 84 patients with rectal cancer (RC), and 87 healthy controls (HCs) from the Jingmen First People’s Hospital between April 2013 and July 2015. All subjects were recruited consecutively. Serum samples were stored at
A total of 73 paraffin-embedded specimens from 35 CC and 38 RC patients who had been underwent surgical treatment with available follow-up information at the Jingmen First People’s Hospital of from April 2013 to July 2015 were recruited in present study. All tumor specimens were previously assessed by two independent pathologists. The median age of CC patients at the time of surgery was 66 (range 40–85) years, with a male: female ratio of 19:16. The median age of RC patients at the time of surgery was 68 (range 47–89) years, with a male: female ratio of 23:15. Basic characteristics of these patients were summarized in Supplemental Table 2. Further, 35 cases of CC and 38 cases of RC paired para-cancerous normal colorectal tissues (more than 2 cm away from the cancer foci) were recruited as controls. Two consecutive sections were obtained from each of the specimens described above and were used for staining of MR and CD163 respectively.
Enzyme-linked immunosorbent assay (ELISA)
Briefly, 96-well microplates were coated with 100
Immunohistochemistry (IHC)
All paraffin-embedded sections in the present study were deparaffinized in xylene and rehydrated in a graded ethanol series. Antigen retrieval was performed by heating the slides in 0.01 M citrate-buffered solution, pH 6.0, in an electric constant temperature drying oven at 60
Preoperative serum MR, CD163, CEA, CA19-9 and CA72-4 concentrations in different groups. Preoperative serum levels of MR (A), CD163 (B) in different group. Correlations of serum levels of MR with CD163 in CC (C) and RC (D) patients. Preoperative serum levels ofCEA (E), CA19-9 (F), CA72-4 (G) in different group. HC 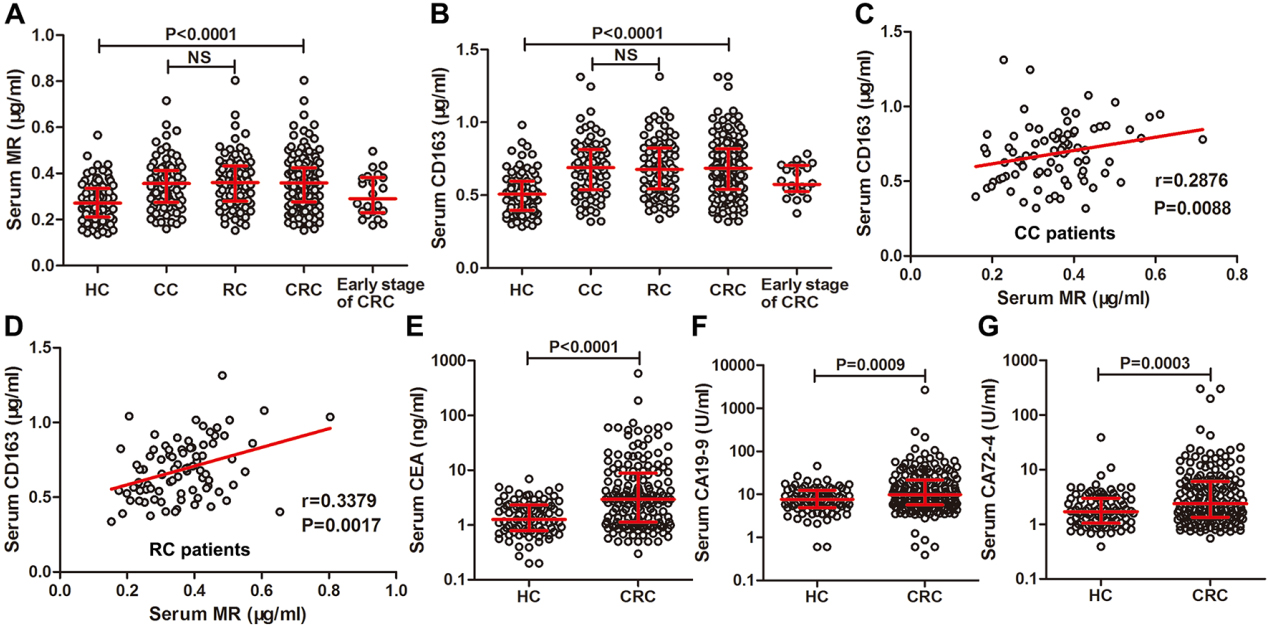
To assess the expression of MR and CD163 in the CRC tissues, three fields were examined on each slide, particularly demarcated areas with distinct brown stai- ning. MR and CD163 immunostaining in CRC and all controls were evaluated by (IOD sum)/Area using the Image Pro Plus (IPP) image analysis software system (Media Cybernetics, Inc. Silver Spring, MD