
Abstract
BACKGROUND:
Lung cancer is a leading cause of death worldwide, with poor survival rates despite diagnostic and therapeutic advances. Markers are needed in order to improve clinical patient management and survival. TP53 is frequently involved in lung cancer development with polymorphic sites potentially having a role in it. This study aims to determine the value of codon 72 missense polymorphic variant genotyping, TP53 R72P, as a prognostic factor in NSCLC patients.
METHODS:
One hundred and fifteen NSCLC samples from patients exposed to tobacco smoke and silica dust from Asturias (Northern Spain) were genotyped by direct sequencing.
RESULTS:
Seventy-five percent tumour samples alleles coded for Arg. The R72P genotype was an independent predictor of lymph node status (HR
CONCLUSION:
Our results indicate a remarkable application of R72P genotyping in the clinical setting: refine patient subclassification to identify those with an adverse clinical course despite tumour free lymph node status.
Introduction
Lung cancer is the most common type of cancer and the leading cause of cancer death in men in the world. In 2012 1.8 million new cases and estimated 1.1 million men deaths occurred worldwide [1]. In Spain, lung cancer is more common in men, accounting for 17173 deaths in 2014 [2]. Asturias (Northern Spain) has the second highest age-adjusted mortality (world population) rate in the country (45.64 in 2014) [3]. Approximately 80% of patients with lung cancer are non-small cell lung cancers (NSCLC) that are further classified based on histology. Twenty-nine percent of diagnosed cases have squamous cell cancer (SqCC) and approximately 32% have adenocarcinoma (AC) [4]. Cigarette smoking is the most important causal factor for lung cancer; an estimated 90% of all lung cancer–related deaths are attributable to cigarette smoking [5]. In recent years, remarkable progress has been made in improving treatment modalities, with a shift from more general to targeted treatments depending on the molecular background of individual tumours. Treatable oncogenic alterations include mutations in EGFR and in BRAF V600E, translocations in ALK and ROS1 and, more recently, PD-L1 [6]. An analysis of advanced adenocarcinoma, conducted by the Lung Cancer Mutation Consortium, showed longer overall survival among patients with oncogenic driver mutations who received targeted therapies than among either patients with driver mutations who did not receive targeted therapies or patients without driver mutations [7]. However, despite these promising developments, this devastating disease remains the leading cause of cancer related death worldwide, nearly 20% of cancer mortality as a whole [1].
The tumour suppressor gene TP53 is activated in response to several known cellular stresses, such as genotoxic damage, hypoxia, nutritional starvation, mitochondrial biogenesis stress, ribosomal biogenesis, spindle poisons, heat or cold shock, protein unfolding problems, and oncogene activation. P53 protein acts as a transcription factor, activating genes that participate in cell cycle arrest, apoptosis or senescence. In this ways, TP53, as a tumour suppressor gene, prevents genomic instability and protects cells from tumorigenesis, reason why it has been named “The Guardian of The Genome” [8].
TP53 is the most frequently somatically altered gene in human cancer, with hundreds of different mutations described in different types of tumours, and further confirmed by recent genome-wide analyses [9]. Knowledge accumulated up to date on TP53 mutations is integrated in the IARC TP53 Database (
In the course of a larger study of TP53 mutational status in lung cancer samples from silica-exposed coal mine workers from Asturias (Northern Spain) we found a striking potential role of R72P polymorphism as a prognostic marker in NSCLC.
Material and methods
Patients and tumour samples
One hundred and fifteen patients diagnosed with either adenocarcinoma or squamous cell carcinoma of the lung between 1999 and 2013 were collected at Hospital Universitario Central de Asturias (HUCA) with institutional review board approval for guidelines on ethical procedures.
The patients were selected from HUCA tumour registry database and CAPUA Study
Characteristics of the studied patients and their tumours
Characteristics of the studied patients and their tumours
Tumour samples were obtained from neumectomy or lobectomy specimens. The diagnosis of lung tumours was based on common morphologic and immunohistochemical criteria at the time of diagnosis. Restaging according to the 7
Clinical data of the patients (age, toxic habits, silicosis, status and follow up) were obtained from both the tumour registry and HUCA patient database by trained neumologist. Histopathological data (TNM stage, type of specimen, histological type of cancer, perineural invasion and neumoconiosis) was obtained from histopathological reports of HUCA Pathology Laboratory by trained neumologist and are all shown in Table 1. As may be observed, our series is enriched in early stage tumours due to the fact that specimens were collected from surgically removed tumour samples, and thus correspond mostly to resectable cases, following clinical criteria. Time from surgery until the end of the study (2015) or until death of the patient was defined as time of survival. In case of loss of a patient for follow up, the date of the last check-up was used for calculation.
In all the cases there was a patient-signed Biobank consent accepting the use of samples for research purposes. The Tumour Bank provided fresh frozen tissue (at
Genomic DNA was extracted from 20–100 mg pieces of tumour tissue using DNAzol
HRs associated with the RP genotype for each subclassification of patients according to lymph node status, histological type, smoking history, silicosis or age
HRs associated with the RP genotype for each subclassification of patients according to lymph node status, histological type, smoking history, silicosis or age
TP53 codon 72 genotyping was performed by direct Sanger sequencing. TP53 exon 4 was PCR amplified using oligonucleotides TGAGGACCTGGTCCTC TGAC and GATACGGCCAGGCATTGAAG. Amplified DNA fragments were then sequenced usingBigDye™ terminator sequencing kits (Applied Biosy- stems). The most common allele at codon 72 in the studied series was R72 (present in 75% of the cases) and was thus taken as the reference allele.
Statistical analysis
For statistical purposes, age was dichotomized according to the median value in the series (67 years); tumour grade was dichotomized as grade 1 vs 2–3 and tumour stage was dichotomized as stage I vs II-IV.
The experimental results distributed among the different clinical groups of tumours were tested for significance employing the
Kaplan-Meier survival probability curves of patients with NSCLC according to the R72P genotype of their tumour. Homozygous patients (either RR or PP, N 
This work complied with STROBE statement [25] for dissemination of observational studies and also with reporting recommendations for tumour marker prognostic studies (REMARK) criteria [26].
Kaplan-Meier survival probability curves of patients with NSCLC stratified according to the following criteria: lymph node status (A, tumour free and B, tumour affected); histological type (C, Squamous cell carcinoma vs D, adenocarcinoma); smoking history (E, current smoker vs F, former smoker); silicosis (G, patients with silicosis vs H, patients without silicosis) and age (I, under 67 years vs J, over 67 years). For each set of patients a comparison was made between those with an homozygous R72P genotype in their tumour (either RR or PP, dotted line) and those with an heterozygous genotype (RP, continuous line). The log-rank method was used to test differences across the groups. A poorer survival rate was specifically observed for the RP genotype cases among patients tumour free lymph nodes, with squamous cell carcinomas, current smokers, patients that presented with silicosis and those over 67 years (p-values are indicated). Tick marks represent censored data.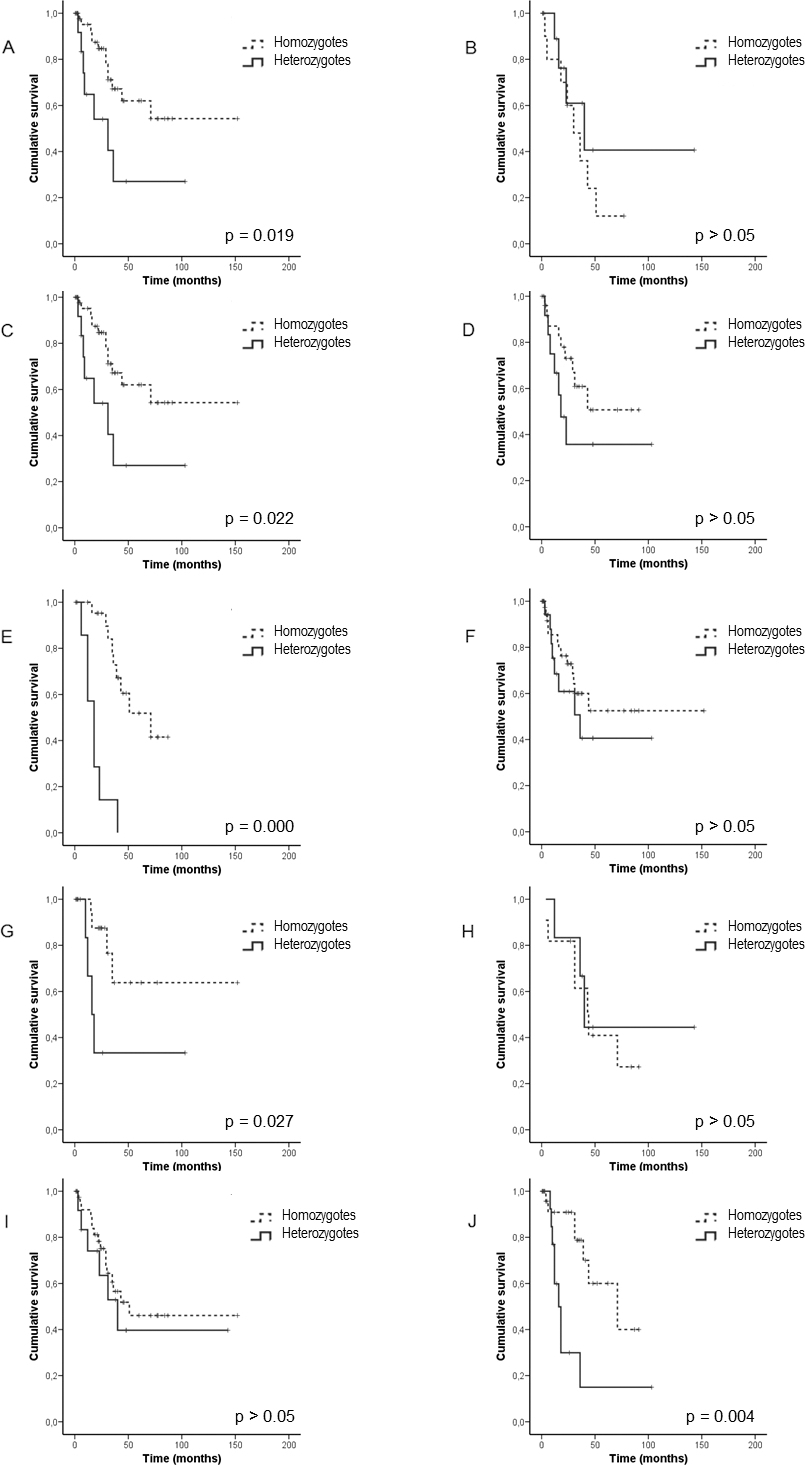
The polymorphic site genotype at codon 72 was determined in 115 tumours: 25% of the alleles (58/230) coded for the P (Pro) variant, while 75% (172/230) alleles coded for the R (Arg) variant. No difference was found for allele distribution between the histological types of tumours (squamous cell carcinoma or adenocarcinoma).
Distribution of tumours according to their genotype was as follows: 66 cases (57%) were homozygous for the Arg allele (RR), 9 (8%) homozygous for the Pro allele (PP) and 40 cases (35%) were heterozygotes Arg/ Pro (RP).
The observed 5-year survival rate of this series (44.4%) was higher than the described for lung cancer (15–20% on average). This fact can be explained by the overrepresentation of early stage tumours in this study as a consequence of resectability criteria that excludes advanced tumour stage cases from surgery.
The 5-year survival rate was significantly different (
Interestingly, the negative impact of RP genotype on survival was differentially observed in the following groups: patients with tumour free lymph nodes and not among cases with affected nodes; those with squamous type tumours but not in adenocarcinomas; current smokers, but not in former smokers group; patients with silicosis but not in non-silicotic patients and those of age over 67 but not in younger patients (Table 2 and Fig. 2).
The advanced stage tumours in our series showed, as expected, an adverse clinical course (5-year survival, 30%) compared to stage I tumours (65%) [age and smoking history (smoker vs former smoker) adjusted HR
We next investigated the relative contribution of the R72P polymorphism and relevant clinicopathological parameters (age, smoking history, tumour grade, histological type) to the lymph node status. A logistic regression model was built for this purpose. Only age under 67 yr [HR
Discussion
In this study, we have found that the TP53 R72P genotype may serve as a clinical prognostic factor in lung carcinomas. The Pro coding allele (P72) is the ancestral form, although R72 has been described to occur at a high frequency (
Our results support an adverse prognostic value for the presence of heterozygous genotype in tumour samples from lung cancer patients. The impact of RP genotype on an unfavourable outcome is specifically observed among patients with either SqCC, silicosis, tumour free lymph nodes, age over 67 years or in the smoker group and points to the need for clinical stratification of patients to take full advantage of the R72P as a marker of poor clinical course. This information could complement that provided by the adverse categories of the mentioned parameters such as histological SqCC type, advanced age and tobacco consumption. Besides cigarette smoking the studied patients had a history of silica exposure in the professional setting. Coal mining has been an outstanding activity in Asturias for decades, where silicosis is a prevalent disease. Moreover, the region has the second highest lung cancer related age-adjusted mortality rate (world population) in Spain. In this scenario, our finding of a useful role of R72P genotype as a prognostic factor among patients with silicosis takes a special relevance as it may serve to improve the clinical management of these patients. Long term exposure to silica dust triggers an inflammatory response that may lead to neumoconiosis. Molecular events involved in this process include oxygen free radicals generation, a known DNA damaging agent. We could hypothesize that the RP genotype might modulate p53 function and thus the cellular response to this noxious agent contributing to a worse disease outcome. Additionally, lymph node status merits an especial mention, due to the fact that it serves as a reference for tumour dissemination information, so that affected nodes make prognosis worse. However, among tumour free lymph node cases, the presence of the RP genotype could identify a subpopulation of patients with a poor outcome and this information could be of help in some clinical decisions regarding a more aggressive treatment choice or a closer follow up of the patients. This interesting observation is complemented by the finding pointing to the RP genotype as an independent predictor of lymph node affected status.
A previous case-control study performed also in lung cancer patients from Asturias analysed the value of the R72P polymorphism as a genetic risk factor for lung cancer development with P allele carriers presenting a statistically significant higher risk [17]. Importantly, the allelic frequencies as well as the genotypes described in such study obtained from controls and patients germline samples were similar to those found in the present study, where tumour samples were the source of DNA for genotyping. Some studies have suggested a non-random distribution of TP53 mutations and deletions in tumours, with the R allele most frequently mutated and a selection for a loss of the P allele [21]. A possible misclassification has been hypothesized to occur as a consequence of the preferential loss of the P allele in heterozygous individuals and a concern has been raised over the use of tumour derived samples as a source of genetic material for association studies [28]. According to this hypothesis we should observe a lower prevalence of the P allele in our study with tumour samples when compared to the frequency reported by Fernandez-Rubio et al. [17] with germline samples. The fact that such frequencies are so similar (0.252 in our study cases vs 0.24 in controls and 0.266 in cases in the previous one) would suggest that the proposed potential bias would not be affecting our study.
In human populations, the base change present in TP53 codon 72 is non-synonymous with an amino acid change expected to have functional consequences on the protein. Some in vitro studies have described functional differences for the R and P alleles. The RR homozygous genotype has greater apoptosis-promoting potential than the PP genotype. Mechanistically, this has been linked to differential nuclear/cytoplasmic transport of the 72R and 72P forms and localization at the mitochondrion [29]. The homozygous PP genotype displays greater transcriptional efficiency, inducing a higher level of G1 arrest than the R/R genotype [30, 31, 32]. However, these results have been reported to be tissue- and context-specific, and the in vivo relevance of these differences is not well established. Further research is needed in order to elucidate the precise capabilities of the RP genotype, but we are tempting to speculate that a possible insufficient antitumour response displayed by p53 in the heterozygous tumours could contribute to a worse prognosis. Additional effects on p53 protein function could derive from a modulating effect of such polymorphism on mutational forms of the protein as well as from interactions with polymorphic variants in upstream activators, repressors or downstream effectors of p53 [33]. A modifier effect of the R72P SNP has been reported in germline TP53 mutation carriers, in whom R72 was associated with earlier age at first diagnosis of cancer [34].
In summary, the results presented herein certainly suggest a remarkable application of R72P genotyping in the clinical setting, as demonstrated in our selected population of lung tumours from patients exposed to silica, to refine patient subclassification identifying those with an adverse clinical course despite tumour free lymph node status.
Footnotes
Acknowledgments
This work was partially financed by FIS/Spain grant numbers FIS-01/310, FIS-PI03/0365, and FIS PI06/0604. FICYT Asturias grant numbers FICYTPB02-67 and FICYT IB09-133 and grant 2015 from Fundación Caja Rural de Asturias. We thank Fundación Caja Rural de Asturias for financial collaborative support to Laboratorio de Oncología Molecular (HUCA). The Instituto Universitario de Oncología is supported by Fundación Bancaria Caja de Ahorros de Asturias, Spain. We thank Biobanco del Principado de Asturias at HUCA for providing the samples for this study. We are also very grateful to the patients who have participated in this study.
Conflict of interest
The authors declare no competing financial interests.