
Abstract
BACKGROUND:
Pancreatic cancer (PDAC) will have been the second leading cancer-related death in the United States by 2020, according to current estimation. Its late manifestation and the lack of good early detection methods are the cause of extremely low survival rates. Therefore, there is an urgent need to develop highly sensitive and specific marker. GDF-15, a member of TGFbeta family, has recently emerged as a protein playing an important role in carcinogenesis of various neoplasms.
OBJECTIVE:
Our aim was to assess the potential of GDF-15, IL-17, IL-23 serum concentration, and the panel of PDAC markers in differentiating pancreatic adenocarcinoma from chronic pancreatitis.
METHODS:
Sixty-three consecutive patients operated on due to pancreatobiliary lesions were enrolled in this study. Levels of CEA, CA125 and Ca19-9 were assessed using standard laboratory protocols. A sample of serum was collected prior to the surgery via central line. Levels of GDF-15, Il-17, Il-23 were measured using a ELISA kit. After standard pathological examination of specimens obtained on surgery, patients were divided into 2 groups: 42 patients with pancreatic adenocarcinoma and 21 patients with focal chronic pancreatitis.
RESULTS:
Mean GDF-15 concentration in patients with CP vs PDAC was 2247.95 (
CONCLUSIONS:
In conclusion, GDF-15 is more accurate than Ca19-9 in differentiating pancreatic mass due to chronic pancreatitis from pancreatic adenocarcinoma. Interleukin 17 and 23 cannot be considered as PDAC biomarkers. GDF-15 concentration in serum should be further investigated in order to assess their usefulness in pancreatic adenocarcinoma diagnosis.
Keywords
Background
It is estimated that pancreatic cancer (PDAC) will have been the second leading cancer-related death cause in the United States by 2020 [1].
PDAC is, at present, the fourth cause of cancer-related death worldwide. The lack of early symptoms and signs combined with very high aggressiveness are the factors affecting survival. Therefore, only 6% of patients survive more than 5 years after being diagnosed [2].
The probability that a patient with a detected PDAC will undergo resection which proves to be curative is 10–20% [3]. Long term survival rates have not significantly improved during the past 40 years [4].
Differentiating between malignant and inflammatory/benign pancreatic tumors remains one of the hardest quests for clinicians, as there is no 100% specific and sensitive tumor marker to discriminate between these conditions. Radiological signs of PDAC and inflammatory processes affecting pancreas are often misleading, thus the diagnosis must be based on not only on imaging studies, but on also various clinical presentation factors [5, 6]. Nevertheless, no highly accurate diagnostic algorithm has been established. As a consequence, misdiagnosis is frequent. Data from literature show that the frequency of surgery revealing inflammatory/benign lesion varies from 5% up to 26% [7, 8, 9, 10, 11]. Excised and pathologically verified tumors are proven to be mainly focal chronic pancreatitis, and some of those patients do not need extensive resection associated with significant mortality and complications. As there is no 100% specific and sensitive tumor marker to discriminate PDAC from inflammatory processes affecting the pancreas, differentiation between these lesions is still relatively hard and must be based on various clinical presentation factors and additional examinations [5, 6].
Growth differentiation factor-15 (GDF15, MIC-1) is known as a member of the transforming growth factor beta family and has been shown to play various roles in different pathological conditions such as cancer, inflammation, cardiovascular and metabolic diseases [12].
GDF-15 seems to be an important factor of carcinogenesis in many types of human cancers, including PDAC as it plays a significant part in proliferation, migration, apoptosis, and angiogenesis of cancer cells [13].
There is a strong association between pancreatic cancer and chronic inflammation. Various inflammatory cell types are involved in that process but a subset of IL-17-producing T Helper cells has been proven to be significant in both chronic inflammation [14] and inflammation-induced tumorigenesis [15]. Th17 cells differentiation requires IL-6 and TGF-
Interleukin-17A is a pro-inflammatory cytokine, expressed mainly by fibroblasts and Th17 cells [17]
Interleukin-23 is responsible for the in vitro transforming of naive T cells into Th17 cells, which produce IL-17 and plays crucial roles in the functioning and maintaining of the Th17 subtype [18].