USA). Integrated optical density sum (IOD sum) reflects the protein content of MR or CD163 in the area of interest (AOI), whereas Area represents the area of AOI. The mean density of MR and CD163 were equal to (IOD sum)/Area. The average of the mean density of three fields reflected the intensity of MR and CD163 expression. In brief, the slides were examined and photographed using a microscope with a
Statistical analysis
The non-parametric Mann-Whitney U test was used to determine the statistical significance between the two groups. Receiver operating characteristic (ROC) analysis was performed to evaluate the discriminated values of serum MR and CD163 in CRC patients. The optimal serum cut-offs were calculated using the maximum sum of the sensitivity and specificity. The logistic regression model was used to combine the results from serum MR and CD163 to enhance the accuracy. Correlations of two parameters were evaluated by using the non-parametric Spearman rank correlation coefficient test. Overall survival (OS) was defined as the time from curative surgery to the last follow-up or death of any cause. Survival curves were plotted using the Kaplan-Meier method, and group differences in survival times were assessed by log-rank test. Cox proportional hazards models were used to assess the correlations of clinical variables with survival. A
Diagnostic parameters of serum MR, CD163, CEA, CA19-9 and CA72-4 in detection of colorectal cancer patients
Diagnostic parameters of serum MR, CD163, CEA, CA19-9 and CA72-4 in detection of colorectal cancer patients
Note: AUC, area under curve. Sen, sensitivity. Spe, specificity. Acc, accuracy. PPV, positive predictive value. NPV, negative predictive value. Pos LR, positive likelihood ratio. Neg LR, negative likelihood ratio.
Diagnostic power of preoperative serum levels of MR, CD163, CEA, CA19-9 and CA72-4 for CRC patients. (A) ROC curves for MR, CD163 and the combination of them. (B) Positive rates of MR, CD163 and the combination of them for CRC detection. (C) ROC curves for single of CEA, CA19-9 and CA72-4. (D) ROC curves for combined detection for any two of CEA, CA19-9 and CA72-4. (E) ROC curves for combined detection of MR with CEA, CA19-9 and CA724 respectively. (F) ROC curves for combined detection of CD163 with CEA, CA19-9 and CA724 respectively.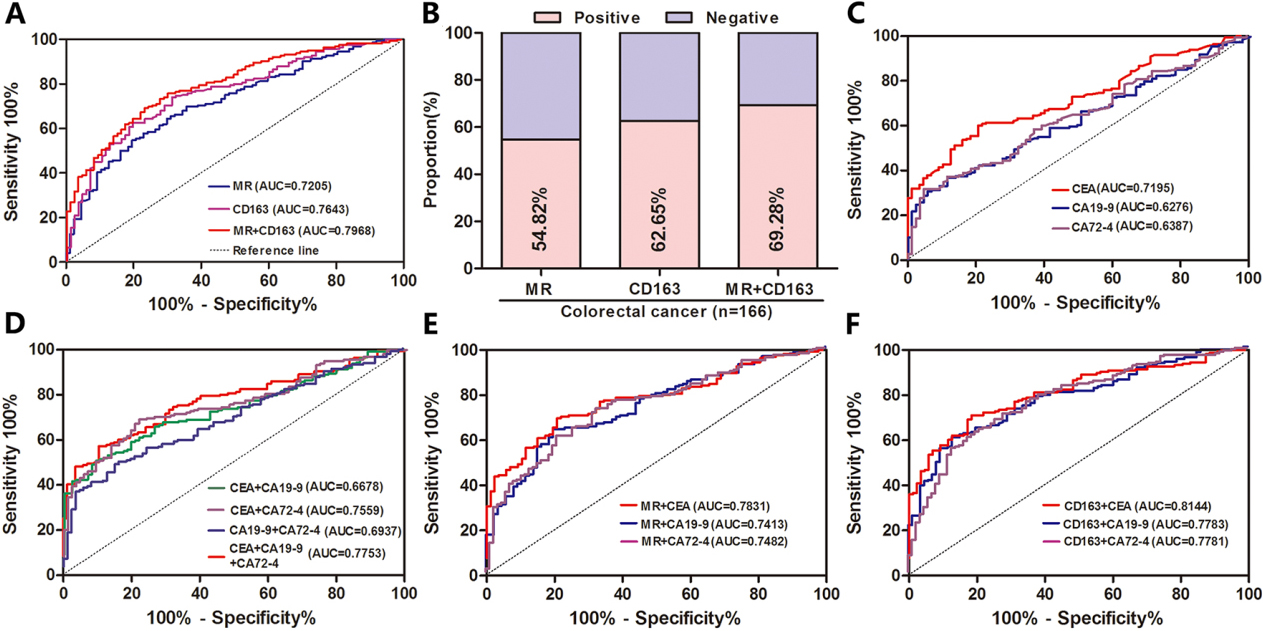
