
Abstract
BACKGROUND:
The intrinsic foot muscles play an important role in medial longitudinal arch support, as well as several extrinsic foot muscles. While various strength training methods specific to intrinsic foot muscles have been conducted, these exercises are associated with certain concerns regarding their effectiveness and difficulty. We developed a new exercise for the intrinsic muscles (MTP flexion exercise).
OBJECTIVE:
The aim was to compare the shear modulus of the toe flexors as the muscle contraction activity during MTP flexion and short-foot exercises using ultrasound shear wave elastography.
METHODS:
Eleven healthy participants were included in this study. The shear modulus of the toe flexor muscles was measured during MTP flexion and short-foot exercises using ultrasound shear wave elastography. The muscle shear modulus was statistically compared between the resting phase, and during the two exercises.
RESULTS:
The shear modulus during MTP flexion exercise was significantly greater than in the resting phase in the abductor hallucis, flexor hallucis brevis, flexor digitorum brevis, quadratus plantae, and flexor digitorum longus. The flexor digitorum longus showed greater shear modulus during MTP flexion exercise than during short-foot exercise.
CONCLUSION:
MTP flexion exercise showed equivalent or greater contraction activity in certain intrinsic and extrinsic foot muscles when compared with short-foot exercise. This exercise is considered one of the training options for strengthening the intrinsic muscles of the foot.
Introduction
The intrinsic muscles of the foot play an important role in dynamic support of the longitudinal arch of the foot [1]. These muscles are considered local stabilisers in the active subsystem of the foot core theory [2].
Several methods are used to strengthen the intrinsic foot muscles, including toe towel curls, picking up objects, shin curls, unilateral balance activities, and short-foot exercises [3]. Recently, systematic reviews and meta-analyses have revealed the effectiveness and superiority of short-foot exercises for plantar intrinsic foot muscle training [4, 5, 6]. This exercise is believed to improve foot alignment, medial longitudinal arch function, foot muscle strength, and static and dynamic balance. Short-foot exercises have been applied to patients and athletes with foot dysfunction or sports-related problems, such as flatfoot, chronic ankle instability, or patellofemoral pain [7, 8, 9]. However, short-foot exercises are difficult to perform [10].
The anatomical insertions of the extrinsic and intrinsic muscles of the foot are different, resulting in variations in toe flexion patterns [11]. Contraction of the flexor digitorum longus (extrinsic muscle) flexes the interphalangeal (IP) joints and metatarsophalangeal (MTP) joints, while the distal interphalangeal joint remains extended by contraction of the flexor digitorum brevis (intrinsic muscle). Contraction of the interossei and lumbrical (intrinsic muscle) flexes and extends the IP joints [11]. In the hand, this position (metacarpophalangeal joint flexion and IP joints extension) is known as ‘intrinsic plus position’ [12]. A previous study reported that the flexion method affected the activities of the toe flexor muscles and that MTP joint flexion without IP joint flexion was more effective for the intrinsic muscles of the foot [13]. Based on these findings, we developed a new exercise for the intrinsic muscles of the foot (MTP flexion exercise). The concept of this exercise involves resistance muscle training in the intrinsic plus position and is easy to perform.
Ultrasound shear wave elastography was developed as a technique for quantifying the stiffness of the tissue. This is a non-invasive method to measure the shear modulus of muscles. A handheld ultrasound probe induces shear waves in soft tissues using acoustic force. The probe determines the shear modulus (in kPa) by analyzing the propagation velocity of shear waves [13]. Several studies have reported that muscle shear modulus during contraction is closely related to the contraction intensity and electromyography [14, 15, 16].
Therefore, this study aimed to compare the shear modulus of the toe flexors as the muscle contraction activity during MTP flexion and short-foot exercises using ultrasound shear wave elastography.
Methods
Study design
This is a crossover study, where healthy participants served as their own controls, performing both MTP flexion and short-foot exercises in a repeated measures design. Muscle contraction activities were measured using ultrasound shear wave elastography for each participant during both exercises.