IL-23 promotes tumor progression and induces IL-17 and IFN
The aim of our study was to assess the potential of GDF-15 serum concentration together with a panel of inflammatory regulatory cytokines and cancer biomarkers in differentiating pancreatic adenocarcinoma (PDAC) from chronic pancreatitis (CP/ Inflammatory tumor). According to our literature review, their clinical usefulness for the differential diagnostics under consideration has not been evaluated yet.
Patients characteristic and values of biomarkers in benign (CP) and pancreatic cancer group (PDAC)
Patients characteristic and values of biomarkers in benign (CP) and pancreatic cancer group (PDAC)
Sixty-three consecutive patients operated on for solid pancreatic lesions with total bilirubin level lower than 2 mg/dL at the time of surgical procedure were enrolled in this study.
The levels of CEA, CA125 and Ca19-9 were assessed using standard laboratory protocols. A day prior to surgery, a 4.9 mL blood sample was collected (Serum Z, Sarsted) and centrifuged for 10 min at 3000 rpm at 4
For statistical analysis, we used Mann-Whitney non-parametrical test to compare mean biomarker levels between groups. The same test was used in order to evaluate an association between gender and the level of biomarkers, separately for the group of PDAC patients and non-malignant patients. In the same manner, Spearman’s correlation test was applied to assess the impact of age on the levels of biomarkers.
Diagnostic performance of a single biomarker was measured by building receiver operating characteristic curves (ROC) and choosing the optimal cut-off point afterwards.
