
Abstract
Objective
This study was performed to assess the complication and diagnostic rates of computed tomography (CT)-guided transthoracic needle biopsy of pulmonary parenchymal and mediastinal lesions.
Methods
Patients who were suspected to have a malignancy based on chest imaging and CT and could not be otherwise diagnosed were evaluated.
Results
Sixty-five patients were included; 48 (73.8%) were male and 17 (26.2%) were female. Their average age was 58 years. The lesion size ranged from 11 to 105 mm. The most common specific histologic subtype was adenocarcinoma, and the least common was lymphoma. The diagnostic rate was 90.8%. The mean complication rate was 15.4%. Statistically significant associations were found between the complication rate and needle size and between the needle path length and lesion size.
Conclusion
CT-guided needle biopsy is an effective diagnostic method for patients with mediastinal and parenchymal lesions before thoracotomy. This method can also reliably differentiate benign and malignant tumors.
Keywords
Introduction
Lung cancer is one of the most common causes of cancer-related death among all types of cancer worldwide. 1 Therefore, suspected lesions should be accurately diagnosed and optimal treatment planned as soon as possible. Most lung malignancies can be confidently diagnosed with accurate histopathological identification. 2
Intrathoracic lesions are common and often difficult to diagnose. Many diagnostic techniques are used for pulmonary and mediastinal lesions, including washing and brushing cytology, transbronchial biopsy, transthoracic biopsy, thoracoscopy, mediastinoscopy, and thoracotomy. Although many of these techniques are invasive, they remain necessary to achieve an accurate histopathological diagnosis.3,4 Of these diagnostic techniques, percutaneous transthoracic biopsy is performed using either cutting needle biopsy (CNB) or fine needle aspiration biopsy (FNAB). 5
FNAB is used for cytological examination of aspirated material. CNB is used to obtain tissue fragments from the lesion for histopathological diagnosis. 4 Because a piece of tissue is taken via a cutting needle, this method is especially useful for diagnosis of suspicious malignant or benign and lymphoproliferative diseases. Additionally, it is generally more accurate than aspiration. This technique is frequently used for chest wall lesions or peripheral lesions that do not require parenchymal passage. 6 The diagnostic value of percutaneous transthoracic needle biopsy (TTNB) for malignant diseases ranges from 77% to 99%, and its sensitivity is excellent. 7
Historically, radiologists developed lesion biopsy techniques using guidance with fluoroscopy, ultrasonography, and computed tomography (CT), contributing to optimal surgical and medical management. 7 Using CT-guided TTNB, lesions in the lung parenchyma and mediastinum that are not reachable by bronchoscopy can be distinguished, and a specific diagnosis can be made with high accuracy. Thus, unnecessary performance of thoracotomy to obtain a histological diagnosis can be avoided. 6 CT-guided TTNB allows the practitioner to safely avoid vascular and cardiac structures when sampling almost all lesions. CT-guided TTNB is an easy technique that induces less trauma than thoracotomic biopsy techniques. 8 The complication and diagnostic rates of CT-guided TTNB are affected by many factors, including the needle depth, needle size, and distance from the lesion to the pleura. 9
The purpose of this study was to investigate the technique, suitability, and factors influencing the diagnostic and complication rates of CT-guided TTNB of lung masses.
Materials and methods
In this retrospective study, we assessed 65 patients who underwent CT-guided lung biopsy using a fine needle and a cutting needle. The diagnostic studies were performed during a 4-year period in the Department of Radiology, Ankara Numune Training and Research Hospital, Ankara, Turkey. This study was approved by the ethics committee of the same institute. Written informed consent was obtained from all patients.
Patients who were suspected to have malignant lesions on CT images and chest radiographs that were unspecified by other methods were evaluated. TTNB was performed under CT guidance. We used a CT Scanner (Hitachi Radix Turbo Model; Hitachi Medical, Tokyo, Japan) to guide the needle and locate the lesion.
Patients with significant coagulopathy, contralateral pneumonectomy, bullous disease adjacent to the suspicious lesion, pulmonary arterial hypertension, and advanced chronic obstructive pulmonary disease were excluded from the study.
