
Abstract
BACKGROUND/OBJECTIVE:
Midkine (MDK) and pleiotrophin (PTN) are two closely related heparin-binding growth factors which are overexpressed in a wide variety of human cancers. We hypothesized that the concentrations of these factors in washout of biopsy needles would be higher in breast and lung cancer than in benign lesions.
METHODS:
Seventy subjects underwent pre-operative core needle biopsies of 78 breast masses (16 malignancies). In 11 subjects, fine needle aspiration was performed ex vivo on 7 non-small cell lung cancers and 11 normal lung specimens within surgically excised lung tissue. The biopsy needle was washed with buffer for immunoassay.
RESULTS:
The MDK/DNA and the PTN/DNA ratio in most of the malignant breast masses were similar to the ratios in benign masses except one lobular carcinoma in situ (24-fold higher PTN/DNA ratio than the average benign mass). The MDK/DNA and PTN/DNA ratio were similar in most malignant and normal lung tissue except one squamous cell carcinoma (38-fold higher MDK/DNA ratio than the average of normal lung tissue).
CONCLUSIONS:
Both MDK and PTN are readily measurable in washout of needle biopsy samples from breast and lung masses and levels are highly elevated only in a specific subset of these malignancies.
Background
Midkine (MDK) and pleiotrophin (PTN) are two members of the heparin-binding growth factor family which are highly expressed in multiple embryonic tissues and in many malignant tissues. MDK is a basic cysteine-rich polypeptide with a molecular weight of 13 kDa. It is expressed in multiple tissues in the mouse embryo and decreases to undetectable levels by adulthood in many tissues, including breast [1, 2, 3]. High expression of MDK mRNA has been found in various human cancers such as breast, lung, stomach, colon, liver, ovary, urinary bladder, prostate, glioblastomas, neuroblastomas and Wilms’ tumor [4, 5, 6, 7]. PTN is a related basic polypeptide with a molecular weight of 15 kDa, which is also expressed in multiple tissues of the mouse embryo and decreases with age in most tissues other than nervous tissue. PTN, like MDK, has been found to be overexpressed in various human cancers, including human breast, prostate, ovary, lung, pancreas, choriocarcinoma, melanoma, glioblastoma, and multiple myeloma [8, 9]. Both cytokines have been found to promote tumor growth, invasion and angiogenesis [10].
Both MDK and PTN act on several receptors, such as receptor-type protein-tyrosine phosphatase
We recently reported that both MDK and PTN protein levels are increased in washouts of fine needle aspiration (FNA) biopsies of malignant thyroid nodules compared to benign thyroid nodules, suggesting that measurement of these two growth factors by ELISA in FNA biopsies might provide adjunctive diagnostic and/or prognostic information to supplement current cytological and molecular approaches [17, 18]. Some prior studies suggest that MDK and PTN are overexpressed in breast and lung cancers [4, 5, 6, 7, 8, 9].
Objectives
We therefore hypothesized that tissue concentrations measured by ELISA might also be elevated in needle biopsy samples of breast and lung cancer compared to benign breast masses and normal lung. As a pilot study to test this hypothesis, we obtained washout fluid from core needle biopsies of breast masses and from ex vivo FNA lung samples and measured MDK and PTN using high-sensitivity ELISAs. To adjust for tissue content, we normalized the resulting concentrations to DNA content.
