
Abstract
OBJECTIVE:
To assess whether adrenalectomy may improve biochemical and metabolic impairment for patients with subclinical Cushing syndrome (SCS) due to adrenal incidentaloma (AI) compared with conservative management.
METHODS:
A total of 87 patients with SCS due to AI in Peking Union Medical College Hospital between September 2011 and January 2016 have been treated. Forty-eight patients underwent laparoscopic adrenalectomy (operative group), whereas 39 were managed conservatively (control group).
RESULTS:
The duration of follow-up was 32.5
CONCLUSIONS:
Laparoscopic adrenalectomy should be performed for patients with SCS due to AI.
Introduction
Adrenal incidentaloma (AI) is an adrenal mass that is typically discovered serendipitously during radiologic examinations performed for unrelated reasons [1]. Recently, with the extensive application of CT and MR imaging examination, the prevalence of AI has increased, which has been estimated as 1%
SCS adrenal tumor CT findings (indicated by the arrow), smooth edges, smooth density showed in A) enhanced showed in B.
Despite the lack of specific clinical manifestations of AI, there are still 5
Patients
The definition of AI is based on the guidelines of the American Society of Clinical Endocrinology (AACE) and the American Society of Endocrine Surgeons (AAES) [13]. In the absence of symptoms associated with adrenal disease or routine physical examinatio, an adrenal tumor that is unexpectedly discovered by imaging methods, excluding from the diagnosis of cancer screening. Imaging needs to be met: unilateral renal AI, tumor maximum diameter greater than 1 cm, uniform density, smooth edges, no significant signs of malignancy (Fig. 1). The diagnosis of SCS was according to the guidelines of AACE and AAES [13], The consensus of AI experts on the diagnosis and treatment of the endocrine Physicians Association in Italy [14] and France [15]. The diagnosis of SCS was based on the presence of at least one of the following in addition to cortisol levels greater than 1.8
Treatment
Forty-eight patients were treated by laparoscopic unilateral adrenal resection of ipsilateral adrenal (operation group). Of these patients, 18 cases were male and 30 cases were female. The median age was 51.8
