
Abstract
BACKGROUND:
Ovarian cancer is frequently diagnosed at an advanced stage and 70% of patients experience recurrence months to years from initial diagnosis. The expression of paraneoplastic antigens can result in the occurrence of onconeural autoantibodies in ovarian cancer that may be associated with neurological disorders that are clinically manifested in patients before diagnosis of ovarian cancer. These paraneoplastic antigens can serve as excellent biomarkers not only for early detection but also for monitoring ovarian cancer recurrence.
OBJECTIVE:
To assess the immunoreactivity of our previous 3 biomarkers along with 3 paraneoplastic antigens, HARS, Ro52 and CDR2 for the evaluation of their sensitivity in predicting recurrence before the clinical relapse of the ovarian cancer.
METHODS:
Western blot immunoassays were performed to assess the immunoreactivity of 6 antigens with 21 recurrent ovarian cancer patients.
RESULTS:
The results indicated that antibodies to HARS, Ro52, CDR2 and 5H6 antigens predicted ovarian cancer recurrence 5.03 months before the clinical or symptomatic relapse in 21 ovarian cancer patients with a sensitivity of 90.5% when CA125 levels were below the standard cutoff (35 U/ml).
CONCLUSION:
Our study suggests that appearance of onconeural antibodies prior to the rise in CA125 during post treatment surveillance can be a useful diagnostic to predict ovarian cancer recurrence.
Keywords
Introduction
Routine disease monitoring of ovarian cancer patients is generally recommended by gynecologic oncologists after the completion of primary surgery and first-line chemotherapeutic treatments. The clinical symptoms of recurrence are determined by measuring the level of serum CA125, one of the most extensively used tumor biomarkers in standard clinical practice for disease surveillance. In a randomized trial performed by Rustin et al. it was shown that ovarian cancer patients who had increased CA125 level before the clinical recurrence followed by chemotherapy treatments did not have a survival benefit compared to the other arm of ovarian cancer patients who received chemotherapy based on clinical evidences of ovarian cancer recurrence [25]. Conversely, a recent study has shown that ovarian cancer patients at risk of recurrence may benefit from early initiation of treatments. Guo and Peng reported that when setting the CA125 threshold to 10 U/ml instead of 35 U/ml, distant recurrent lesions located in spleen, liver and pelvic region were detected in 3 postoperative epithelial ovarian carcinoma patients who had CA125 values 14.5 U/ml, 13.5 U/ml and 20.9 U/ml respectively. In all of these patients, recurrent lesions were detected 2–3 months prior to clinical recurrence and all the patients underwent second cytoreductive surgery. After the surgery, their CA125 values were less than 10 U/ml and the patients were in good health. Thus, early treatments were shown to be necessary when there is a risk of recurrence involved [14]. Their study may not be in agreement with the randomized trial by Rustin et al. where only chemotherapy was considered as an early treatment and the impact of second-line cytoreductive surgery was not taken into consideration [25]. Also, patients who participated in that trial were not treated with new salvage chemotherapy regimens that might have improved prognosis [13, 22]. Another study reported by Yang et al. showed that in a study population of 152 ovarian cancer patients, the average elevation of CA125 level was 116.28 U/ml at the time of clinical recurrence and the average time that elapsed from the rise in CA125 to the time when recurrent lesions were detected by physical or radiologic examinations was 122 days. The sensitivity and specificity of detecting early ovarian cancer recurrence using CA125 tumor marker alone with a threshold of 35 U/ml was 67.39% and 86.79% respectively [28]. Despite its utility in ovarian cancer diagnosis and disease monitoring, CA125 has its limitations. A rise in CA125 to 1,000 IU/ml has been observed in many benign gynecological conditions, such as, intramural leiomyoma, adenexal cystic mass, and ovarian endometrioma [12]. Other studies have documented normalization of CA125 in 50% of patients with ovarian cancer with microscopic disease at the second-look laparotomy [4]. Therefore, there is a dearth of sensitive biomarkers that can predict ovarian cancer recurrence with a sufficient lead time prior to the rise in CA125 during cancer surveillance, so that the patients can benefit from an early therapeutic intervention capable of prolonging the disease-free interval and improve overall survival.
Numerous studies have shown the role of tumor autoantibodies as biomarkers for ovarian cancer diagnosis and its recurrence. These autoantibodies to tumor associated antigens (TAAs) arise due to the generation of humoral immune response before evidence of clinical symptoms in cancer patients [5, 7, 8]. Our previous study indicated that a 3 biomarker panel, one being a peptide epitope from a known paraneoplastic antigen, predicted ovarian cancer recurrence at a median lead time of 9.07 months with 94.7% sensitivity, 86.7% specificity, and 93.3% accuracy, in a cohort of ovarian cancer patients where normalization of CA125 had occurred after the surgery and completion of chemotherapy [5]. Paraneoplastic antigens can elicit a humoral immune response in cancer patients as these antigens are expressed in the cells of nervous system and tumor [24]. The appearance of these onconeural antibodies in ovarian cancer patients leads to the development of various neurological disorders called paraneoplastic syndromes, particularly dermatomyositis or polymyositis [1, 2, 15, 21]. The diagnosis of ovarian cancer can be preceded by the occurrence of dermatomyositis or polymyositis. Marie et al. reviewed the medical data to evaluate the clinical outcome of 89 patients who had antisynthetase syndrome (ASS) associated with Jo-1 antibodies that target HARS antigen. Concurrent occurrence of Ro52 antibodies was also observed in 36 out of 89 patients. It was reported that 7/36 (19.4%) had colon, breast, ovarian, or esophageal cancers and 28/36 (77%) had interstitial lung disease with poorer prognosis [17]. Other studies have shown that patients with ovarian cancer in association with paraneoplastic cerebellar degeneration harbor Yo antibodies directed against CDR2 antigen that is expressed in tumor cells and Purkinje cells [21]. The frequency of appearance of Yo antibodies in patients with paraneoplastic cerebellar degeneration associated with ovarian cancer and breast cancer was found to be 13/557 (2.3%) and 4/253 (1.6%) respectively. The diagnosis of 2/13 ovarian cancer patients was preceded by the appearance of paraneoplastic cerebellar degeneration [21]. These onconeural antibodies can occur in the absence of paraneoplastic symptoms leading to their diagnostic utility in asymptomatic subjects. Although the clinical implication of these onconeural antibodies as biomarkers for early diagnosis of ovarian cancer has been reported in many case studies, the usefulness of these antibodies has yet to be evaluated in monitoring disease status in ovarian cancer patients after cytoreductive surgery and chemotherapy treatments. In the present study we evaluated the role of a panel of 3 recombinant paraneoplastic antigens, HARS, CDR2 and Ro52 in combination with 3 of our previous biomarkers in predicting recurrence in new and independent cohort of ovarian cancer patient population in which most of the patients had no elevation in CA125 level months before their clinical recurrence. Our results indicate that autoantibodies to HARS, Ro52, CDR2 and 5H6 antigens predicted ovarian cancer recurrence 5.03 months before the clinical or symptomatic relapse in 21 ovarian cancer patients with a sensitivity of 90.5% when CA125 levels were below the standard cutoff (35 U/ml).