Materials and methods
Subjects and sample collection
For the study of breast cancer, subjects [
Peripheral blood (2.7 mL) was collected in a plastic citrate tube at the time of biopsy from 39 subjects with breast masses who subsequently had a histological diagnosis. The blood was centrifuged at 4
MDK/DNA ratios (A), and PTN/DNA ratios (B) in core needle biopsy washout from histologically confirmed benign (open circles) and malignant (closed circles) breast masses.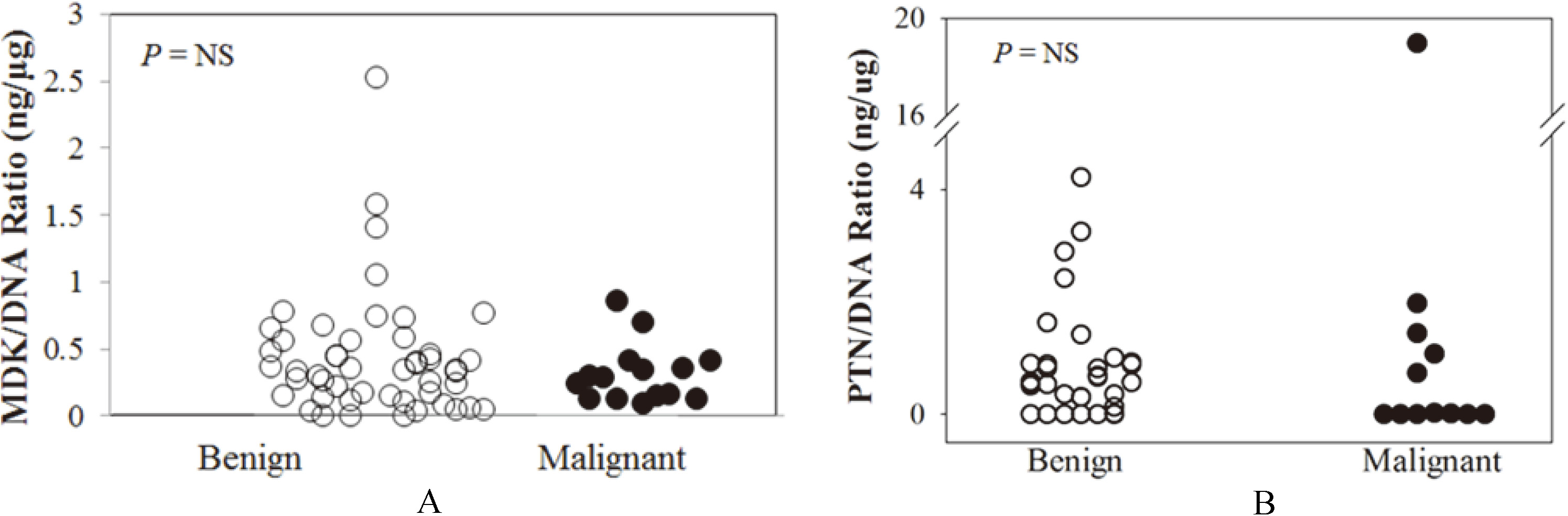
For the study of lung cancer, subjects (
Histological diagnoses were made by standard pa-thological examination. None of our subjects had heart failure or chronic kidney disease, conditions which may increase circulating MDK concentrations [19, 20, 21]. None of our subjects had known metastases.
Study protocols were approved by the WRNMMC Institutional Review Board (protocol 385478), and all patients provided written informed consent to participate in the study. The investigators have adhered to the policies for protection of human subjects as prescribed in the 45 CFR, Part 46.
MDK sandwich ELISA was performed using a commercial kit (Biovendor, Czech Republic) with modifications as previously described [11]. In summary, 50
Malignant breast masses
Malignant breast masses
IDC, invasive ductal carcinoma; DCIS, ductal carcinoma in situ; ILC, invasive lobular carcinoma; LCIS, lobular carcinoma in situ; NA, not available.
Mouse anti-pleiotropin monoclonal antibody (3B20, produced in the lab of Dr. Anton Wellstein) was diluted to 0.5
Malignancies in lung masses
Malignancies in lung masses
DNA concentration was measured using the Quant-it dsDNA HS assay kit (Life Technologies, Grand Island, NY). 20
Plasma midkine sandwich ELISA assay
125
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics, version 19. For lung masses we assayed two FNA samples and averaged the values. Samples that showed DNA concentration less than 50 ng/mL were considered to have inadequate breast or lung tissue and were excluded from further analysis. The relationship between MDK vs. DNA and PTN vs. DNA concentrations were analyzed after log transformation by generalized linear model taking into account sampling from different nodules. Histological groups were compared using the Kruskal-Wallis and the Mann-Whitney U test with Holm correction for multiple comparisons. An
Results
Characteristics of subjects and masses
For MDK measurements, core needle biopsy samples were obtained from 78 breast masses in 70 subjects (mean age, 49.1 years; all females). Thirteen masses were excluded for low DNA content. For 15 masses (14 subjects), the core needle biopsy histology was read as malignant: invasive ductal carcinoma (IDC) in 5 masses, ductal carcinoma in situ (DCIS) in 9 masses and 1 invasive lobular carcinoma. Malignancy characteristics are summarized in Table 1. Three malignant breast samples were estrogen receptor negative (ER-B23-1, B60-1, B63-1; Table 1). For 50 masses (45 subjects), the core needle biopsy histology was read as benign.