Preoperative serum MR and CD163 levels were significantly elevated in CRC patients than in HCs
Preoperative serum MR levels ranged from 0.160 to 0.716
Preoperative serum MR and CD163 exhibited higher diagnostic value than CEA, CA19-9, and CA72-4 for CRC patients
ROC curves for CRC patients suggested that the optimum cut-offs for serum MR and CD163 were 0.3485
Correlations of serum MR and CD163 levels with CEA, CA19-9, and CA72-4 concentrations in colorectal cancer patients
Correlations of serum MR and CD163 levels with CEA, CA19-9, and CA72-4 concentrations in colorectal cancer patients
Correlations of preoperative serum MR and CD163 levels with major clinical variables in colorectal cancer patients
order to compare the predictive power of serum MR and CD163 with traditional markers in diagnosis of CRC, we then conducted ROC analyses for serum CEA, CA19-9, and CA72-4. For single diagnosis, CEA was apparently superior to CA19-9 and CA72-4 with AUC of 0.7195 (Fig. 2C). The combined detection of CEA and CA72-4 displayed the highest diagnostic power with AUC of 0.7559 than in other kinds of two markers combination, which was similarly lower than the combination of MR and CD163 (Fig. 2D). Further, we investigated diagnostic potential of combination of serum MR and CD163 with traditional markers respectively. Combined detection of MR and CEA with AUC of 0.7831 was superior to the combination of MR with CA19-9 or CA72-4 (Fig. 2E). Similarly, combined detection of CD163 and CEA with AUC of 0.8144 was superior to the combination of CD163 with CA19-9 or CA72-4 (Fig. 2F). As showed in Table 1, combination of MR and CD163, MR and CEA, as well as CD163 and CEA, were associated with better diagnostic parameters (accuracy, PPV and NPV) in CRC prediction.
As shown in Table 2, serum concentrations of MR in CC patients correlated remarkably with CEA and CA19-9 levels (
Univariate and multivariate analyses of various clinical variables in colorectal cancer patients based on OS
Univariate and multivariate analyses of various clinical variables in colorectal cancer patients based on OS
Note: HR, hazard ratio. 95%CI, 95% confidence interval. N, negative. P, positive.