Materials and methods
Patient population
Patients diagnosed and treated for late stage serous epithelial ovarian cancer at Karmanos Cancer Institute, St John Health System (Detroit, MI), or Oakwood Hospital (Dearborn, MI) were entered on to the study at the time of their diagnosis. Study participation included collection of serial blood samples starting at or near the time of surgery and continuing for every six months up to five years, concurrent with clinical lab draws. Medical records were reviewed to determine CA125 levels, disease status, chemotherapy status, disease-free interval (DFI) and time to recurrence (TTR) over a multi-year period. Serial serum samples were collected between 2003 and 2014. All participants provided written informed consent. Study procedures were approved by the Wayne State University, St. Johns Health Systems, and Oakwood Hospital Institutional Review Boards.
Specimen collection and processing
Samples were collected and processed using the procedure as described earlier [5]. The demographics of patients in the training set were also described in earlier studies [5]. For each patient in the test set we selected 3 samples; 1) the baseline blood sample (collected at time of diagnosis), 2) the blood sample collected approximately 3–15 months before the clinical recurrence, ideally with normal CA125 and no evidence of disease, and 3) the sample collected as close as possible to clinical recurrence (Supplementary Table S2). The disease status of 3 sequential serum samples correlated to EOD-NED-EOD but the second sample was usually taken while still in chemo so the NED was not actually a true remission, but a response to the chemotherapy. EODs were determined by clinical/imaging data, or elevated CA125 level, or both. Future studies will include more frequent collection of interval samples to increase the pool of samples fitting the ideal profile.
Cloning of recombinant antigen into bacterial expression vector
All the previous phage bearing tumor antigens such as 4B7, 4H4, 5H6, and T7 1-2a (empty phage capsid protein used as negative control protein) as well as 2 paraneoplastic antigens such as Ro52 and CDR2 were first PCR amplified using different forward primers (containing 5’ restriction site followed by His tag and T7 tag at the N terminus) and reverse primers (containing 3’ stop codon followed by restriction site at the C terminus) using cDNA templates (Supplementary Table S1). For phage antigens, the cDNA templates were obtained from ovarian tumor T7 phage cDNA libraries and for paraneoplastic antigens, cDNAs were prepared from different ovarian cancer cell lines. The PCR products were column purified (Qiagen, Germantown, MD), restriction digested, column purified again and successively ligated to pET-21b bacterial expression vector by following manufacturer’s protocol (EMD Millipore Corporation, San Diego, CA). The ligated DNA was then transformed into BL21-DE3 strain and several colonies were picked and sequenced. Positive colonies bearing the respective genes were further employed for in vivo production of recombinant His and T7-tagged proteins in Bl21-DE3 bacterial strain. All cDNA clones were DNA sequence verified by standard techniques.
Production and purification of recombinant His and T7 tagged proteins
BL21-DE3 bacterial cells bearing clones, pET21b-4B7, pET21b-4H4, pET21b-5H6, pET21b-Ro52, pET21b-CDR2, and pET21b-T71-2a (negative control) were grown overnight in 10 ml LB with 50
Immunoscreening of ovarian cancer patient serum samples using purified recombinant antigens
For the purified recombinant Ro52 antigen, 0.06
Determination of threshold of each antigen using the training set
Threshold of each antigen was calculated based on the immunoreactivity of T71-2a protein (negative control) with the all the ovarian cancer patients (5 recurrent and 5 non-recurrent) in the training set. The median (Median T71-2a) and standard deviation (STDEV) of the normalized signal intensity values representing the immunoreactivity of T71-2a protein with 5 recurrent patients (serum samples were obtained at months to 1 year before the clinical recurrence) and the 5 non-recurrent patients (serum samples were obtained at approximately 1 year from ovarian cancer diagnosis) in the training set was calculated as shown as Table 1. The threshold for each antigen was chosen in such a way to achieve higher percent specificity against 5 non-recurrent ovarian cancer patients in the training set as shown in Table 1 that also listed the sensitivity of each antigen that reacted with 5 recurrent ovarian cancer patients. For moderate to weakly reactive antigens such as HARS, 4B7, 4H4, 5H6, a threshold of 0.03 (Median T71-2a
Determination of threshold of an antigen that discriminated recurrent ovarian cancer patients (serum was drawn close to 1 year before clinical recurrence) from non-recurrent ovarian cancer patients (serum was drawn close to 1 year after diagnosis) in the training set
Determination of threshold of an antigen that discriminated recurrent ovarian cancer patients (serum was drawn close to 1 year before clinical recurrence) from non-recurrent ovarian cancer patients (serum was drawn close to 1 year after diagnosis) in the training set
Note: Calculation of threshold for each antigen: Normalized signal intensity value was calculated by dividing the background corrected signal intensity obtained with patient’s serum by background corrected signal intensity obtained from His-tag antibody. Median of normalized signal intensity value of T7 1-2a (negative control) with 5 recurrent and 5 non-recurrent ovarian cancer patients in the training set was 0.010. Standard Deviation (STDEV) of the normalized signal intensity value of T7 1-2a (negative control) with 5 recurrent and 5 non-recurrent ovarian cancer patients in the training set was 0.0173. Please note that the threshold values were adjusted to 2 places of decimal in excel worksheet (data not shown). Threshold for HARS, 4B7, 4H4, 5H6: (Median T7 1-2a
Our goal is to predict recurrence prior to the biochemical (CA125 level) or clinical/radiologic evidence of recurrence so that re-initiation of therapy can maximize the chances of improving overall survival in ovarian cancer patients. To this end we have been utilizing tumor autoantibody biomarkers in ovarian cancer patients diagnosed with late stage serous adenocarcinoma. After subtractive biopanning with sera from ovarian cancer patients and healthy controls we employed protein microarrays using phage lysates of single phage bearing cDNA clone to identify cDNA clones of antigens that specifically reacted with sera from ovarian cancer patients [7]. We found that these clones were good biomarkers for both early detection [7] and recurrence [5] of ovarian cancer. In addition, the antigen clones were frequently homologous to known paraneoplastic antigens and we propose that autoantibodies to these paraneoplastic antigens occur in asymptomatic cancer patients and can be used for diagnostic purposes. After cloning, bacterial expression and purification of the most informative antigen biomarkers, we performed a serological immunoscreening using western blotting to evaluate the sensitivity of these recombinant proteins to predict recurrence prior to the rise in CA125 level (cutoff 35 U/ml) or radiologic indication of clinical recurrence in an independent retrospective cohort of ovarian cancer study population.