Participants
The study included 11 healthy university male students (mean age, 22
Interventions
MTP flexion exercise
MTP flexion exercise. (a) exercise for the hallux, (b) and (c) exercise for the lesser toes. The participants were instructed to perform isometric MTP joint flexion without IP joint flexion.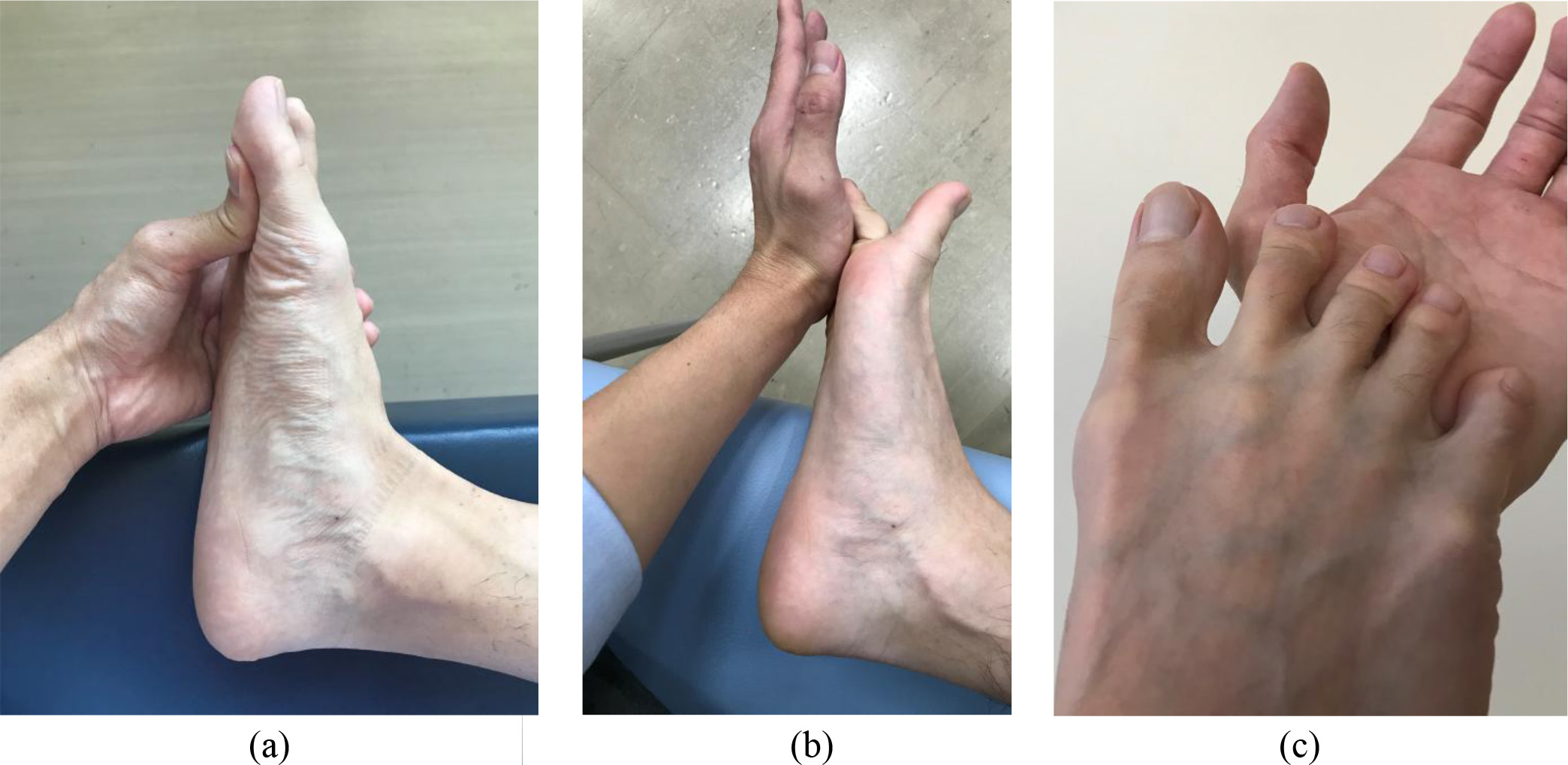
The participants were instructed to sit on the bed The leg and foot to be used during exercise and imaging was placed with the hip flexed, abducted, and the knee flexed. The ankle was neutral in the sagittal plane. The participants performed isometric MTP joint flexion by applying manual resistance to their toes. The examiner instructed the participants to flex the MTP joint without IP joint flexion. The hallux and lesser toes were assessed separately (Fig. 1).
