
Abstract
BACKGROUND:
The prognostic value of geriatric nutritional risk index (GNRI) for diffuse large B-cell lymphoma (DLBCL) treated in the rituximab era was not clear.
OBJECTIVE:
To investigate the prognostic impact of GNRI in patients with DLBCL in our hospital.
METHODS:
DLBCL patients were recruited and classified into two groups with and without malnutrition based on GNRI. Clinical features, concentration of T-helper cell type (Th1/Th2/Th17) cytokine profiles and overall survival were compared between these two groups.
RESULTS:
One hundred and five (39%) out of 267 patients were classified into malnutrition group. Patients with malnutrition had lower levels of albumin and hemoglobin, but older age, higher lactate dehydroxygenase (LDH) level, higher frequencies of advanced stage, poor performance status, B symptoms and extranodal involvement, higher scores of NCCN-IPI and higher level of INF-
CONCLUSIONS:
GNRI is not an independent predictor for DLBCL patients.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common subgroup of non-Hodgkin lymphoma (NHL), accounting for 25–35% of all newly diagnosed NHL annually [1]. DLBCL is an aggressive disease with the considerable clinical, pathologic, and molecular heterogeneity [2, 3]. To date, the standard initial treatment for DLBCL patients is the combination of rituximab and chemotherapy with cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP). In addition, the standard tool for prognostication in DLBCL is the international prognostic index (IPI). IPI composed of age, disease stage, extranodal involvement, poor performance status and elevated lactate dehydrogenase. Recently, NCCN-IPI and revised IPI(R-IPI) based on these clinical factors are proved to be more predictive than IPI [4, 5]. Thus, in addition to classic morphology and molecular analyses, the DLBCL diagnosis undoubtedly requires the clinical parameters to stratify R-CHOP-treated patients into prognostically different subgroups. These can be evident by the several reports that pretreatment C-reactive protein, soluble interleukin-2 receptor, lymphocyte-to-monocyte ratio and tumor necrosis have the prognostic value in DLBCL patients [1, 6, 7, 8, 9]. Thus, although clinical parameters have been proposed to improve prognostic stratification for DLBCL patients, additional prognostic factors are still in need.
Altered metabolism is regarded as a hallmark of cancer including DLBCL. An increase of biosynthetic precursors have been consistently observed in cancer cells and tissue [10]. Consequently cancer patients suffered from DLBCL have the propensity of malnutrition in part due to the nutritional supplies to the highly proliferative cancer cells. It is considerable that malnutrition would be associated with adverse outcome. Thus, the impact of malnutrition on DLBCL patients is becoming a research hotspot. To data, many nutritional assessment tools are developed to use as prognostic predictors such as min-nutritional assessment (MNA), subjective global assessment (SGA) and malnutrition universal screening tools (MUST), and so on [11]. However, these assessment tools have obvious limitations such as low specificity, and low predictive values in clinical practice [11]. Intriguingly, a geriatric nutritional risk index (GNRI) is a nutritional assessment tool calculated from serum albumin and the ratio between actual and ideal body weight [12]. GNRI is considered to be time saving and demands little patient involvement. Additionally, it is a prognostic determinant for clinical outcomes in patients with chronic heart failure [13] and those on hemodialysis [14]. Moreover, GNRI is also applied in critically ill cancer patients like gastrointestinal cancer [15]. To our known, there have been no reports of the GNRI in patients with DLBCL. Therefore, we evaluated the prognostic value of GNRI in a large cohort of DLBCL patients, and explored its underlying links to the cytokine profiles.
Materials and methods
In this study, we recruited 267 patients with newly diagnosed DLBCL from 2010 to 2016 in the first affiliated hospital of Zhejiang University. All patients were confirmed by pathological diagnoses, and treated with R-CHOP chemotherapy as follows: rituximab 375 mg/m
Characteristics of patients according to geriatric nutritional risk index
Characteristics of patients according to geriatric nutritional risk index
GNRI; geriatri nutritional risk index, IQR; interquartile range, ECOG-PS; eastern cooperative oncology group performance status, PLT; platelet cell counts, LDH; lactate dehydrogenase, BMI; body mass index, NCCN-IPI; National Comprehensive Cancer Network International Prognostic Index. Extranodal involvement: the bone marrow, CNS, liver/GI tract, spleen, lung and other sites.