Serological screening of ovarian cancer patients using recombinant protein biomarkers
To determine the threshold of immunoreactivity of each antigen we performed an initial immunoscreening with 5 recurrent and 5 non-recurrent ovarian cancer patients (training set) using 6 biomarkers, namely HARS, 4B7, 4H4, 5H6, Ro52, CDR2, and T7 1-2a (which served as a negative control protein) as described in Materials and Methods section (see reference 5 for patients’ demographics used in the training set) [5], (Table 1). The threshold for each antigen was next applied to evaluate the immunoreactivity of antigens with serum IgGs obtained from 21 ovarian cancer patients at 3 different time points, initially at the time of diagnosis (T1) when the patients had elevated CA125 levels, during the monitoring phase approximately 3–15 months before their clinical recurrence (T2) when most of the patients had their CA125 values within the normal range (
Association of immunoreactivity of antigens with recurrence status of ovarian cancer patients having stable disease during monitoring phase
We observed that immunoreactivity of Ro52, CDR2 and HARS antigens was most strongly associated with the recurrence status of 3/5, 3/5 and 4/5 ovarian
Association of immunoreactivity of Ro52, CDR2 and HARS antigens with the recurrence status of 21 ovarian cancer patients
Association of immunoreactivity of Ro52, CDR2 and HARS antigens with the recurrence status of 21 ovarian cancer patients
Note: Ovarian cancer patients with asterisk had evidence of disease months before the clinical recurrence ; NED: No evidence of disease; EOD: Evidence of disease. T1 represents time at ovarian cancer diagnosis; T2 represents time in months before the clinical recurrence.
Association of immunoreactivity of 4B7, 4H4, and 5H6 antigens with the recurrence status of 21 ovarian cancer patients
Note: Ovarian cancer patients with asterisk had evidence of disease months before the clinical recurrence ; NED: No evidence of disease; EOD: Evidence of disease. T1 represents time at ovarian cancer diagnosis; T2 represents time in months before the clinical recurrence.