The statistical analysis was performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp. Armonk, NY) and MedCalc for Windows, version 13.0 (MedCalc Software, Ostend, Belgium).
Ethical approval for this study (Ethical Committee N
Log-transformed values of GDF-15 pg/mL in benign (CP) and pancreatic cancer group (PDAC).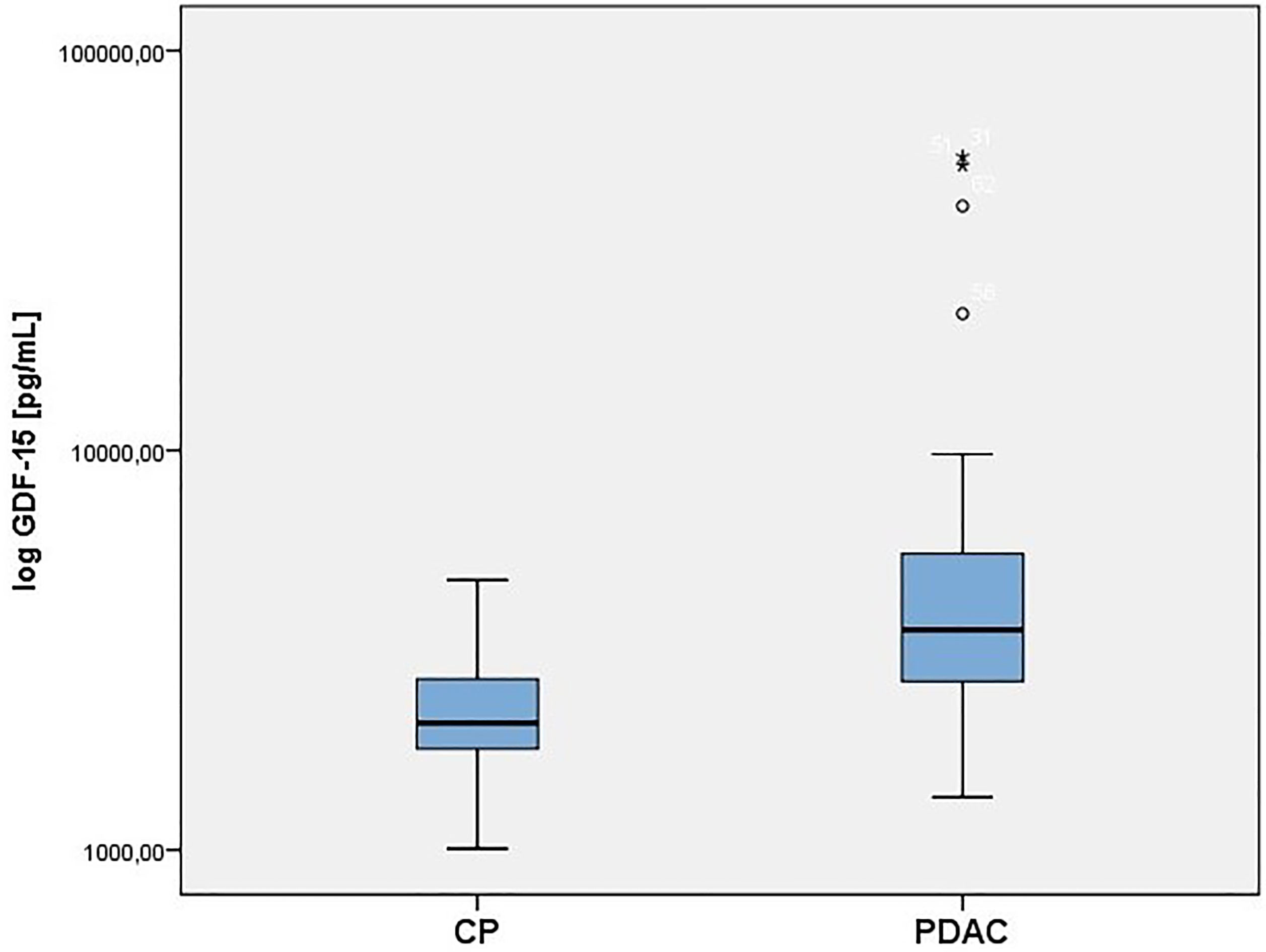
Log-transformed values of Ca19-9 IUmL in benign (CP) and pancreatic cancer group (PDAC).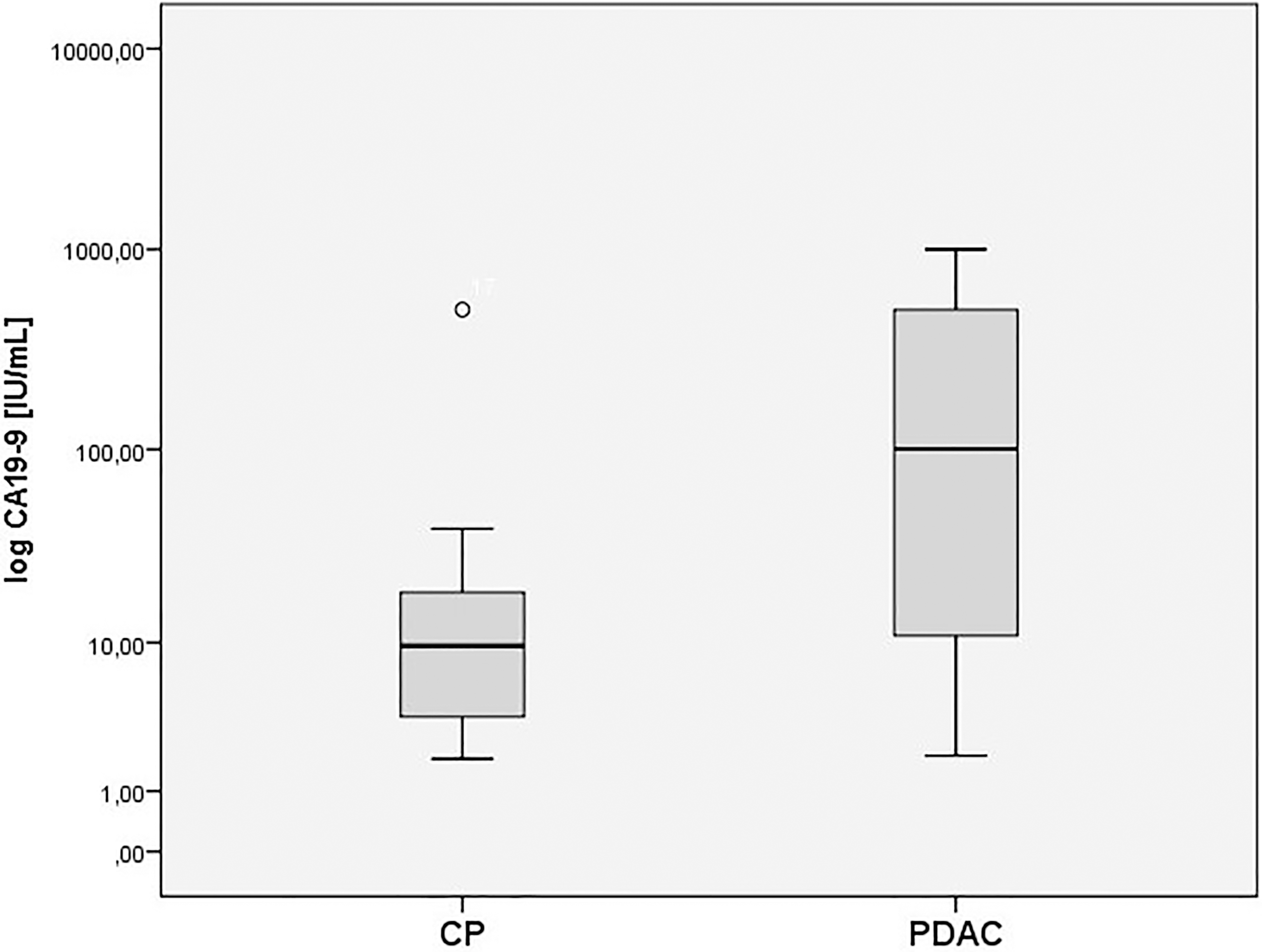
Group basic statistics are presented in Table 1. As shown, interleukins 17 and 23 cannot be considered as PDAC biomarkers, since mean levels of these cytokines as well as their distribution are almost the same in both groups. Similarly, there is no statistically significant difference in mean Ca15-3 levels. The most significant differences can be seen in mean levels of GDF-15, CA19-9, CEA and Ca125 (Figs 1 and 2). Moreover, significant correlations between GDF-15 and age (
Differences between areas under curve (AUC) of receiver operating characteristic (ROC) of single tumor markers in predicting pancreatic cancer (PDAC)
Differences between areas under curve (AUC) of receiver operating characteristic (ROC) of single tumor markers in predicting pancreatic cancer (PDAC)
Specificity, sensitivity and cut-off point of single tumor markers in predicting pancreatic cancer (PDAC)
Receiver operating characteristic (ROC) curve of single tumor markers with the optimum cut-off values in predicting pancreatic cancer (PDAC).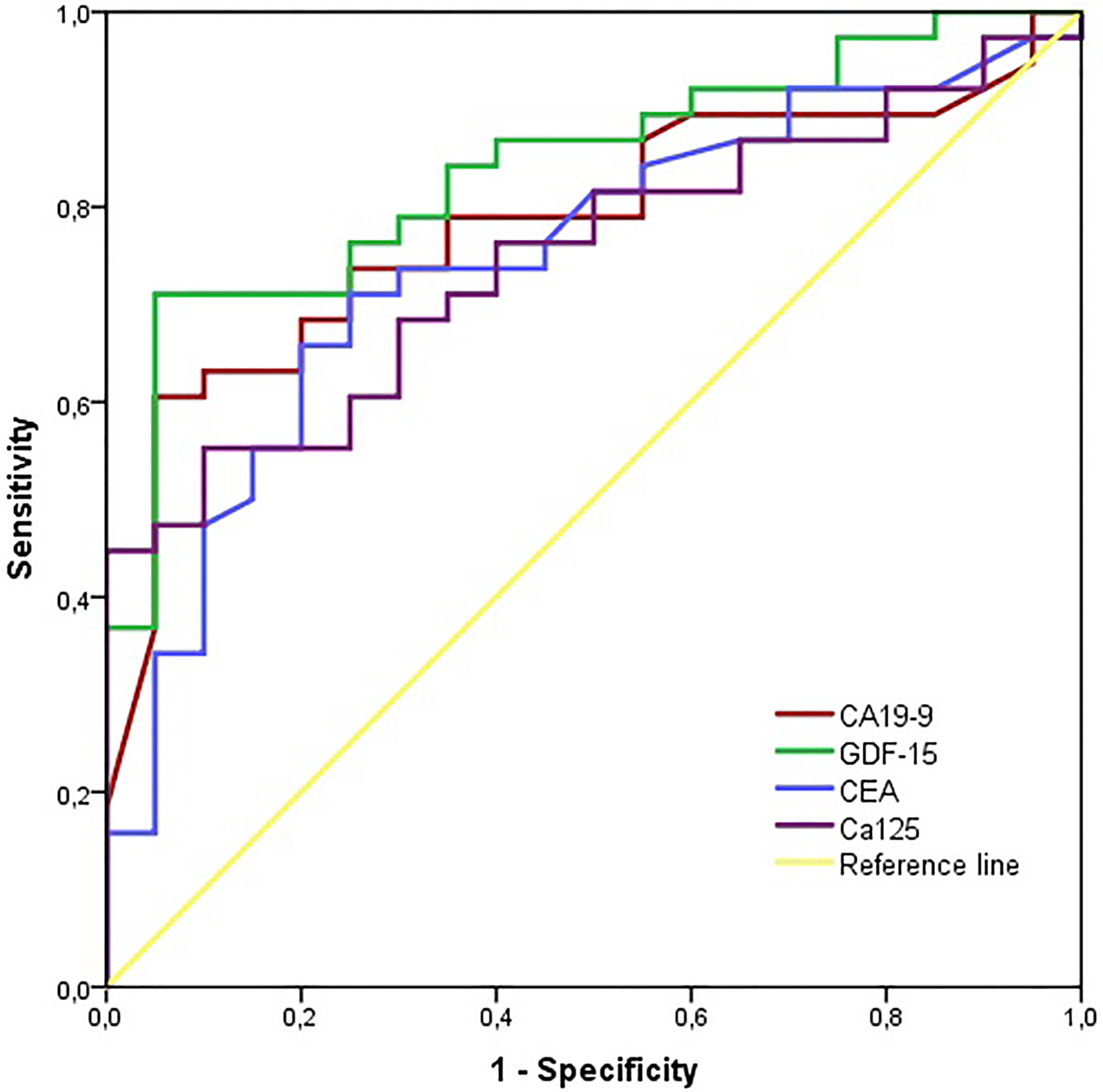