For PTN, we were only able to test 55 breast masses from 49 subjects (mean age, 51.1 years; all females) due to sample quantity. 4 masses were excluded for low DNA content. For 13 masses (10 subjects), the core needle biopsy histology was read as malignant: invasive ductal carcinoma (IDC) in 5 masses, ductal carcinoma in situ (DCIS) in 6 masses, invasive ductal carcinoa (IDC), and lobular carcinoma in situ (LCIS) in 1 mass. For 38 masses (34 subjects), the core needle biopsy histology was read as benign.
For MDK measurements, FNA samples were obtained from 7 lung nodules and 11 normal lung specimens in 12 subjects (mean age, 66.5 years; 9 males, 3 females). For all 7 nodules, the histology was read as malignant: adenocarcinoma in 4 nodules and squamous cell carcinoma in 2 nodules and mucinous adenocarcinoma in 1 nodule.
For PTN, we were only able to test 6 lung nodules in 10 subjects (mean age, 66.4 years; 7 males, 3 females) due to sample quantity. For 6 nodules, the histology was read as malignant: adenocarcinoma in 4 nodules and squamous cell carcinoma in 2 nodules. Malignancy characteristics were summarized in Table 2.
Midkine, pleiotrophin and DNA concentrations in needle biopsy washout of breast masses
The concentrations of MDK in washout of core needle biopsies were similar in malignant breast masses and benign breast masses (0.17
MDK/DNA ratios (A), and PTN/DNA ratios (B) in washout fluid from fine needle aspiration samples of normal lung tissue (open circles) and malignant lung masses (closed circles).
MDK, PTN, and DNA concentrations and MDK/DNA and PTN/DNA ratios were similar in most benign and malignant samples, except for a single high PTN/DNA ratio in the one lobular carcinoma in situ studied. MDK and DNA concentrations were significantly associated (R
The concentrations of MDK in washout of FNA was significantly different in malignant lung nodules and normal lung tissue (0.62
The concentrations of PTN in washout of FNA were similar in malignant lung nodules and normal lung tissue (0.14
Plasma midkine concentrations
Plasma MDK concentrations did not differ between subjects with malignant breast masses and those with benign breast masses (0.28
Discussion
We previously reported that the concentrations of two heparin-binding growth factors, MDK and PTN were higher in needle biopsy washouts of malignant thyroid nodules than in benign nodules [17, 18]. Because MDK and PTN are both reportedly overexpressed in breast cancer cells, we used highly sensitive ELISAs to measure MDK and PTN concentrations in the washouts of core needle biopsies from breast masses to determine whether levels differed in malignant and benign lesions. In order to correct for the amount of breast tissue present, we normalized the MDK and PTN concentration to the DNA concentration. We found that, in general, neither MDK nor PTN protein levels in core needle biopsy washout samples were significantly higher in malignant than in benign breast masses. However, one lobular carcinoma in situ showed a PTN/DNA ratio 24- fold higher than the average benign mass. Because PTN was only measured in one LCIS, it is unclear whether PTN overexpression is a general property of LCIS. We also measured MDK concentration in plasma and did not find significant differences in plasma MDK concentrations between subjects with malignant and benign masses.
Several previous studies have suggested that MDK and PTN are overexpressed in some breast cancers. In an early study, using non-quantitative RT-PCR, Garver et al. detected MDK mRNA expression in more malignant samples than in normal samples [4]. Similarly, Yu et al. found higher MDK mRNA expression in breast cancer samples than in normal breast tissue using semi-quantitative northern analysis [22], and Qin et al. reported that 86% of IDC samples showed immunohistochemical staining for MDK expression [23]. In contrast to the above studies, Miyashiro et al., using RT-PCR and northern analysis, identified MDK mRNA similarly in malignant and normal breast tissue samples, but found differential expression of a truncated form of MDK, which was identified in 6 of 26 malignant samples but not in normal breast tissue [24]. MDK expression seems to be unrelated to the level of estrogen and progesterone receptors [4].
For PTN expression in breast cancer, there are conflicting results. Fang et al. reported PTN mRNA expression in 62% of breast cancer samples but not in normal breast tissue using an RNAse protection assay [25]. In that study, the status of ER or PR was not correlated with PTN mRNA expression. However, Garver et al. found that most breast cancers and most normal breast tissue samples expressed PTN mRNA as assessed by RT-PCR. More recent microarray analysis by Turashvili et al. and by Casey et al. actually found decreased PTN mRNA expression in malignant compared to normal breast tissue [26, 27].