As shown in Table 3, serum levels of MR levels in CRC patients displayed significant correlations with T stage (
High expression of MR and CD163 in serum correlated significantly with shorter overall survival
According to currently established cut-off values for serum MR and CD163, high expression of preoperative serum MR and CD163 displayed obviously shorter OS in CRC patients (
Preoperative serum MR and CD163 were adverse prognostic markers for CRC patients
As shown in Table 4, univariate analysis revealed that differentiation (
Correlations of preoperative serum MR and CD163 levels with OS. Correlations of preoperative serum levels of MR (A), CD163 (B) and their subgroups (C) with OS. Correlations of preoperative serum levels of CEA (D), CA19-9 (E) and CA72-4 (F) with OS.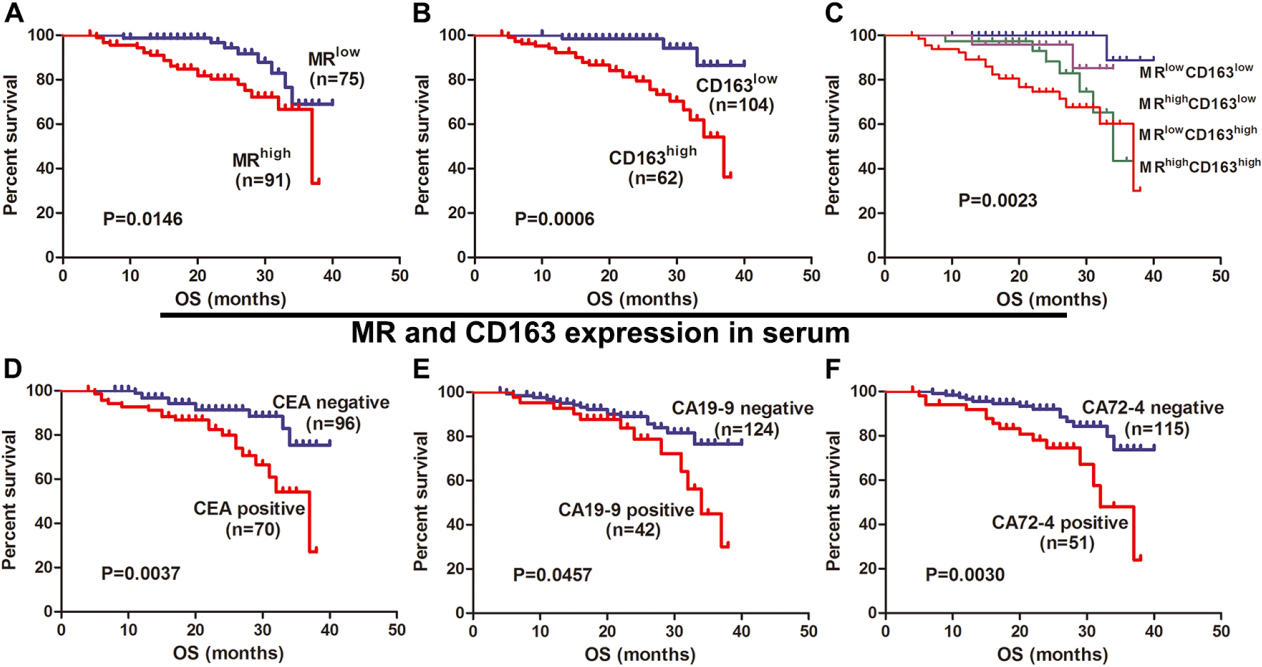
IHC for MR and CD163 staining in CRC and matched para-cancer tissues. IHC for MR staining in tissues of CC (A, E), para-CC (B, F), RC (C, G) and para-RC (D, H). IHC for CD163 staining in tissues of CC (I, M), para-CC (J, N), RC (K, O) and para-RC (L, P).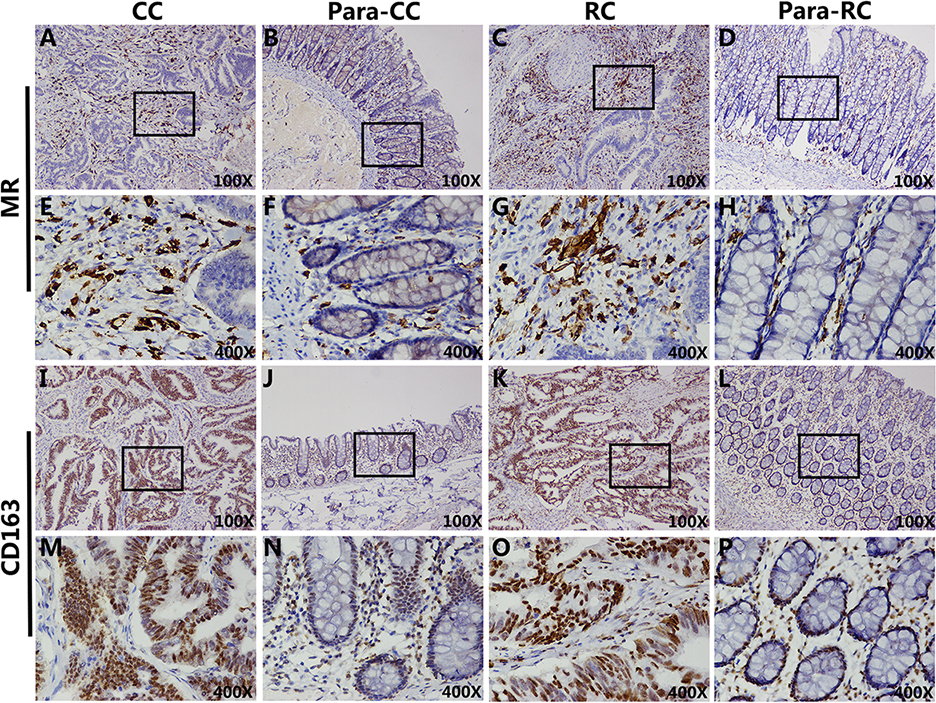
Correlations of MR and CD163 expression in colorectal cancer tissues with major clinical variables