The CT images were evaluated before the procedure, and the patient was positioned based on these images to provide the safest distance from the skin surface to the lesion. Each patient was informed about the procedure and was asked to maintain the initial position during the procedure. A metal marker was then used to indicate the estimated lesion area according to the scanned images, and this area was rescanned using a 5-mm slice thickness for confirmation. The depth of the lesion and the angle of needle entrance were calculated. The selected section was marked on the patient. The upper side of the costal margin was used for needle entrance to protect the neural and arterial structures. The skin was cleaned, and subcutaneous and intradermal anesthesia was performed with 2% prilocaine (Citanest; Dentsply, York, PA). We used 20-cm-long, 22-gauge Franseen lung biopsy needles (Cook Medical, Inc., Bloomington, IN) for the aspiration biopsies and 15-cm-long, 18-gauge Franseen biopsy needles (Cook Medical, Inc.) for the cutting biopsies. The patient was told to hold his or her breath, and the needle was lowered to the specified depth after ensuring that no deviations due to patient motion had taken place. The patient was then told to take superficial breaths, and several control scans were taken from that area. After ensuring that the needle tip was in the lesion, the mandrel of the needle was removed. The needle was wiggled within the lesion to free it, and aspiration was then performed. When we judged that enough material had been obtained, the needle and injector were withdrawn. Both hands were used for this procedure to terminate the negative pressure. The puncture site was covered with sterile gauze. The aspirate of FNAB was sprayed to lam, and the tissue specimen of CNB was placed into 10% formalin solution and sent out for pathological examination. A single entry was performed to reduce the complication rate.
Upon completion of the biopsy, the patient was examined by CT for rule out pneumothorax and hemorrhage. The patient was then sent to the clinics for further follow-up.
Percentage of lesions in each group according to histopathological diagnosis.

Statistical analysis
Demographic characteristics, history, histopathologic diagnoses, complication rates, and radiologic data were recorded for all patients. Pearson’s chi-square test was used to assess the data. The results are reported as either percentage or mean ± standard deviation. A P value of < 0.05 was considered statistically significant.
Results
In total, 49 lesions in 65 patients underwent CT-guided transthoracic FNAB, and the remaining 16 lesions underwent CT-guided transthoracic CNB. Lesion access was achieved at the first needle pass in all cases. Of the 65 patients, 48 (73.8%) were male and 17 (26.2%) were female. The patient age ranged from 20 to 80 years for male patients and from 11 to 78 years for female patients. The median age was 58 years (65.4 ± 10.7 years).
The mean lesion size was 36 mm (range, 11–105 mm; 54 ± 19 mm). The mean distance from the margin of the lesion to the pleural surface was 21 mm (range, 0–53 mm; 23 ± 12 mm). The mean distance from the skin to the center of the lesion (needle path length) was 48 mm (range, 0–91 mm; 53 ± 21 mm).
The histopathologic results from all biopsies were classified into the five above-mentioned groups (Table 1). Table 1 also shows the percentage of lesions in each group according to the histopathological subtype. The histopathological diagnoses were defined in 59 of 65 (90.8%) patients: 72.4% had malignant lesions and 18.4% had benign lesions. In six patients, histopathological analysis was not informative because of inadequate samples. The histopathological results in patients with malignancies included non-small cell carcinoma and malignant epithelial lesions (21.6%), lung adenocarcinoma (16.9%), squamous cell carcinoma (12.3%), metastatic disease (10.8%), small cell carcinoma (6.2%), lymphoma (3.1%), and pleomorphic carcinoma (1.5%).
Factors influencing diagnostic and complication rates.