Receiver operating characteristic (ROC) curve comparing Ca19-9 and GDF-15 with the optimum cut-off values in predicting pancreatic cancer (PDAC).
Taking into account that GDF-15 did not reach exceptionally high sensitivity and specificity, we investigated whether its combination with other parameters could enhance diagnostic accuracy. We chose logistic regression model in which we applied factors such as: (i) biomarkers levels (CA19-9, GDF-15, CEA, Ca125) (ii) geneder and age (iii) platelets and white blood cells counts (iv) biologically feasible interaction terms such as CA19-9 by age or CA19-9 by Ca125 were also tested. Out of the proposed models, we chose a model including GDF-15 and Ca125, as it reached statistical significance and moderately improved diagnostic accu- racy (Fig. 4). The coefficients in our model were as follows: 0.23
In the pancreatic cancer group most of tumors were unresectable (23/42). There were 3 patients with stage IB, 7 with stage IIA, 9 with stage IIB, 9 with stage III and 14 with stage IV according to American Joint Committee on Cancer Staging Manual.
Among resectable cases in the pancreatic cancer group there were 15 pancreatoduodenectmies and 4 distal pancreatectomies performed. No significant correlation has been observed between biomarkers levels and stage of the disease.
Among various pancreatic cancer markers, CA19-9 is proven to be the only blood-based cancer biomarker in clinical use. Its specificity and sensitivity belong to the highest among other markers, but are still relatively too low for clinical utility. Around 10% of population do not express CA19-9, due to the