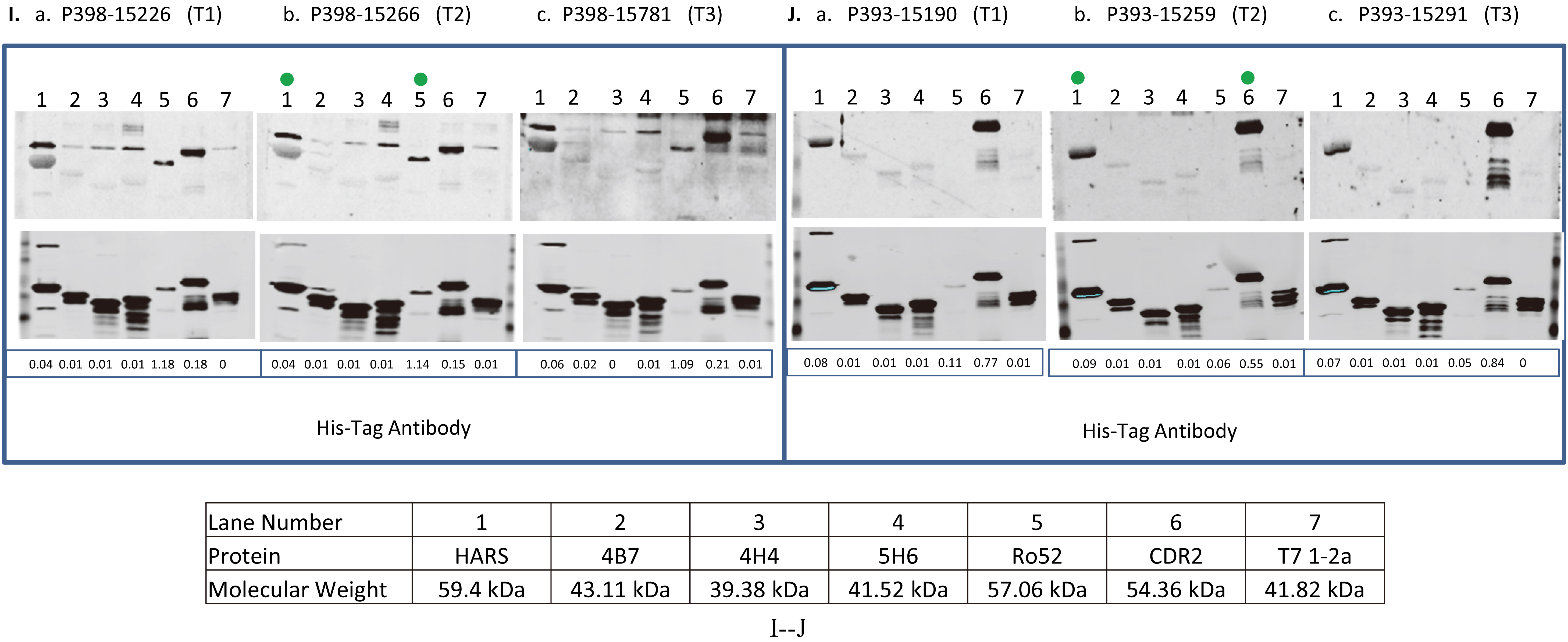
The reactivity of antigens with serum samples obtained from ovarian cancer patients at 3 different time points and women with other benign diseases and healthy women. BL21-DE3 bacterial cells bearing individual antigen clone were grown and cell lysate was prepared. One 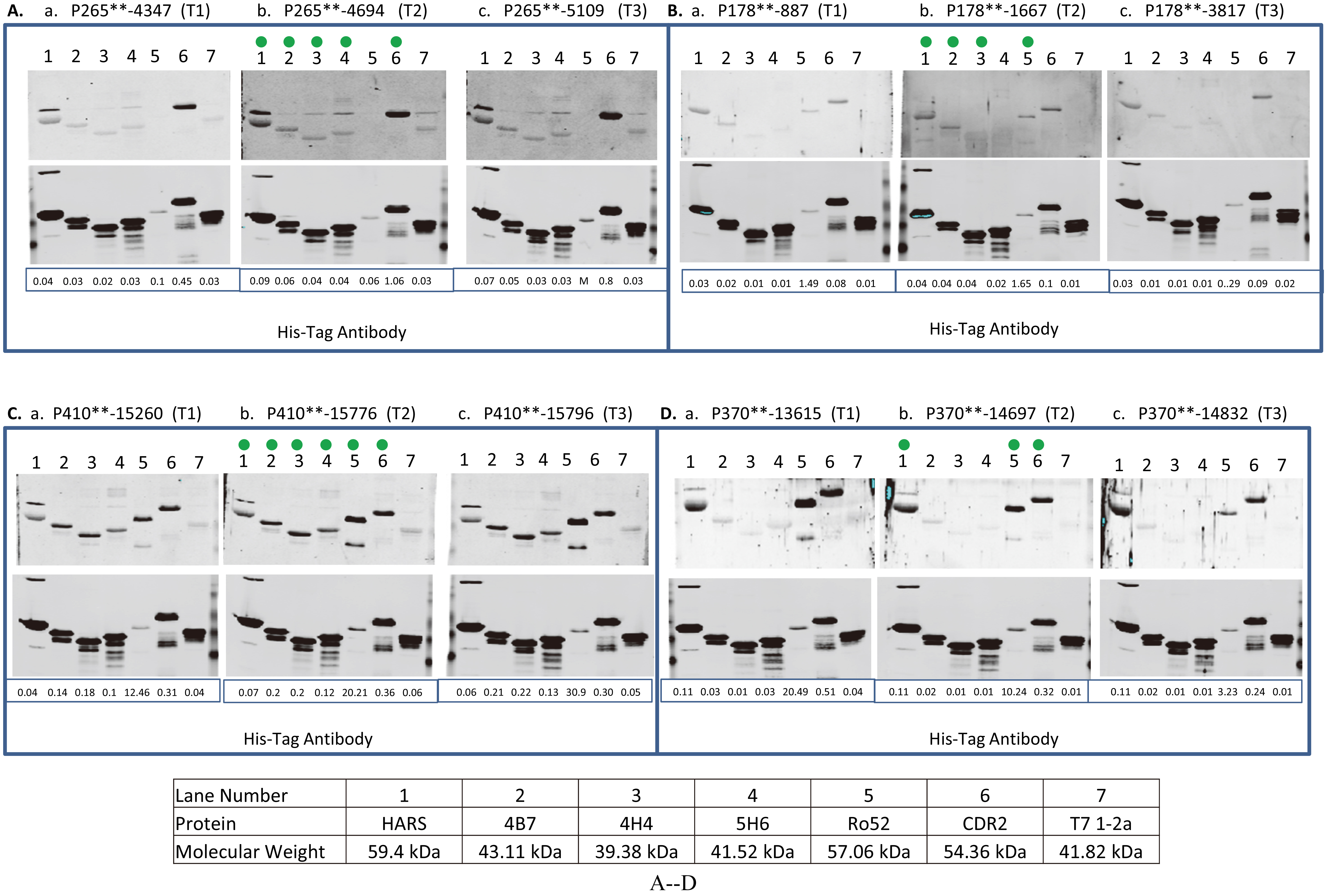
continued.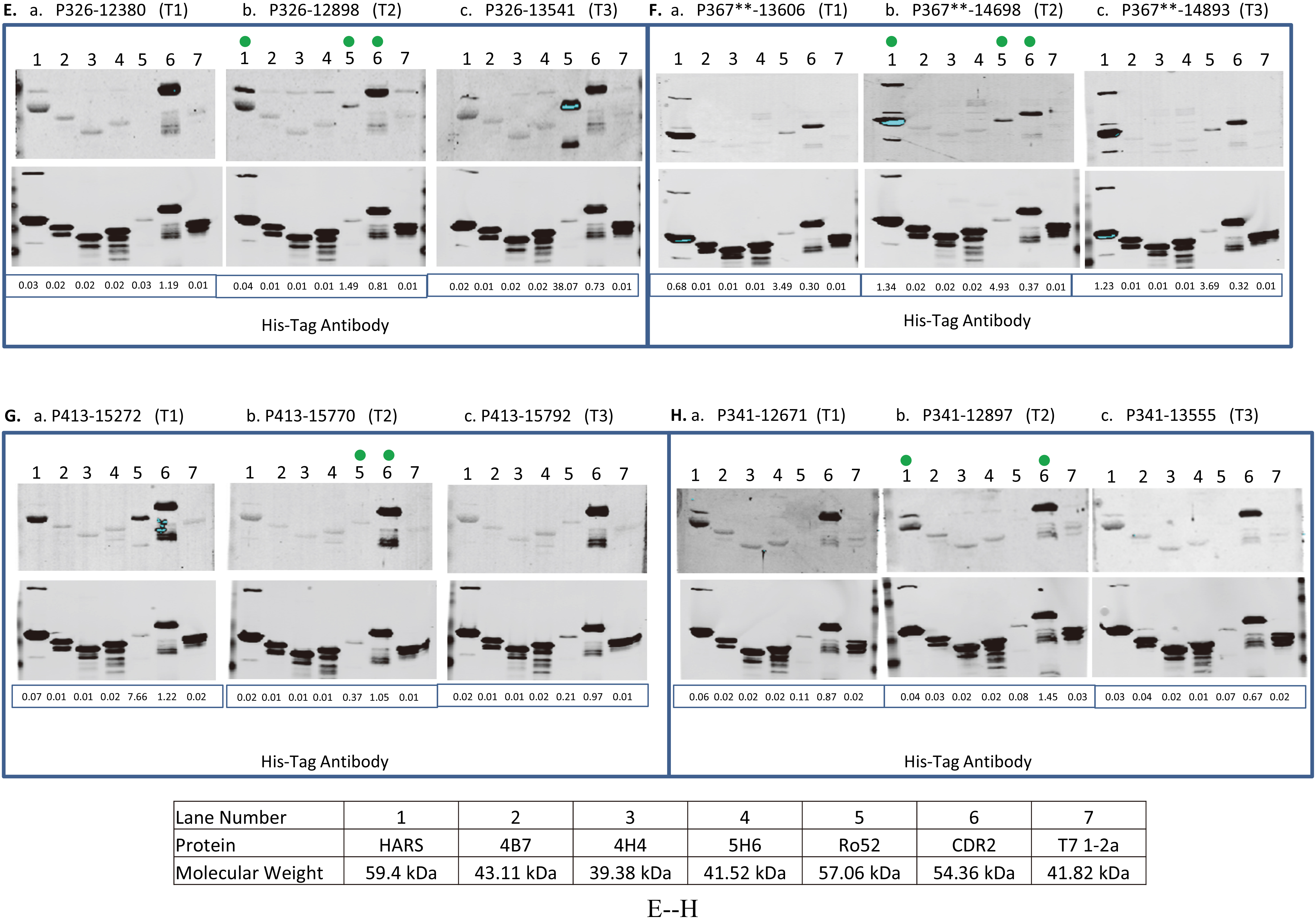
continued.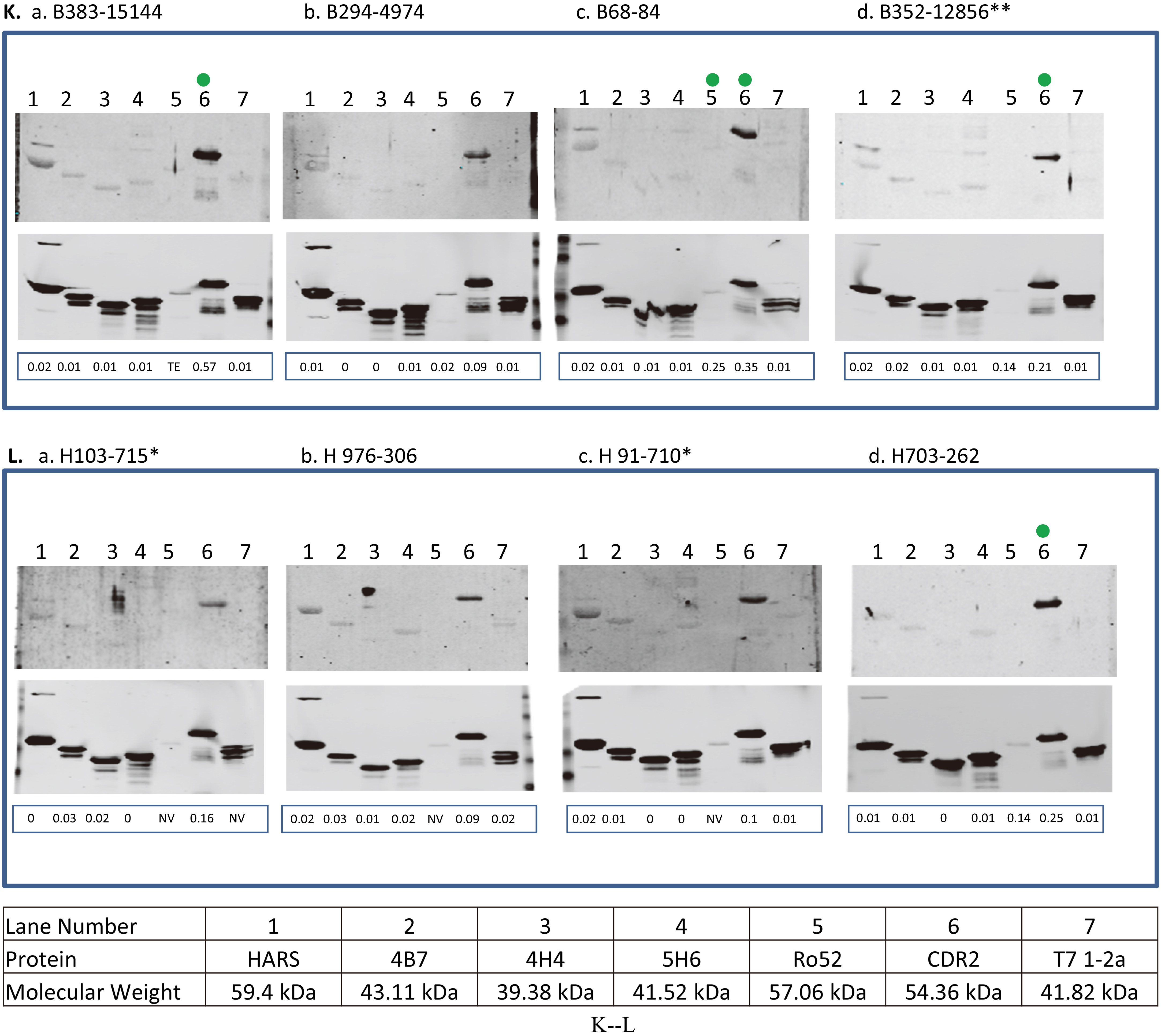
Reactivity of antigens with 5 recurrent and 5 non-recurrent ovarian cancer patients (training set) and an independent recurrent ovarian patient population (test set,
Note: The sero reactivity of the recombinant antigen biomarkers revealed 3 different range of affinity toward serum IgGs such as strong (
Sensitivity of 6 antigens (in combinations of 1, 2 or 3 antigen panels) to predict recurrence prior to clinical recurrence in 21 ovarian cancer patients
Note:
cancer patients respectively (patients with asterix shown in Table 2a) who had stable disease or under treatment at time T2 when their CA125 values were below or very close to the standard cutoff (35 U/ml). In contrast, the immunoreactivity values of 4B7, 4H4 and 5H6 were below cutoff for those patients. The reactivity of Ro52 antigen with ovarian cancer patient P326 was increased by 51.5 fold (fold change is calculated by dividing the normalized signal intensity of the antigen reactivity with the patient’s serum IgG by the normalized signal intensity of the reactivity of His-tag at the N terminus of the antigen with anti-His-tag antibody) in contrast to immunoreactivity values of CDR2 or HARS that dropped by 1.5 fold or remained the same at 4.3 months when her CA125 value was only 41 U/ml before the clinical recurrence compared to the sero-reactivity at the time of diagnosis ((Fig. 1E, a, b, lanes 5, 6, and 1), Table 2a). For patient P367, the immunoreactivity of Ro52 and HARS was increased by 1.4 and 2 fold during the monitoring phases at 4.3 months (CA125 29 U/ml) before the clinical recurrence compared to the their immunoreactivity at diagnosis ((Fig. 1F, a, b, lanes 5 and 1), Table 2a). The immunoreactivity of CDR2 antigen with P367 at times T1 and T2 remained almost the same, but the immunoreactivity value was 2.2 fold above the cutoff at T2. Although the patient P398 showed no increase in the serum reactivity with Ro52 protein at 10.3 months (CA125 level 24 U/ml) before the clinical recurrence over the time at diagnosis, the immunoreactivity of Ro52 was significantly higher, 6.7 fold above the cutoff at T2 ((Fig. 1I, a, b, lane 5), (Table 2a)). However, the immunoreactivity of HARS and CDR2 antigens with the patient P398 showed weaker to reactivity below cutoff (Fig. 1I, a, b, lanes 1 and 6), (Table 2a). The high reactivity of Ro52 with the patient P398 could be associated with the presence of residual tumor tissues after her first sub-optimal debulking, indicating that a high anti-Ro52 titer is needed for the equilibrium state when tumor cells remain in a dormant state before they develop into a highly progressive phenotype [26]. Although the reactivity of HARS with the patient P393 remained almost the same at T1 and T2, the immunoreactivity of HARS was about 3 fold above its cutoff at T2 in contrast to Ro52 immunoreactivity that was below its cutoff at T2. The immunoreactivity of CDR2 antigen with the same patient P393 dropped by 1.4 fold at T2 (Fig. 1J, a, b, lanes 1, 5 and 6), (Table 2a). CDR2 expression is upregulated in ovarian tumors [10], so there is a possibility of sequestration by antigen blocking of newly synthesized Yo antibodies by circulating CDR2 protein. This can occur by the process of shedding, secretion of tumor antigens or antigens released due to apoptotic cell death as revealed by the proteomic analyses of 3 ovarian cancer cell lines by Faca et al. [11]. These shed antigens can enter into circulation and can bind to their respective antibodies.
The immunoreactivity of Ro52, CDR2, HARS, 4B7, 4H4, and 5H6 antigens showed association of recurrence with 8/16, 12/16, 10/16, 3/16, 3/16 and 3/16 ovarian cancer patients respectively who had no evidence of disease (NED), except one patient whose disease was not specified, at a median lead time of 5.85 months before the clinical recurrence at time T2 when most of the patients had CA125 levels below the standard cutoff (35 U/ml), with the exception of only one patient P178 who had a high CA125 value 203 U/ml at time T2 (Table 2a–2b). For Ro52, HARS, 4B7 antigens, reactivity increased by 1.6, 1.6 and 1.4 fold with the patient P410, however, the immunoreactivity values of CDR2, 4H4 and 5H6 remained the same at T1 and T2 (individual immunoreactivity values of CDR2, 4H4 and 5H6 were 2, 6.6 and 4 fold higher than their cutoffs at time T2) during the monitoring phases at 3.23 months (CA125 24 U/ml) before the clinical recurrence compared to their time at diagnosis (Fig. 1C, a, b, lanes 5, 1, 2, 6, 3, and 4). The immunoreactivity of CDR2 and Ro52 antigens with the patient P370 dropped by 1.6 and 2 fold at recurrence interval of 2.63 months (CA125 13 U/ml). However, immunoreactivity of HARS remained the same at T1 and T2 (individual immunoreactivity was 3.6 fold higher that its cutoff at T2) ((Fig. 1D, a, b, lanes 6, 5 and 1), Table 2a). The drop in immunoreactivity of CDR2 and Ro52 (individual signal intensity values for both the antigens at time T2 were still 1.9 and 60 fold above cutoff) for P370 who had very short DFI 2.63 months could be related to the aggressive tumor growth that overpowered immune surveillance. Studies have indicated that tumor cells secrete immunosuppressive factors like IL-10, PEG2, TGF
Serological screening of antigens using healthy women and women with benign gynecological diseases
The 6 recombinant biomarkers were also tested for their immunoreactivity with the serum IgGs obtained from few healthy women and women with benign gynecological disease (they all had ovarian cysts/Benign Cystic Ovarian Neoplasms) (Fig. 1K–L). As the analyses of immunoreactivity of antigens with all the benign and healthy women is generally performed to achieve a higher specificity for the early diagnosis of ovarian cancer and not for predicting recurrence in a cohort of patients who are under surveillance during monitoring phase, only few western blot images of sero-reactivity of 6 antigens with benign and healthy women were shown for the present study. Only CDR2 antigen exhibited strong reactivity with a patient with benign disease, B383 (3.4 fold above cutoff) and with other benign and healthy women, the reactivity was in the range of 1.2 to 2 fold above the CDR2 cutoff. The frequency of CDR2 antigen reactivity with healthy and benign samples was higher more often than the rest of the 5 antigens.
The above results indicated that out of 6 recombinant antigens employed to assess their sero-reactivity with serum IgGs obtained from 21 ovarian cancer patients, 3 antigens, Ro52, CDR2 and HARS showed high frequency and strong reactivity, and the remaining 3 antigens, 4B7, 4H4 and 5H6 showed low frequency and moderate reactivity during the monitoring phase when most of the patients had CA125 levels above the standard cutoff (35 U/ml).
Determination of sensitivity of antigens based on their serological immunoreactivity with ovarian cancer patients for prediction of recurrence before the clinical relapse
The serologic reactivity of all the 6 recombinant antigens with serum IgGs obtained from 5 recurrent and 5 non-recurrent ovarian cancer patients (training set), and 21 recurrent ovarian cancer patients (test set) at time T2 before the clinical recurrence is shown in Table 3. The sensitivity of 6 antigens (single or in combination) to predict recurrence before the clinical recurrence in 21 ovarian cancer patients (test set) was determined.
Determination of sensitivity using one antigen at a time
Analyses of western blot immunoassays revealed that individually, Ro52, CDR2, HARS, 4B7, 4H4, and 5H6 antigens resulted in sensitivities of 52.4% (11/21), 71.4% (15/21), 66.7% (14/21), 14.3% (3/21), 14.3% (3/21) and 14.3% (3/21) respectively (Tables 3 and 4).
Determination of sensitivity using a combination of any 2 antigens at a time
High sensitivities were observed for a combination of any 2 antigens, for example, 86% (18/21) for Ro52 and CDR2 antigens, 81% (17/21) for CDR2 and HARS antigens, 81% (17/21) for Ro52 and HARS respectively. Among the other combinations of antigens in a panel of 2 that resulted in moderate sensitivities were 62% (13/21) for 5H6 and Ro52 antigens, 76% (16/21) for each of the combinations of 4B7 and CDR2, 4H4 and CDR2, and 5H6 and CDR2 antigens, and 71.4% (15/21) for 5H6 and HARS antigens respectively (Table 4).
Determination of sensitivity using a combination of any 3 antigens at a time
High sensitivities were observed for a combination of any 3 antigens, for example, 90.5% (19/21) for Ro52, CDR2 and 5H6 antigens (Fig. 2A), 86% (18/21) for HARS, CDR2 and 5H6 (Table 4), 86% (18/21) for Ro52, CDR2 and HARS (Fig. 2B), 80.9% (17/21) for CDR2, 4B7 and 5H6 or CDR2, 4H4 and 5H6 respectively (Table 4). Among the other panel of 3 antigens, moderate sensitivities were observed for 61.9% (13/21) for the combinations, Ro52, 4B7 and 5H6, or Ro52, 4H4 and 5H6 (Table 4).