Patient and tumor characteristics in all patients
Patient and tumor characteristics in all patients
Continuous variables were expressed as mean
Results
Tumor characteristics
Resection of the tumor was accorded with the pathological diagnosis of adrenal cortical adenoma specimens, gross specimen was round, encapsulated, brown in profile, and visible bleeding area. Microscopic specimen showed that the tumors mainly composed of clear cells (Fig. 2).
Tumor has a complete capsule, the section was brown, visible bleeding area (A); HE staining 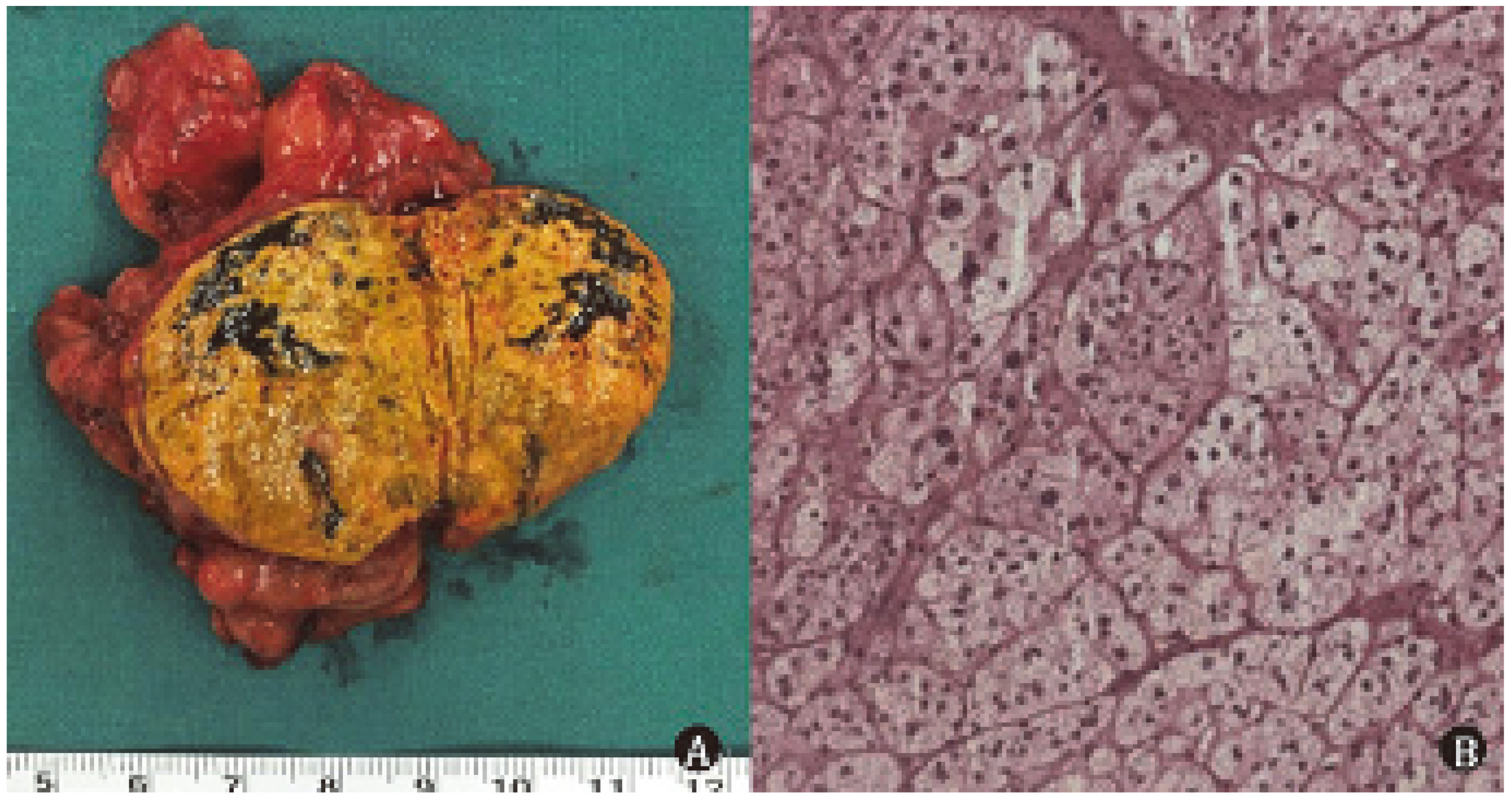
The follow-up time of the operation group was 32.5
The prevalence of patients affected by metabolic syndrome after following up
Abbreviations: BMI body mass index; ACTH adrenocorticotropic hormone; UFC urinary free cortisol; 1 mg-DST overnight 1 mg dexamethasone suppression test; HbA1c glycosylated hemoglobin; TG triglyceride; HDL-C high density lipoprotein.
No hormone replacement therapy was performed preventively after the operation, and 3 patients were given hormone replacement therapy during hospitalization due to adrenal insufficiency. All patients were successfully treated with hormone replacement therapy within 3 months, and the duration of treatment was 9 weeks, 10 weeks and 12 weeks. At the end of follow-up, there was no serious cardiovascular and cerebrovascular accident or death in the two groups, and there was no patients progressed into clinical CS in the non operation group.
In recent years, SCS has become a hot spot of research. On the one hand, the prevalence of AI is increasing year by year. On the other hand, there is a close relationship between SCS and cardiovascular complications. It was reported that the prevalence rates of hypertension, abnormal blood glucose and obesity in SCS patients were 72%, 46% and 39%, respectively [14], which suggested that even mild hyperlipidemia might lead to metabolic disorders of blood pressure, blood glucose and lipids. Other studies have shown that the incidence of cardiovascular accidents and related mortality risk in patients with SCS were higher than those in the general population [16].
Diagnostic criteria
Due to the lack of specific clinical signs and laboratory tests, there is no consistent diagnostic criteria for SCS. The difference of diagnostic criteria is an important reason for the controversial findings [17]. At present, several assay indexes were applied including: plasma ACTH, 24 h UFC and 1 mg DST. Among them, 1 mg DST is considered to be the most sensitive test for the detection of cortisol, but the cut-off value of 1 mg DST remains controversial. The Endocrine Society of France used 1.8 ug/dL as the cut-off value of 1 mg DST, with a sensitivity of more than 95%, but the specificity was 70%
Treatment of SCS related metabolic abnormalities
In view of the published results of the present issue, whether adrenalectomy can alleviate SCS related metabolic disorders remains controversial. Adrenalectomy appears to be effective in correcting in patients with hyperlipidemia [17, 23], but most studies lack the results of postoperative hormone levels [24]. More clinical studies are needed to assess the role of adrenalectomy in the treatment of hyperlipidemia. In this study, a detailed record of the changes of 1 mg DST, ACTH 24 h and plasma UFC had been performed from admission and final follow-up. We found that of laboratory indexes were recovered to normal after the operation, which further confirmed the corrective effect of adrenalectomy on hypercortisolemia.
In the aspect of blood pressure control, Iacobone M summarized the research published in recent years, and found that 72% of patients with SCS postoperative blood pressure was improved. While the blood pressure of patients in conservative treatment group was not improved, suggesting that adrenalectomy has a role in improving blood pressure [25]. However, some other studies showed adrenalectomy could not improve blood pressure control [26, 27]. In this study, the blood pressure control postoperative was better than that preoperative in the operation group, but there was no improvement in the conservative treatment group. In the aspect of blood glucose control, a retrospective study reported that 10% patients completely recovered and 40% patients improved after adrenalectomy, and no improvement of blood glucose were showed in conservative treatment group, there are a number of studies support the this conclusion, but also no lack of research results oppsite to the conclusion [28, 29]. This study found that although the proportion of abnormal blood glucose and fasting blood glucose had no significant difference in the two groups, HBA1c level decreased in the operation group, suggesting that adrenalectomy might play a vital role in the long-term control of blood glucose. In the aspect of blood liquid control, Guerrieri M have found that some patients with postoperative blood lipids improved [30], while other researchers found that surgery does not improve blood lipid metabolism [25]. In this study, the results of lipid metabolism are similar to previous reports, suggesting that the role of adrenalectomy in lipid metabolism is not clear, and it might play a role in improving the metabolism of TG.
Hormone replacement therapy after adrenalectomy
Adrenalectomy resulting in insufficiency of contralateral adrenal hormone secretion can occur adrenal cortex crisis, and even affect the safety of patients [31, 32]. Routine hormone replacement therapy is common after CS surgery, and the duration often up to 1 to 2 years [33]. There is no consensus on the need for prophylactic sex hormone replacement therapy after adrenalectomy of SCS [34, 35]. In this study, no prophylactic hormone replacement therapy was given, and only 3 patients underwent adrenal cortex insufficiency after surgery. These patients finished hormone replacement therapy within 3 months. Moreover, adrenal insufficiency occurred in few patients, and postoperative adrenal function could be restored in a short time, which suggested that for patients with SCS adrenal adenoma, prophylactic hormone replacement therapy might not be necessary.
Perspective
In present study, we found that adrenalectomy can effectively correct hypercortisolemia, improve blood pressure, blood glucose and blood lipid, and with respect to patients with the adrenal adenoma caused by SCS, surgical treatment was recommended. There were also some limitations in this study: the general data and follow-up time of the two groups were comparable, but the time points of the follow-up data were large, and the non-prospective randomized study had more confounding factors and resulted in Diminished reliability; on the other hand, this study found no serious cases of cardiovascular accidents and deaths, which may be related to limited follow-up time, and cardiovascular accident and survival of the data on the evaluation of surgical efficacy is essential. Thus, in order to further clarify the relationship between adrenalectomy and SCS-related cardiovascular accidents and survival status, prospective randomized controlled trials and long-term follow-up are required.
Footnotes
Conflict of interest
The authors who have taken part in this study declared that they have nothing to disclose regarding funding or conflict of interest with respect to this manuscript.