Peripheral blood samples were collected at the time of DLBCL diagnosis. The serum was harvested and stored at 4
Statistical analysis
Patient characteristics were summarized using descriptive statistics, which included frequency counts, median, and interquartile range. Categorical variables were compared using Fisher’s exact test or the Chi-squared test and continuous variables using a nonparameter T-test. The main objective of this study was to evaluate the prognostic impacts of GNRI on overall survival (OS) of DLBCL patients. OS was defined as time from the date of diagnosis until death due to any cause or the last follow-up. From the GNRI values, we defined 4 grades of nutrition-related risk based on previously published thresholds: major risk (GNRI
Characteristics of patients with and without malnutrition
In this study, the median of GNRI value was 101, with a range from 68 to 158. The cutoff value of GNRI was defined as 98 according to previously reported studies [17, 18, 19, 20]. Thus, we identified 105 (39%) patients with malnutrition based on GNRI
Overall survival of DLBCL patients. Overall survival of DLBCL patients by the 4 grades of the nutritional-related risk estimated by GNRI (A). 4 grades of nutrition-related risk was based on previously published thresholds [12]: major risk (GNRI 
Because malnutrition might be a reflection of the systemic inflammation in patients with DLBCL [18, 21], 50 matched samples from 267 cases were available to conducted T-helper cell type (Th1/Th2/Th17) cytokine profiles analysis. The characteristics of these patients were summarized in Table S1. Consequently, we found IFN-
T-helper cell type cytokine profiles in DLBCL patients with malnutrition Data are presented as median [interquantile range]
T-helper cell type cytokine profiles in DLBCL patients with malnutrition Data are presented as median [interquantile range]
Multivariate variable analyses for patients with DLBCL
Multivariate variable analyses for patients with DLBCL
NCCN-IPI; National Comprehensive Cancer Network International Prognostic Index.
Overall survival of DLBCL patients with and without nutrition-related risk (no risk: GNRI 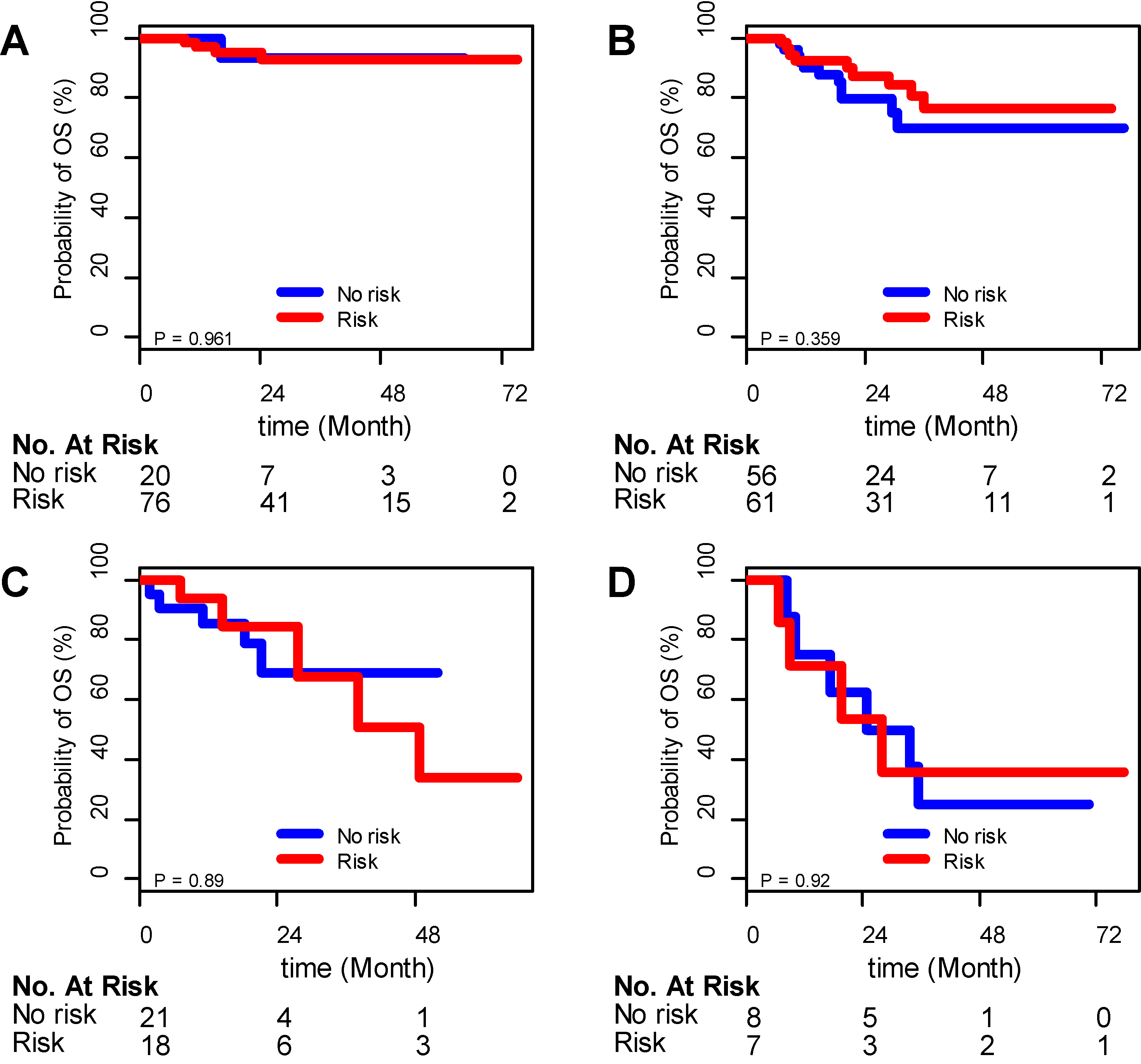
In this study, the 3-year OS rate of 267 patients with DLBCL treated with R-CHOP was 76%. According to previous studies [17, 18, 19, 20], patients can be subdivided into 4 subgroups with distinct grades of nutrition-related risk: no risk subgroup (GNRI