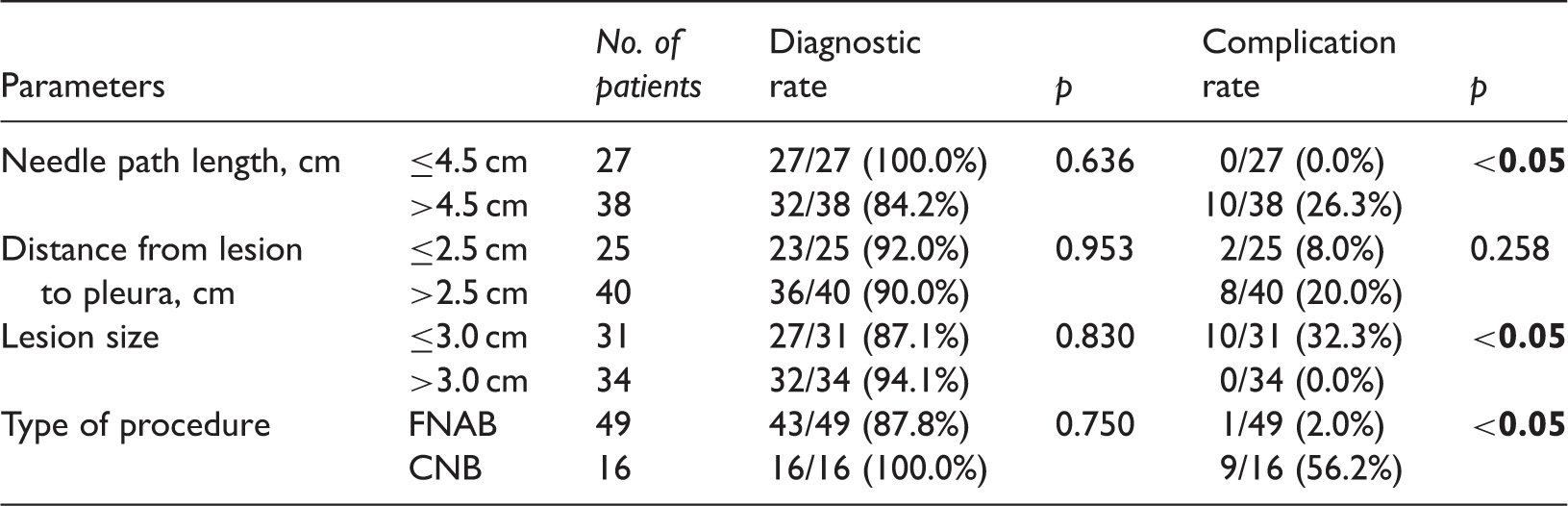
FNAB, fine needle aspiration biopsy; CNB, cutting needle biopsy
Post-procedure pneumothorax developed in 10 (15.4%) of all 65 patients as shown by the CT examination performed after the biopsy. None of these patients required chest tube placement. Pneumothorax occurred in 4 (6.2%) of all 65 patients as shown by the post-biopsy chest X-ray taken 3 hours later. Minor intraparenchymal bleeding occurred in 7 (10.8%) patients as shown by CT after the procedure. No hemoptysis or hemothorax was seen.
Discussion
Lung cancer is the most common cancer in men and the second most common cancer in women that causes mortality. 1 Therefore, suspected lesions should be diagnosed as soon as possible. When a lesion is seen in the lung, the first step is to determine whether the mass is benign or malignant. Microbial analyses and histopathologic specimens should provide the final diagnosis, regardless of whether a mass is considered malignant or benign based on chest imaging as your proposal. Many methods have been described for diagnostic sampling of intrathoracic lesions.9,10 Of these, the sensitivity of bronchoscopy and transbronchial biopsy are high for endobronchial lesions and low for peripheral lung lesions. For pulmonary nodules, CT-guided needle biopsy is an effective technique with which to confirm the pathological diagnosis. This technique has been analyzed with respect to factors that affect its diagnostic and complication rates.10,11
The indications for CT-guided TTNB include consolidation, abscesses, mass lesions, pulmonary nodules, pleural lesions, and hilar and mediastinal masses that cannot be definitively diagnosed by sputum cytology or bronchoscopy. 12 In current practice, CT-guided TTNB is the gold standard method for the diagnosis of intrathoracic lesions. Easy and rapid application and the lack of a requirement for general anesthesia are the main advantages of CT-guided TTNB over bronchoscopy and video-assisted thoracoscopic biopsy. 13
The reported accuracy rate of CT-guided TTNB varies from 77% to 99%. 14 In the present study, the diagnostic rate of CT-guided TTNB was 90.8% (72.4% for malignant lesions, 18.4% for benign lesions). Diagnosis was successful in 59 of 65 patients. A specific result could not be achieved in all patients who underwent CT-guided FNAB (43/49, 87.8%), whereas a specific histopathologic diagnosis was obtained in all CT-guided CNB procedures (16/16, 100.0%). This result is similar to the findings reported in previous publications. However, this difference was not statistically significant in the present study.