Determination of sensitivity of different combination of antigens for predicting ovarian cancer recurrence using venn diagram. Venn diagrams represented the immunoreactivity of each antigen (above its cutoff) with ovarian cancer patient’s serum sample obtained at time T2 (the blood sample collected approximately 3–15 months before the clinical recurrence, ideally with normal CA125 and no evidence of disease). Panels (A–B) represent venn diagram of different combination of antigens, Ro52, CDR2 and 5H6 (A), and Ro52, HARS, and CDR2 (B) used for determining sensitivity for predicting ovarian cancer recurrence.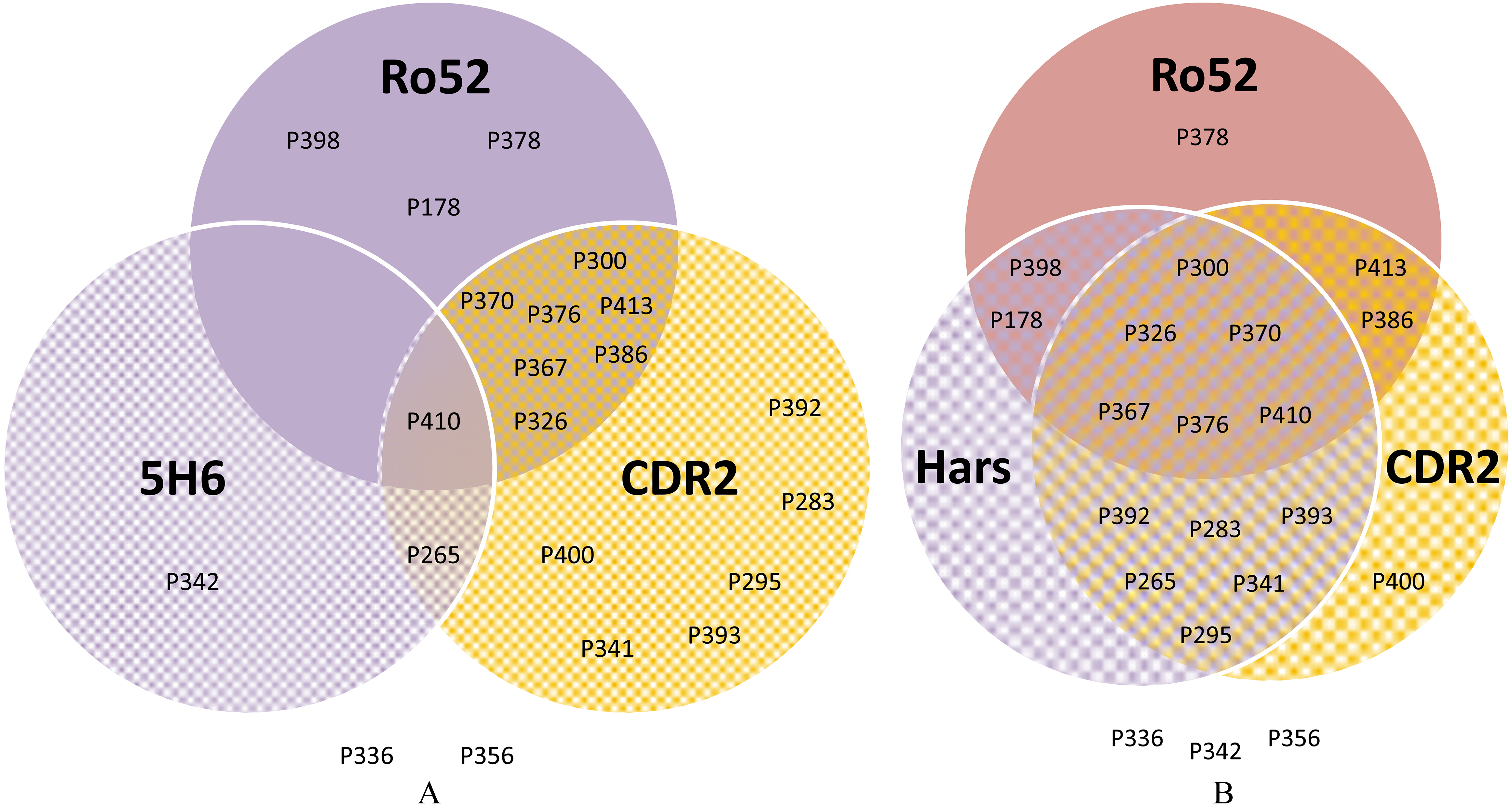
Our results indicate that a panel of 3 antigens, Ro52, CDR2 and 5H6 resulted in 90.5% sensitivity in predicting recurrence in 21 ovarian cancer patients at a median lead time of 5.03 months before the clinical relapse when CA125 levels were within the normal range (
Studies have shown that early onset of some paraneoplastic neurological symptoms is generally associated with the occurrence of onconeural antibodies that can serve as a diagnostic tool for a suspicion of ovarian cancer in asymptomatic high-risk patients carrying BRCA1/2 mutations [6, 29]. Very few studies have shown the utility of these onconeural antibodies for disease monitoring in cancer patients. One study reported that antibodies to paraneoplastic antigen Ma2 showed a high sensitivity, specificity and accuracy (AUC between 0.734 and 0.816) to predict early recurrence in 124 patients who had small intestine neuroendocrine tumors (SI-NETs) [9].
In our present study, we assessed the immunoreactivity of 6 recombinant antigens with serum IgGs obtained from 21 ovarian cancer patients to predict recurrence at various times prior to clinical/radiologic evidence when the level of CA125 was below the normal range (35 U/ml). Three paraneoplastic antigens, Ro52, CDR2 and HARS showed strong immunoreactivity association and the other 3 antigens, 4B7, 4H4 and 5H6 exhibited moderate immunoreactivity association with the recurrence status of the 21 ovarian cancer patients, majority of which showed no elevation of CA125 (standard cutoff 35 U/ml) (Table 2a–2b). Out of those 3 recombinant antigens, only 4B7 showed amino acid homology with the known paraneoplastic antigens, Histidyl t-RNA synthetase or HARS. Despite the homology to the C-terminal region with HARS protein, a similar frequency of reactivity was not observed between the recombinant 4B7 peptide and the full length HARS protein. A similar discordance was observed in most patients diagnosed with idiopathic myositis using epitope mapping of HARS protein which showed that 3 epitopes located at the N terminal region were mostly the reactive peptide segments [18]. As dermatomyositis is often associated with the occurrence of ovarian cancer, several processes that cause epitope spreading resulting in broadening of anti-HARS specificity can also occur during the course of development of ovarian cancer [18]. Although 4B7, 4H4 and 5H6 antigens encoded short peptides, exhibited low frequency and weak to moderate serological reactivity toward the ovarian cancer patients, these antigens still hold potential as biomarkers to monitor disease better than CA125 because of their high specificities against the 5 non-recurrent patients in the training set (Table 1). Those previous 3 biomarkers, 4B7, 4H4, and 5H6 were T7 phage encoded peptides and in our previous study their immunoreactivity was assessed by robotically printing the individual phage lysates on nitrocellulose membranes that were immunoscreened against patients’ sera. Therefore, the immunoreactivities of these antigens assessed by the current study could not be compared with that of our previous ovarian cancer recurrence study because in the current study we used purified recombinant proteins in western blot immunoassay in contrast to the previous study in which T7 phage lysates of the individual phage clones were employed for immunoscreening on protein microarrays.