Mean density of MR and CD163 in CRC and matched para-cancer tissues and correlations of MR and CD163 expression in CRC tissues with OS. Mean density of MR in tissues of CRC and matched para-cancer tissues (A). Mean density of CD163 in tissues of CRC and matched para-cancer tissues (B). Correlations of mean density of MR with CD163 in CC (C) and RC (D) tissues. Correlations of expression of MR (E), CD163 (F) and their subgroup (G) in CRC tissues with OS.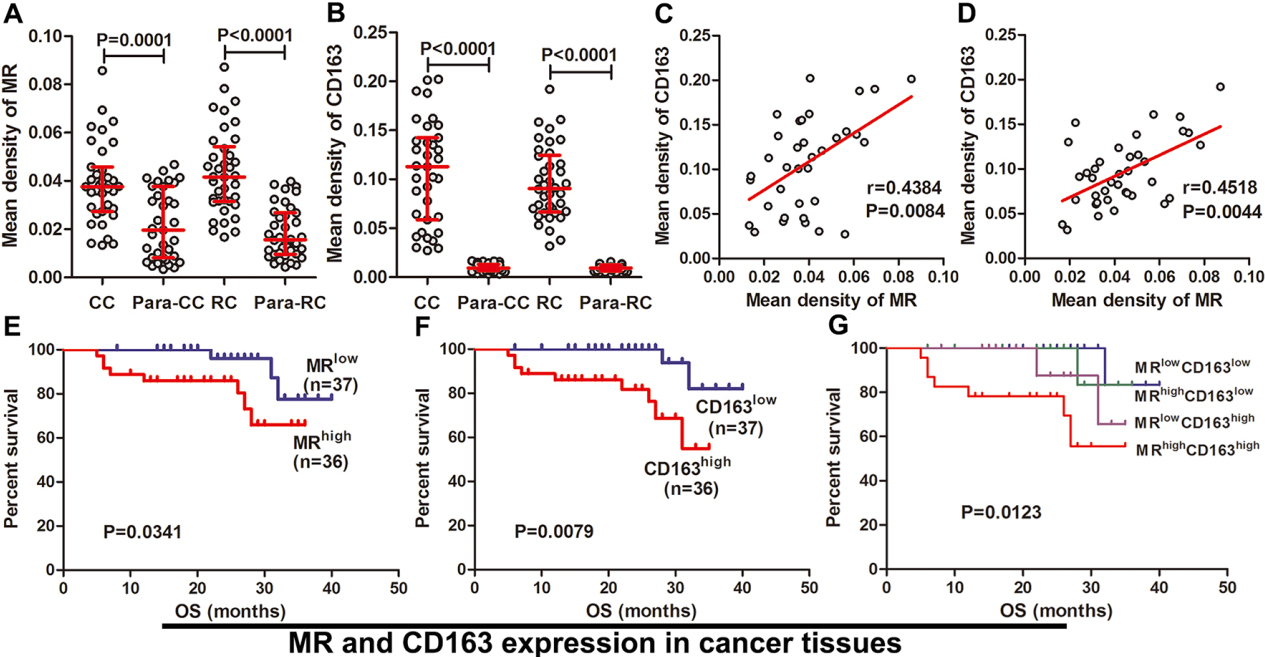
Correlations of MR and CD163 expression in serum and tissues of CRC patients with lymphatic and distant metastasis. Serum levels of MR (A) and CD163 (B) correlated significantly with lymphatic metastasis. Expression of MR (C) and CD163 (D) in CRC tissues correlated significantly with lymphatic metastasis. Serum levels of MR (E) and CD163 (F) were not correlated with distant metastsis. Expression ofMR (G) and CD163 (H) in CRC tissues was not correlated with distant metastasis.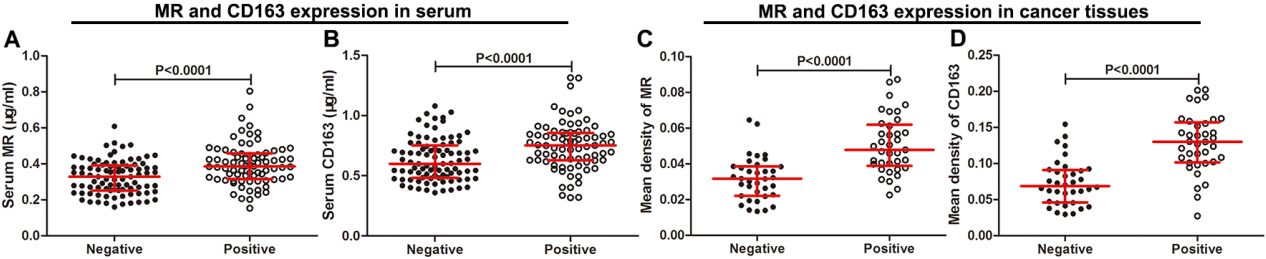
In IHC study, MR staining in CRC and para-cancer tissues was mainly distributed in stroma (Fig. 4A–H). CD163 staining in CRC tissues was distributed mainly in cancer cells and less in tumor stroma (Fig. 4I, K, M and O). CD163 staining in para-cancer tissues was distributed in epithelial cells and stroma (Fig. 4J, L, N and P). Then, mean density of MR in CC and RC tissues was obviously higher than their matched para-cancer tissues (
Expression of MR and CD163 in CRC tissues were associated significantly with major clinical variables, such as N stage, clinical stage
As shown in Table 5, expression of MR in CRC tissues displayed significant correlations with T stage (
High MR and CD163 expression in CRC tissues correlated significantly with shorter overall survival
In present study, the median levels for MR and CD163 expression in CRC tissues were regarded as discriminated values to determine high or low expression. High expression of MR and CD163 in CRC tissues displayed obviously shorter OS (
MR and CD163 may be important facilitators for lymphatic metastasis of CRC
Serum MR and CD163 levels in the lymphatic metastasis cohort were significantly elevated than in the non-lymphatic metastasis cohort (
Discussion
This paper was aimed to explore the clinical significances of MR and CD163 in CRC. Preoperative serum MR and CD163 presented highly diagnostic accuracy for CRC patients, especially when they detected together. High expression of MR and CD163 in serum or cancer tissues of CRC patients correlated significantly with increased risks of lymphatic metastasis and shorter OS. These interesting findings suggest that MR and CD163 may be novel biomarkers for CRC.