Because NCCN-IPI is the well-established prognostic factor for DLBCL patients treated with rutuximab and the close correlation between GNRI and NCCN-IPI in this study, we had to exclude the confounding effect of NCCN-IPI on the predictive value of malnutrition (GNRI
Similarly, the independent prognostic value of GNRI did not stand in the multivariable analysis after adjusting for NCCN-IPI for overall survival analysis (Table 3). Notably, the variable NCCN-IPI still remained in the multivariate models (Table 3).
Diffuse large B-cell lymphoma (DLBCL) was a group of aggressive disease. Several new tools such as the revised IPI (R-IPI) [4], NCCN-IPI [5], elderly patients IPI (E-IPI) can be used as the prognostic factors for patients with the standard R-CHOP treatment. Other than these prognostic markers, numerous novel markers like clinical parameters could be used as a simple and promising tool to risk stratification in DLBCL patients treated with R-CHOP [19]. GNRI calculated by the clinical parameters like albumin, body weight and high are now reported as a useful predictor in solid tumor [15]. However, the prognostic significance in DLBCL patients was unclear. Here, we found that GNRI was closely associated with NCCN-IPI, and did not have an independent prognostic value on overall survival in DLBCL patients.
It is important to assess the nutritional status for patients with hemotological disorder in clinical practice [11]. Therefore, we focused on the prognostic value of GNRI on overall survival for DLBCL patients. As previously reported, GNRI less than 98 was regarded as malnutrition status in elderly patients. In general, DLBCL occurred more often in elderly patients. The mean age of patients in these study was 55 years with the interquantile from 49 to 65 years. The major aims of our study was to investigate whether GNRI might be a useful tool to assess the nutritional status in our DLBCL patients. We classified patients into four groups based on the 4 grades of nutritional risk estimated by GNRI. We found GNRI as a four categorical variable can be used as the prognostic predictor in our patients cohort. Next, we refined patients into two group with and without malnutrition. We found patients with malnutrition had the adverse overall survival. These results suggested malnutrition measuring by GNRI might be used as a biomarker for advanced lymphoma.