The paraneoplastic antigen Ro52 is an E3 ubiquitin ligase and elevated levels of circulating anti-Ro52 antibodies have been shown to cause autoimmunity in patients with Sjögren’s syndrome and systemic lupus erythematosus (SLE) [3]. Mechanistically Ro52 causes inflammation by the process of ubiquitination of interferon regulatory factors [3]. The paraneoplastic antigen CDR2 has been shown to be expressed in Purkinje cells, testis and ovarian cancer [27]. There is an association of onconeural anti-Yo antibodies (targets CDR2 antigen) with ovarian cancer patients who developed paraneoplastic cerebellar degeneration before cancer diagnosis [21]. CDR2 is a cell cycle regulated protein that is highly expressed during mitosis in tumor cells. CDR2 interacts with c-Myc protein that can enhance gene transcription [23]. The occurrence of anti-Jo-1 antibodies targeting HARS antigen has been associated with myositis, a paraneoplastic neurological disorder that causes inflammation and weakness in muscles. Twenty-five percent of patients who are diagnosed with polymyositis or dermatomyositis harbor anti-Jo-1 antibodies [16]. Reports indicated that concurrent appearance of Jo-1 and Ro52 antibodies in patients diagnosed with antisynthetase syndrome (ASS) was associated with elevated risk of breast, ovarian, and esophagus cancers [17]. Our study employed serial ovarian cancer serum samples that were not used in our discovery of these biomarkers. However, a limitation of our present study is that the training set population which was used to set the threshold of each antigen to achieve high specificity was comprised of only 5 recurrent and 5 non-recurrent ovarian cancer patients. The reasons for using a smaller size of patient population in the training set for the determination of threshold of each antigen were first, in the present study, we wanted to reevaluate the strength of immunoreactivity of the previous biomarkers, 4B7, 4H4, 5H6 [5] on the western blot platform to predict ovarian cancer recurrence prior to its clinical recurrence in patients who showed no elevation in CA125 level above its clinical threshold (35 U/ml) which led us to use the same training set as before; second, for our previous study, we were able to accrue few non-recurrent ovarian cancer patients (because the disease often recurs) who met patients’ accrual criteria and those non-recurrent ovarian cancer patients were split into training and test sets which made the size of the training set smaller than expected [5]; third, in our earlier immunoassay based studies, the same patient population of 5 recurrent and 5 non-recurrent ovarian cancer patients (current training set) as well as serum samples obtained from patients with paraneoplastic syndrome were immunoscreened with known paraneoplastic antigens to determine the immunoreactivity of those paraneoplastic antigens using paraneoplastic myositis line blots (EuroImmun, Morris Plains, New Jersey) and Paraneoplastic Antigen line blots (Ravo Diagnostika, Freiburg, Germany). Similar immunoreactivity of HARS, Ro52 and CDR2 antigens with both recurrent and non-recurrent ovarian cancer patients in the training set was observed both on western blot (current study) and paraneoplastic antigen line blots (previous study) (data not shown). The immunoscreening analyses provided insights into usefulness of using true paraneoplastic protein antigens for early diagnosis and recurrence of ovarian cancer (data not shown). Therefore, our present was enhanced by using the same ovarian cancer patient population in the training set to choose the threshold of each antigen that was applied to an independent test set patient population for the evaluation of their potential as biomarkers for prediction of ovarian cancer recurrence with a longer lead time than CA125. We propose to use a large independent population of recurrent and non-recurrent ovarian cancer patients in the training set for future validation studies. In addition, the test set study population did not have non-recurrent ovarian cancer patients. As our present study was a prospective-retrospective pilot study based on finding the utility of 6 biomarkers for prediction of ovarian cancer recurrence in patients prior to clinical recurrence, we needed an independent patient population in the test set who had CA125 levels below its threshold (35 U/ml) during the monitoring phase before clinical recurrence. The present study only focused on determining the sensitivity of the immunoassay used for prediction of ovarian cancer recurrence. If we had included non-recurrent ovarian cancer patients, we could have measured specificity along with the sensitivity of the immunoassay. Therefore, in the study we included this as one of the limitations of the study. We propose to include both recurrent and non-recurrent ovarian cancer patients for the future validation studies.
Conclusion
In conclusion, a combination of 4 antigens, Ro52, CDR2, HARS and 5H6 in a panel, showed a sensitivity of 90.5% in a western blot-based immunoassay for early prediction of recurrence in 21 ovarian cancer patients during the surveillance period when most of these patients had normal levels of CA125 level (cutoff 35 U/ml). The median lead time of prediction of recurrence was 5.03 months which was better than CA125. We propose that paraneoplastic autoantibodies occur in asymptomatic cancer patients and can be used for early detection of cancer. Our goal for a future study is to evaluate the potential utility of these 6 markers in combination with other tumor associated antigens that have been shown to be overexpressed in late stage serous adenocarcinoma with concurrent elicitation of humoral immune response in ovarian cancer patients, to develop a panel of biomarkers that can predict the recurrence during the monitoring phase prior to clinical recurrence when the level of CA125 remains below the standard cutoff (35 U/ml). Early prediction of recurrence before the cancer progresses to more aggressive phenotype can provide patients some time to be treated with conventional chemotherapy regimen to prevent recurrence of ovarian cancer.
Conflict of interest
Dr. Tainsky, Dr. Chatterjee and Ms. Levin are coinventors on a patent on ovarian cancer recurrence biomarkers.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/CBM-170652.
sj-pdf-1-cbm-10.3233_CBM-170652.pdf - Supplemental material
Supplemental material, sj-pdf-1-cbm-10.3233_CBM-170652.pdf
Footnotes
Acknowledgments
This project was supported by The Barbara and Fred Erb Chair in Cancer Genetics and an NIH grant R21 CA187278-0. Laura Hurley was supported by T32 training grant CA009531. The authors would like to thank Mike Saleh for volunteering his time in the laboratory. A special thanks to the patients and healthy volunteers who donated serum and tissue for the study. This work could not be done without their willingness to participate in research.