Because MDK and PTN are both reportedly overexpressed in lung cancer cells, we also used highly sensitive ELISAs to measure MDK and PTN concentrations in the washouts of FNA needle biopsies from ex vivo lung nodules to determine whether levels differed in malignant lesions and normal lung. We normalized the MDK and PTN concentration to the DNA concentration to correct for the amount of lung tissue present. Neither MDK nor PTN protein levels in FNA needle biopsy washout samples were significantly higher in malignant lung nodules than in normal lung tissue. However, one squamous cell carcinoma showed MDK/DNA ratio 38-fold higher than the average sample of normal lung tissue. MDK was only measured in two squamous cell carcinoma nodules, and therefore the frequency of MDK overexpression in squamous cell carcinomas is unclear.
Prior analyses have suggested that MDK and PTN are overexpressed in some lung cancers. Ostroff et al. identified PTN as a serum marker that helps identify individuals with non-small cell lung cancer [28]. Similarly, Du et al. reported significant increases in serum PTN levels of patients with lung cancer compared to controls, and, in two surgical specimens, found elevation of PTN mRNA and protein in and around non-small cell lung cancer lesions compared to normal lung tissue [29]. However, using non-quantitative RT-PCR, Garver et al. reported decreased expression of PTN in malignant lung samples compared to resected normal lung but increased expression of MDK [5]. Serum midkine levels are also reportedly elevated in patients with lung cancer [30]. In addition, there is in vitro evidence that MDK promotes lung cancer epithelial-mesenchymal transition [31] and cell migration [32], raising the possibility that those lung cancers that overexpression MDK might be treated by targeting this pathway.
Our study of heparin-binding growth factor levels in breast and lung cancer has several strengths compared to prior studies. First, unlike many previous studies, we assessed expression at the protein, rather than the mRNA level, which has greater relevance for pathogenesis. Second, unlike many older studies, we used a highly quantitative method, ELISA. The assays for both MDK and PTN are highly sensitive [17], readily allowing the detection of both MDK and PTN in the samples studied. Third, we assessed protein levels not only in serum, but directly in malignant tissues, thus potentially increasing the ability to detect increased expression.
However, the current study also has several important limitations. It is a pilot study with a small sample size of patients with breast and lung malignancies. Although we identified specific malignancies with elevated levels of heparin-binding growth factors, additional larger studies would be required to determine the frequency of this overexpression in various subtypes of breast and lung cancer, and to assess whether or not this overexpression has prognostic significance. A second limitation is that we did not have any benign lung masses available for study, and thus the only comparison was to normal lung. A third limitation is that we did not study subjects with advanced, metastatic breast or lung cancer; such subjects might have higher MDK or PTN levels, including elevated circulating MDK, as previously reported [30].
Conclusions
In conclusion, this pilot study indicates that neither MDK nor PTN concentrations in needle biopsy washout samples are higher in most malignant breast or lung masses compared to benign breast masses or normal lung, respectively. However, one lobular carcinoma in situ of the breast showed PTN/DNA ratio 24-fold higher than the average benign mass and one squamous cell carcinoma of the lung showed MDK/DNA ratio 38-fold higher than the average sample of normal lung tissue, suggesting that a subset of breast and lung cancers may strongly overexpress heparin-binding growth factors. Additional studies would be required to determine the frequency of this overexpression, whether or not it has prognostic significance, and whether these overexpressing malignancies could be treated by targeting the MDK/PTN pathways, for example with monoclonal antibodies.
Funding
This work was supported by the Intramural Research Program of the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). The views expressed are those of the authors and do not reflect the official policy of the Department of the Army, the Department of Defense or the U.S. Government.
Conflict of interest
Y.H.J and J.B. are co-inventors on a patent application entitled, “Assay to measure midkine and pleiotrophin level for diagnosing a growth” (U.S. Patent Application No. 14/646,078 – Filed: May 20, 2015), filed by the National Institutes of Health that covers the measurement of MDK and PTN in FNA samples. The authors declare that there is no conflict of interest, employment, consultancy, or products in development or modified products that could be perceived as prejudicing the impartiality of the research reported.
Footnotes
Supplementary data
Supplemental Fig. 1A. Parallelism of the MDK ELISA between the standard curve and serially diluted washout samples.
Single breast washout sample was serially diluted 5, 10 and 20 fold into assay buffer (TBSTA) and then assayed for MDK. White bars, raw MDK concentration. Black bars, measured MDK value multiplied by the dilution factor.
Supplemental Fig. 1B. Parallelism of the PTN ELISA between the standard curve and serially diluted washout samples.
Single breast washout sample was serially diluted 5, 10 and 20 fold into assay buffer (PBSTA) and then assayed for MDK. White bars, raw MDK concentration. Black bars, measured MDK value multiplied by the dilution factor.