In current study, preoperative serum levels of MR and CD163 were elevated in CRC patients. However, the mechanisms of contributing to the increased expression of MR and CD163 in serum of CRC patients are still unknown. Generally, macrophages are considered to participate in inflammatory reaction and immune response and facilitate cancer angiogenesis, aggressiveness and subsequent metastasis. CD163, which is expressed on the surface of macrophage and acted as a specific maker of macrophage activation marker, is frequently up-regulated when it is stimulated by glucocorticoid, interleukin-6 (IL-6), interleukin-10 (IL-10), and macrophage colony-stimulating factor [15]. Inflammatory stimulation, activation of Toll-like receptors and participation of lipopolysaccharide (LPS), metalloprotease and inflammatory medium could corporately contribute to the shedding of CD163 from surface of macrophage into serum as a soluble form [24]. Therefore, serum level of CD163 reasonably represents the degree of inflammatory reaction. The biological behavior of anti-cancer immunity frequently displays certain similarity with anti-inflammation immunity. Thus, we speculate that elevated serum CD163 level in CRC patients may be partially attributed to the activation of macrophage during the process of anti-cancer immunity. Increased serum MR level in CRC patients may undergo the similar shedding mechanism during the process of anti-cancer immunity since MR is co-expression with CD163 on macrophages. Besides, high expression MR and CD163 in CRC tissues may also influence their corresponding serum soluble form.
Then, we evaluated diagnostic value of serum MR and CD163 in CRC patients and compared them with traditional CRC markers. Serum MR, as well as CD163, showed medium diagnostic accuracy with AUC from 0.7 to 0.8. The diagnostic power of serum MR and CD163 in our study was much better than CEA, CA19-9, and CA72-4. Combined detection of multiple tumor markers is an effective way to improve diagnostic accuracy [25]. In our study, combined detection of CD163 with CEA presented the highest diagnostic accuracy than other kinds of two markers combination, including MR and CD163 combination. Therefore, CD163 may be a complementary marker for CEA in CRC detection. Preoperative serum CEA and CA19-9, together with CA72-4, are frequently used for predicting the prognosis of CRC patients who have been underwent surgical treatment. Increased serum levels of these markers indicate high risk of postoperative recurrence and unfavorable survival [26]. Then, similar results were identified in current study. Serum MR and CD163 have been proven to be poor prognostic factors in several cancers, such as gastric cancer, hepatocellular carcinoma and epithelial ovarian cancer [13, 19, 20]. In this study, high levels of serum MR and CD163 in patients with CRC were associated with shorter survival and were identified as adverse prognostic markers for CRC. Meantime, other clinical variables, including TNM stage, CEA, and CA72-4, were proved to be prognostic factors for CRC patients, which was consistent with previously papers [27].
Tumor associated macrophages (TAMs) in tumor microenvironment are commonly classified into M1 and M2 macrophages according to their phenotypic marker. The alternatively activated M2 macrophages are widely accepted to facilitate tumor progression by promoting tumor growth, angiogenesis, invasion, metastasis and the creation of immunosuppressive T-cells [28]. Further, high density of M2 macrophages in cancer stroma is a common phenomenon in several cancers [29]. MR and CD163 are regarded as phenotypic markers which can distinguish M2 macrophages from M1 macrophages. In our study, expression of MR was increased in CRC stroma than in para-cancer tissues and high expression of MR was associated with shorter survival. These findings may suggest high infiltration of M2 TAMs in cancer focus. Similar results were also identified for CD163. Many studies previously reported that high infiltration of M2 macrophages in tumor focus predicted unfavorable prognosis [30]. Therefore, we speculate that high expression of MR and CD163 in CRC tissues represents a certain number of M2 macrophages infiltration and correlates with poor survival.
In this study, increased expression of MR and CD163 in serum or cancer tissues of CRC patients was correlated positively with lymphatic metastasis. It might be assumed that MR and CD163 may be potential targets for lymphatic metastasis of CRC patients. M2 TAMs is shared to promote tumor lymphangiogenesiss, which is the crucial step for tumor lymphatic metastasis [31]. Further, increased infiltration of M2 TAMs has been reported to link with lymphatic and distant metastasis of several solid tumors [32]. Thus, MR and CD163 described as phenotypic markers for M2 TAMs are reasonably correlated with lymphatic metastasis in CRC patients. Although the molecular mechanisms of MR and CD163 mediating lymphatic metastasis of CRC are still unknown, the inspiring findings of our study will encourage us to make further investigation.
In conclusion, our results suggest that MR and CD163 may be novel biomarkers for CRC detection and survival evaluation. Further studies are needed to investigate the molecular mechanisms of MR and CD163 in progression and metastasis of CRC.
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest.