
Abstract
Membranous glomerulonephritis can occur as a rare paraneoplastic complication of human cancers. In this case report, we describe a patient who presented acutely with symptoms of the nephrotic syndrome including heavy proteinuria and anasarca. He was subsequently diagnosed with membranous glomerulonephritis, and soon afterwards was found to have stage IIIB non-small cell lung cancer. Following chemoradiation therapy, both the patient's cancer and membranous glomerulonephritis dramatically improved. However, approximately 14 months following his initial presentation, the patient was found to have a recurrence of his nephrotic-range proteinuria which corresponded temporally with recurrence of his cancer. We present details of the case and a review of the relevant scientific literature.
Introduction
Nephrotic syndrome refers to an array of glomerular disorders in which the filtration barriers of the renal glomeruli are compromised, leading to increased permeability of the filtration complex to macromolecules which leads to proteinuria >3 g/day, hypoalbuminemia, and edema. Additional complications include hypercholesterolemia, increased susceptibility to infections due to urinary loss of immunoglobulins, and increased frequency of thromboembolic events due to urinary loss of antithrombotic factors. 1 Approximately 30% of adult cases of nephrotic syndrome fall within the subtype of membranous glomerulonephritis (MGN). In MGN, there is uniform glomerular basement membrane thickening within the capillary loops, and diffuse granular deposits of IgG and the complement fragment C3 seen by immunofluorescence. Electron microscopy typically shows dense subepithelial deposits, with effacement of the podocyte processes. 1 These changes result in severe compromise of both the size selective and charge selective barrier to filtration that the glomerulus usually provides. 2 It has been observed that in a small subset of patients with nephrotic syndrome there is an associated diagnosis of cancer. MGN is the most common subtype associated with solid tumors, with lung and stomach being the predominant cancers. Minimal change disease is the subtype most commonly associated with Hodgkin's Disease. 3
Case Report
A 49 year old man with no significant past medical history but a sixty pack-year smoking history developed fatigue, foamy urine and dramatic anasarca over a period of several days. An inpatient workup revealed acute renal failure, with serum creatinine of 1.7 mg/dL. Urinalysis showed 12 g protein/24 hours, urinary microalbumin/creatine ratio 8018 (mg microalbumin/g of creatinine), urinary protein: creatinine (P/C) ratio of 11.8 (protein and creatinine both measured as mg/dL), and 9/high powered field granular casts. Blood work revealed low serum proteins: albumin 1.2 g/dL and total protein 4.3 g/dL. Additionally, a fasting lipid panel was drawn, and it showed total cholesterol of 443 mg/dL, low density lipoprotein (LDL) 345 mg/dL, high density lipoprotein (HDL) 36 mg/dL, and triglycerides 309 mg/dL. Hemoglobin A1C was within normal limits (5.6%), as were HBV and HIV serologies, anti-neutrophil cytoplasmic antibody (ANCA), and anti-glomerular basement membrane (GBM) antibody levels. Anti-nuclear antibody (ANA) titers were mildly elevated at 1:40, although anti-dsDNA titers were normal (<1:10). A clinical diagnosis of nephrotic syndrome was made and a renal biopsy was performed. Light microscopy revealed diffuse capillary wall thickening (Figure 1A). Immunofluorescence staining displayed a high level of IgG and C3 staining in a granular pattern within the capillary loops and mesangium (
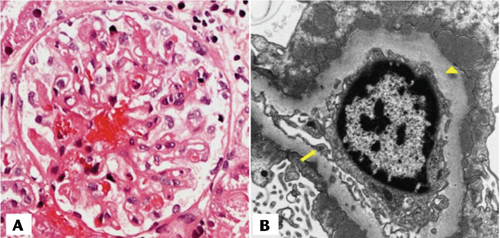
Diagnostic kidney biopsy. A) Hematoxylin and Eosin staining displays diffuse thickening of the capillary walls. B) Transmission electron micrograph of representative podocyte showing effacement and fusion of the podocyte processes (arrow) and diffuse subepithelial dense deposits (triangle).
The patient's edema and foamy urine continued after discharge, and over the next several weeks he developed worsening fatigue, dizziness, and continued severe diffuse soft tissue edema. He was prescribed a regimen of prednisone 40 mg/day for immunosuppressive therapy along with diuretics in an attempt to control his edema. However, over several weeks his edema continued to worsen, and he developed nausea, chest tightness, and dyspnea on exertion and was readmitted to the hospital. Blood work revealed an acceleration of his nephrotic syndrome: serum creatinine level of 2.32 mg/dL, serum albumin <1 g/dL, total serum protein 3.4 g/dL and urine P/C ratio of 8.9. A chest CT scan was performed and revealed a 4 cm enlarged lymph node within the aortopulmonary window, a 2 cm enlarged lymph node in the left paratracheal region, bilateral pleural effusions, and intra-abdominal ascites. Bronchoscopy revealed no endobronchial lesions and endoscopic ultrasoundguided fine needle aspirate of the enlarged left paratracheal node revealed squamous cell carcinoma consistent with lung as the primary site of origin. Staging PET/CT revealed intense FDG avidity in the mediastinum (left and right paratracheal and aortopulmonary regions) and left hilum. No distant metastasis was identified. MRI of the brain showed no CNS metastases and upper endoscopy showed no abnormalities of the esophagus. The patient was classified as having stage IIIB, TXN3M0 nonsmall cell lung cancer. His steroid regimen was tapered off, and he was started on definitive treatment with chemoradiation therapy. Radiation therapy was delivered using a 3D conformal technique to a total dose of 6600 cGy to the left hilum and mediastinum in 37 fractions. He had weekly carboplatin/paclitaxel concurrent with radiation followed by 2 full cycles of carboplatin/paclitaxel for consolidation. He tolerated treatment very well. Followup chest CT scan performed 1 month after completion of chemoradiation showed marked tumor response to therapy (Figure 2B). At this time, his serum creatinine was 0.91 mg/dL, serum albumin was 2.6 g/dL, and urine P/C ratio was 4.9, all of which were greatly improved since his initial presentation with nephrotic syndrome (Figure 3).

Computed tomography and (18)F-fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET). A) Initial staging D-glucose positron emission tomography/computed tomography (PET/CT) shows increased uptake in right paratracheal area and intense uptake in the left paratracheal and aorticopulmonary window areas (arrows); B) Repeat CT scan performed nearly 4 months after initiating chemoradiation shows marked regression of left hilar and mediastinal lymphadenopathy (arrow); C) Repeat PET/CT 14 months following diagnosis displays worsening right paratracheal lymphadenopathy (arrow).

Renal function over time. First solid arrow refers to the initiation of chemoradiation on day 55 after initial presentation. Second solid arrow corresponds to date of follow-up computed tomography imaging which displayed marked regression of malignancy following treatment (see Figure 2B). Third arrow represents confirmation of disease progression as seen in (see Figure 2C).
He remained disease-free from his lung cancer and remained asymptomatic from his renal disease. He had normal renal function and had no edema until a follow up appointment 14 months after his initial presentation. At this time he noted recurrence of foamy urine and was found to have elevated urinary P/C ratio of 6.1, which had increased from 3.3 five months earlier. Serum creatinine remained within the normal range. Repeat chest CT scan revealed new superior mediastinal lymphadenopathy and PET scan confirmed recurrent disease with FDG avidity in the mediastinum and left hilum (Figure 2C). He was started on salvage chemotherapy consisting of carboplatin and Abraxane.
Discussion
Several theories have been postulated to explain the link between paraneoplastic glomerulonephropathies and cancer. One potential mechanism is the generation of autoantibodies that directly interact with the basement membrane of the glomerulus. A recent landmark study identified the phospholipase A2 receptor (PLA2R), a podocyte cell membrane protein, as the likely target of autoantibodies in patients with idiopathic MGN.
4
In this study, antibodies to PLA2R were identified in 70% of patients with idiopathic MGN. However, these antibodies were not seen in any patients with secondary MGN. It appears that secondary MGN likely involves either a different antibody target which has not yet been elucidated or a different mechanism. A serum assay of anti-PLA2R antibodies was not performed during the diagnostic workup of the patient described in this case report. The current leading proposed pathophysiologic mechanism for paraneoplastic MGN is the deposition of circulating tumor antigen/antibody complexes within the glomeruli, which initiates inflammatory changes that compromise the filtration barrier. Indeed, the deposition of immune complexes may be a common phenomenon in patients with cancer. A postmortem study of 189 patients observed that immune deposits were found in 17% of a group patients with a variety of solid tumor types
Relapse of the nephrotic syndrome concomitant with progression of cancer is one of the diagnostic criteria of paraneoplastic glomerulonephropathies. However, little has been described thus far about the mechanistic and temporal links between the recurrence of symptoms of MGN and relapse/progression of malignancies thus far. In this report, the patient achieved regression of both his cancer and his nephrotic syndrome following chemoradiation. However, after several months he displayed laboratory signs of declining renal function and worsening proteinuria that heralded a progression of his malignancy as confirmed by PET-CT shortly thereafter.
Published case reports of lung cancer and associated membranous glomerulonephritis based on a PUBMED review using the search terms
Conclusions
Paraneoplastic membranous glomerulonephritis is a rare complication of non-small cell lung cancer. The renal function appears to correlate with the response and status of the primary lung malignancy. Renal function should be subject to close ongoing surveillance for recurrence of proteinuria. Even in the absence of clinically symptomatic nephrotic syndrome, rising proteinuria can herald recurrence/progression of the underlying malignancy and should prompt further investigation for progression of malignant disease.
Footnotes
Conflict of interests: the authors declare no potential conflict of interests.