absence of Lewis antigen [23]. Unfortunately, CA19-9 can also be elevated in patients with non-malignant diseases, including liver cirrhosis (LC), CP, cholangitis and other GI cancers [24]. Elevated levels of bilirubin may hamper Ca19-9 accuracy as a cancer marker, however bilirubin levels lover than 2 mg/dL are not associated with significant bias [25].
According to Zhang et al. meta-analysis, the CA19-9 specificity and sensitivity range around 80% [26]. The analyzed studies in the above meta-analysis differentiated PC from various other conditions. Only Liao et al., investigated CA19-9 as a marker differentiating PC from focal chronic pancreatitis causing pancreatic head mass. The clinical material and methods applied there are comparable to ours, showing CA19-9 sensitivity and specificity amounting to 75.36% and 60.60%, respectively [27]. However, the heterogeneity of patients constituting control groups in the studies evaluating CA19-9 accuracy in diagnosing PDAC makes the usefulness of this biomarker questionable in differentiating pancreatic mass in inflammatory setting.
CA125 is highly expressed, especially by late stage PDAC [28], and thus its high levels are detected in patients sera. CA125 was also reported to be able to predict PDAC resectability as well as improve CA19-9 accuracy in detecting early stage PDAC [29, 30].
The lack of highly accurate cancer biomarker leads to a urgent necessity to discover a new marker, or a panel of markers, more precise in distinguishing inflammatory tumors of the pancreas from pancreatic cancer including patients non-secreting Ca19-9.
GDF-15, also known as MIC-1, might be one of the possible candidates as the aforementioned cancer marker. It was originally described as a gene overexpressed in the activated macrophages and a member of TGF-
It is worth mentioning that the anti-cancer effect of Th17 cells has been shown alongside their pro-tumor effects. In a mouse pancreatic cancer model, Gnerlich et al. reported that some cytokines can alter the Th17/Treg balance in the tumor microenvironment. Increases in IL-6 in a TGF-
The differentiation of Th17 cells from naive T cells appears to involve signals from TGF-beta, IL-6, IL-21, IL-1beta and IL-23.
In the study of Li et al., IL-17 and IL-23 concentrations in 20 pancreatic cancer patients blood samples detected by enzyme-linked immunosorbent assay (ELISA) were 69.2
Our study did not reveal any significant differences in of Il-17 and Il-23 concentration between pancreatic cancer and chronic pancreatitis group, which may support the thesis about inflammatory manquet surrounding each pancreatic tumor, irrespective of malignancy.
Wang et al. investigated MIC-1 concentration in a cohort of PDAC, benign pancreatic tumors, CP and healthy control subjects. They found a stepwise increase in MIC-1 concentration in groups of healthy subjects, benign tumors, CP and PDAC, respectively. The authors also noticed MIC-1 (AUROC, 0.957; 95% CI 0.945–0.967) outstanding performance in distinguishing Ca19-9 negative PDAC patients from non-pancreatic carcinoma control group (CP, benign pancreatic tumors and healthy subjects). The main limitation of that study is that MIC-1 concentration was compared between PDAC and non-PDAC patients, including healthy controls. In this aspect, it is incomparable with our clinical situation – CP vs PDAC group [35].
In the paper of Kaur et al., the concentration of MIC-1 in pancreatic juice, collected endoscopically after secretin stimulation, was reported to be significantly higher among patients with PDAC and CP as compared with non-pancreatic non-healthly (patients with symptoms mimicking pancreatic disease but found to be free of pancreatic pathology). Furthermore, MIC-1 appeared to be the only marker with statistically significant difference in concentration between PDAC and CP patients [36].
As shown in our study, GDF-15 alone did not reach adequate sensitivity and specificity levels, but it was still superior to CA19-9 alone. Therefore, we investigated whether its combination with other parameters could enhance its diagnostic accuracy. Excluding Ca19-9, our model combined Ca125 and GDF-15 and proved to be 80.95% specific and 80% sensitive. If used in Lewis non-secreting group of patients, the model may improve the diagnostic accuracy in PDAC detection. Interestingly, high GDF-15 level was positively correlated with high level of other biomarkers and age. The former correlation, under certain conditions, might prove useful in creating a panel test for detecting PDAC, while the latter arises from the epidemiological situation. Namely older patients are more likely to suffer from PDAC than CP.
Our investigation also supports the notion that CA125 has clinical utility in detecting PDAC, yet its high sensitivity is limited by its low specificity. According to some studies, its concentration may be more valuable as a prognostic factor in case of PDAC patients with hyperbilirubinemia [37].
Given the calculated values of sensitivity, specificity as well as positive and negative likelihood ratios, it seems that the levels of GDF-15 combined with Ca125 are the most accurate parameters in differentiating pancreatic mass due to chronic pancreatitis from pancreatic adenocarcinoma. GDF-15 might prove useful in such cases and complement Ca19-9, especially in patients who do not express Lewis antigen and whose Ca19-9 levels are not detectable.
Conclusions
In conclusion, GDF-15 in blood is more accurate in differentiating pancreatic mass due to chronic pancreatitis from pancreatic adenocarcinoma than Ca19-9.
Additionally, the combination of GDF-15 with Ca125 is remarkably useful in differentiating pancreatic mass. Interleukin 17 and 23 cannot be considered as a biomarker of PDAC, since mean levels of these cytokines, as well as their distribution, are almost the same in both groups. Similarly, we did not find any statistically significant differences in mean Ca15-3 levels.
Footnotes
Conflict of interest
The author(s) declare that they have no competing interests.
Abbreviations
PDAC – pancreatic ductal adenocarcinoma
CP – chronic pancreatitis
GDF-15/MIC-15 – Growth differentiation factor
Il-17 – interleukin 17
Il-23 – interleukin 23
AUROC – area under receiver operating curve