In order to evaluate the independent prognostic value of GNRI, we must exclude the potential confounders. Therefore, we compared the well-established prognostic factors between patients with and without malnutrition. Interestingly, we found patients with malnutrition had lower levels of albumin, hemoglobin and body mass index, but older age, advanced clinical stages, elevated LDH level, high score of ECOG performance status and more extranodal involvement as well as high score of NCCN-IPI. Notably, advanced lymphoma often complicates with hemophagocytic lymphohistiocytosis (HLH). HLH is characterized by excessive immune activation and cytokine release. Indeed, malnutrition can disturb T cells to produce the inflammatory cytokines [22]. Thus, cytokine factors must have played an important role in malnutrition of DLBCL patients. As expected, we found IFN-
The present study had several limitations. First, our study are limited by the retrospective study design. Second, our sample sizes are not enough large, more large-scale and well-design studies with both clinical and molecule biomarkers are warranted to better clarify the prognostic value of GNRI in DLBCL treated in rituximab era.
Taken together, we found malnutrition measuring by GNRI was closely associated with NCCN-IPI, and GNRI was not an independent predictor for overall survival in DLBCL patients.
Footnotes
Acknowledgments
This work was supported by National Natural Science Foundation of China (Grant # 81370643, 814703 05, 81670124).
Conflict of interest
The authors report no conflicts of interest.
Supplementary data
Characteristics of paired patients for cytokines analyses GNRI; geriatric nutritional risk index, IQR; interquartile range, ECOG-PS; eastern cooperative oncology group performance status, LDH; lactate dehydrogenase, NCCN-IPI; National Comprehensive Cancer Network International Prognostic Index. LDH ratio was calculated using LDH divided by the upper limit of normal.
Variables
GNRI
GNRI
P value
Number
25
25
Sex, male, %
12 (48.0)
9 (36.0)
0.567
Age, years
60.00 [49.00, 69.00]
58.00 [53.00, 68.00]
0.869
ECOG-PS
7 (28.0)
4 (16.0)
0.496
Ann Arbor Stage III-IV, n (%)
17 (68.0)
16 (64.0)
1.000
B symptoms, n (%)
12 (48.0)
7 (28.0)
0.244
Extranodal involvement,
13 (52.0)
6 (24.0)
0.079
LDH ratio
0.196
10 (40.0)
15 (60.0)
1–3
10 (40.0)
9 (36.0)
5 (20.0)
1 (4.0)
NCCN-IPI, n (%)
0.229
Low
2 (8.0)
4 (16.0)
Low intermediate
12 (48.0)
14 (56.0)
High intermediate
5 (20.0)
6 (24.0)
High
6 (24.0)
1 (4.0)
Univariate analysis for overall survival GNRI; geriatric nutritional risk index, HR; hazard ratio, CI;confidence interval, ECOG-PS; eastern cooperative oncology group performance status, LDH; lactate dehydrogenase, NCCN-IPI; National Comprehensive Cancer Network International Prognostic Index.
Variables
P values
HR (95% CI)
GNRI
0.041
0.542 (0.301,0.975)
Sex
0.053
1.888 (0.99,3.599)
Age
0.042
1.84 (1.024,3.307)
ECOG-PS
0.001
3.682 (2.035,6.662)
LDH
0.001
3.225 (2.083,4.995)
Hemoglobin
0.003
2.426 (1.352,4.355)
Ann Arbor Stage III-IV
0.001
4.885 (2.065,11.557)
Extranodal disease
0.216
1.519 (0.783,2.944)
Hemoglobin
0.039
0.987 (0.974,0.999)
NCCN-IPI
Low intermediate vs. Low
0.014
3.416 (1.282,9.102)
High intermediate vs. Low
6.77 (2.306,19.876)
High vs. Low
13.099 (4.475,38.344)