Loubeyre et al. 15 studied 75 patients and reported that a specific histopathological diagnosis with a low complication rate could be achieved with CT-guided CNB. Wallace et al. 16 examined the efficacy of CT-guided FNAB for ≤1.0-cm pulmonary lesions. CT-guided transthoracic FNAB was applied to 61 cases with a <1-cm lesion on CT. The diagnostic rate was 77% (52% for malignant lesions and 25% for benign lesions). In another study, 296 patients underwent core biopsy, FNAB, or both for lung lesions. FNAB was diagnostically helpful in 91.7% and core biopsy in 87.8% of patients in the malignant group. This rate increased to 96.6% when the two methods were combined. 17
The present study included 48 (73.8%) men and 17 (26.2%) women; the male:female ratio was 2.8:1.0. This particular ratio occurred because malignant pulmonary lesions are seen more commonly in males than in females. This is also consistent with the literature.
Malignant histopathological diagnoses included non-small cell carcinoma and malignant epithelial lesions (21.6%), lung adenocarcinoma (16.9%), squamous cell carcinoma (12.3%), metastatic disease (10.8%), small cell carcinoma (6.2%), lymphoma (3.1%), and pleomorphic carcinoma (1.5%). The histologic distribution of lung cancers has changed throughout the years. In past decades, epidermoid carcinoma constituted 50% of lung cancers, and this rate is now lower. Conversely, the proportion of adenocarcinomas has increased, whereas that of small cell cancers has decreased. 4 In the present study, the most common specific histologic subtype was adenocarcinoma and the least common was lymphoma. These findings are consistent with some studies performed by other authors.4,5,11,18
A statistically significant relationship was found between the complication rate and lesion size (p < 0.05), needle path length (p < 0.05), and type of biopsy procedure (p < 0.05). Pneumothorax was the most common complication, but the rate of this complication (15.4%) is within the acceptable level and is even low according to the range reported in the literature (9.0%–59.6%).19,20 A main consideration of lung biopsy-associated pneumothorax is whether it is pleural or non-pleural. Aribaş et al. 21 found that the lesion depth was a poor predictor of pneumothorax. Accordingly, in previous series of CT-guided biopsy in the literature, pleural lesions were associated with a very low incidence of pneumothorax; as soon as the aerated lung was traversed, the risk rose considerably. However, the exact depth of the lesion was not a significant factor. In the present study, we found that the depth of the lesion, rather than whether the lesion was pleural or non-pleural, was a significant risk factor for complications.
The next most common complication was minor intraparenchymal hemorrhage (6.2%). None of the patients required chest tube insertion. No hemoptysis or hemothorax occurred. The low rate of pneumothorax in the present study might have been related to the single entry, the choice of different types of needles according to the size and location of the lesion, and the fact that the patients held their breath and avoided coughing. All patients underwent non-contrast CT scans immediately after the needle was removed, followed by a chest X-ray 3 hours later. If air was seen in the pleural space, pneumothorax was diagnosed. Some authors have reported lower complication rates in association with CNB and higher complication rates in association with FNAB, while others have reported the reverse situation. 17 Topal and Berkman 18 found that the rate of pneumothorax was not affected by the needle size in their retrospective study of 284 cases. Anderson et al. 9 reported a 15.9% rate of pneumothorax when performing CNB and 35.1% when performing FNAB. However, some studies have revealed higher rates of pneumothorax with larger needle diameters. 22 We used 22-gauge, 20-cm Franseen lung biopsy needles for the FNAB and 18-gauge, 15-cm Franseen biopsy needles for the CNB. A statistically significant relationship was found between the needle size and complication rate. The distance from the lesion to the pleura was not significantly associated with the complication rate.
The following four factors also had no significant effect on the diagnostic rate: needle size, lesion size, distance from lesion to pleura, and needle path length. There is a consensus in the literature regarding the use of 18-gauge cutting needles for outlying lesions and 20-gauge needles for deeper lesions.23,24
Overall, the diagnostic yield in our study was 90.8%. The diagnostic and complication rates were found to be consistent with the results reported in the literature. Limitations of this study include the retrospective study design, low number of patients, and low number of evaluated parameters. It is evident that CT-guided TTNB is a reliable method with a low complication rate and high diagnostic rate for lesions that cannot be diagnosed by clinical and radiologic methods. CT-guided TTNB is also highly sensitive for differentiation between malignant and benign lung masses, and it reduces the need for more invasive procedures. We believe that its accuracy will further increase for early thoracic lesions because of continued advances in CT technology and increased experience of radiologists and cytopathologists.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.