Short-foot exercise. The participants were instructed to shorten the foot in the anterior-posterior direction by attempting to bring the head of the first metatarsal toward the heel without toe flexion (indicated by the black arrow) and to raise the medial longitudinal arch (indicated by the dotted arrow). The foot was positioned on a wooden board with an opening at the longitudinal foot arch. Shear wave elastography images of the plantar muscles were obtained by placing the probe on the plantar foot surface through the opening in the board.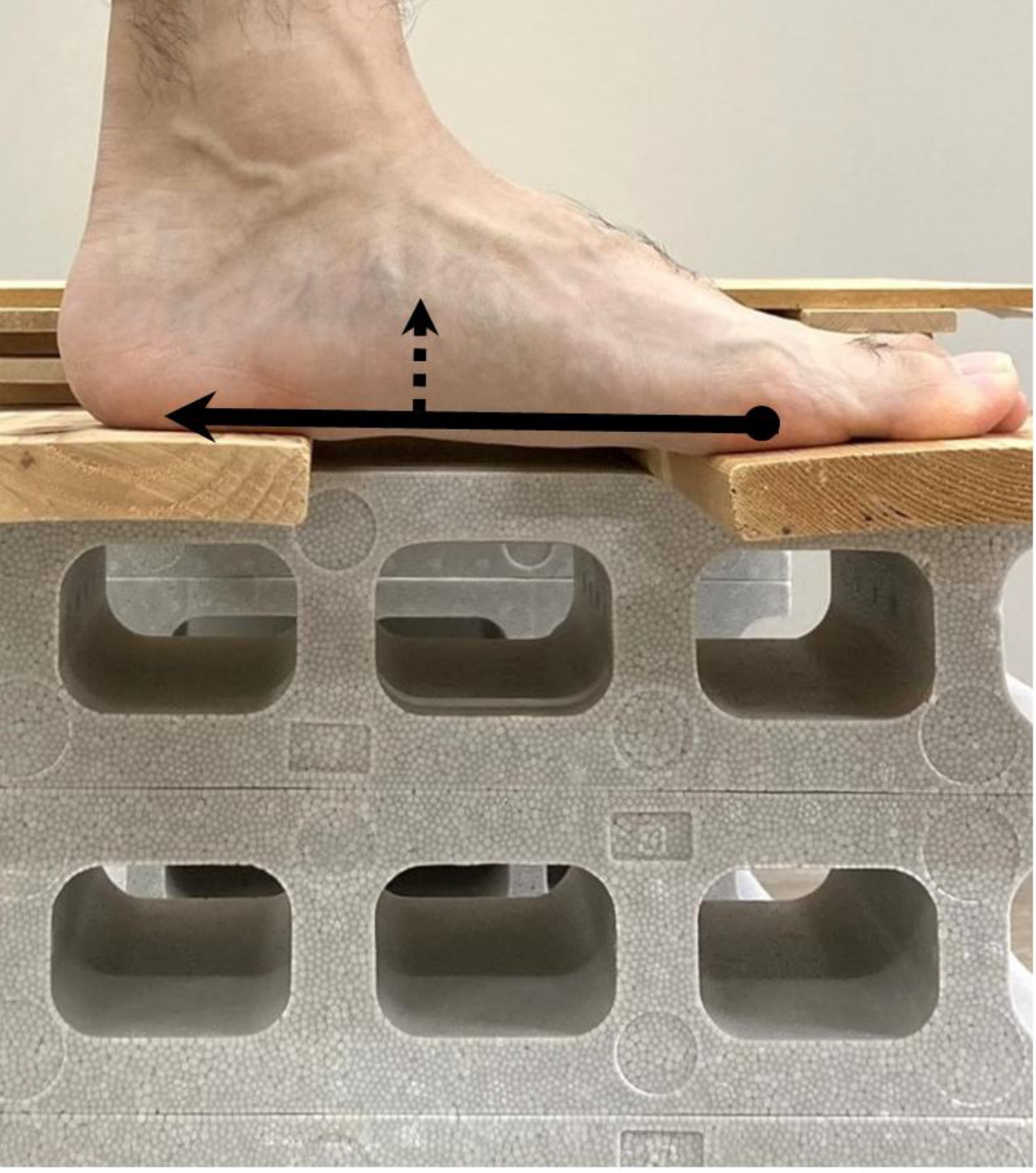
The participants were asked to shorten the foot in the anterior-posterior direction and actively attempt to bring the head of the first metatarsal toward the heel and raise the medial longitudinal arch without toe flexion. The forefoot and heel were kept on the ground during short-foot exercise [3] (Fig. 2).
The participants were allowed practice trials, after which the data from the two trials were collected. The participants performed these two exercises randomly, and the measurements for each muscle, as described below, were also taken randomly. They took a 5-minute break between the exercises.
The muscle shear modulus was measured according to the method described in a previous study [13, 19]. Ultrasound shear wave elastography (Aixplorer, SuperSonic Imagine, France) with a 2–10 MHz linear probe was performed to measure the shear modulus of the abductor hallucis (AbdH), flexor hallucis brevis (FHB), flexor hallucis longus (FHL), flexor digitorum brevis (FDB), quadratus plantae (QP), and flexor digitorum longus (FDL) muscles.
Regarding the location of the probe, the AbdH was measured on a scanning line between the origin of the muscle in the medial calcaneal and navicular tuberosities in the longitudinal section. The FHB was measured longitudinally along the shaft of the first metatarsal at the thickest portion of the muscle. The FDB and QP were measured longitudinally along a line from the medial tubercle of the calcaneus to the third toe. The FDL was imaged at 60% of the distance between the medial tibial plateau and inferior border of the medial malleolus on the medioposterior aspect of the tibia. The FHL was measured at 60% of the distance between the fibular head and inferior border of the lateral malleolus on the posterolateral aspect of the fibula [13, 19].
Shear wave elastography image and measurement of Young’s modulus. This image shows the abductor hallucis. The Young’s modulus in the area of interest enclosed in the square is displayed using color mapping. Three circled areas are set within the area of interest and the average Young’s modulus in each circle is measured in kPa. The average value of the 3 areas is set as the Young’s modulus for each image.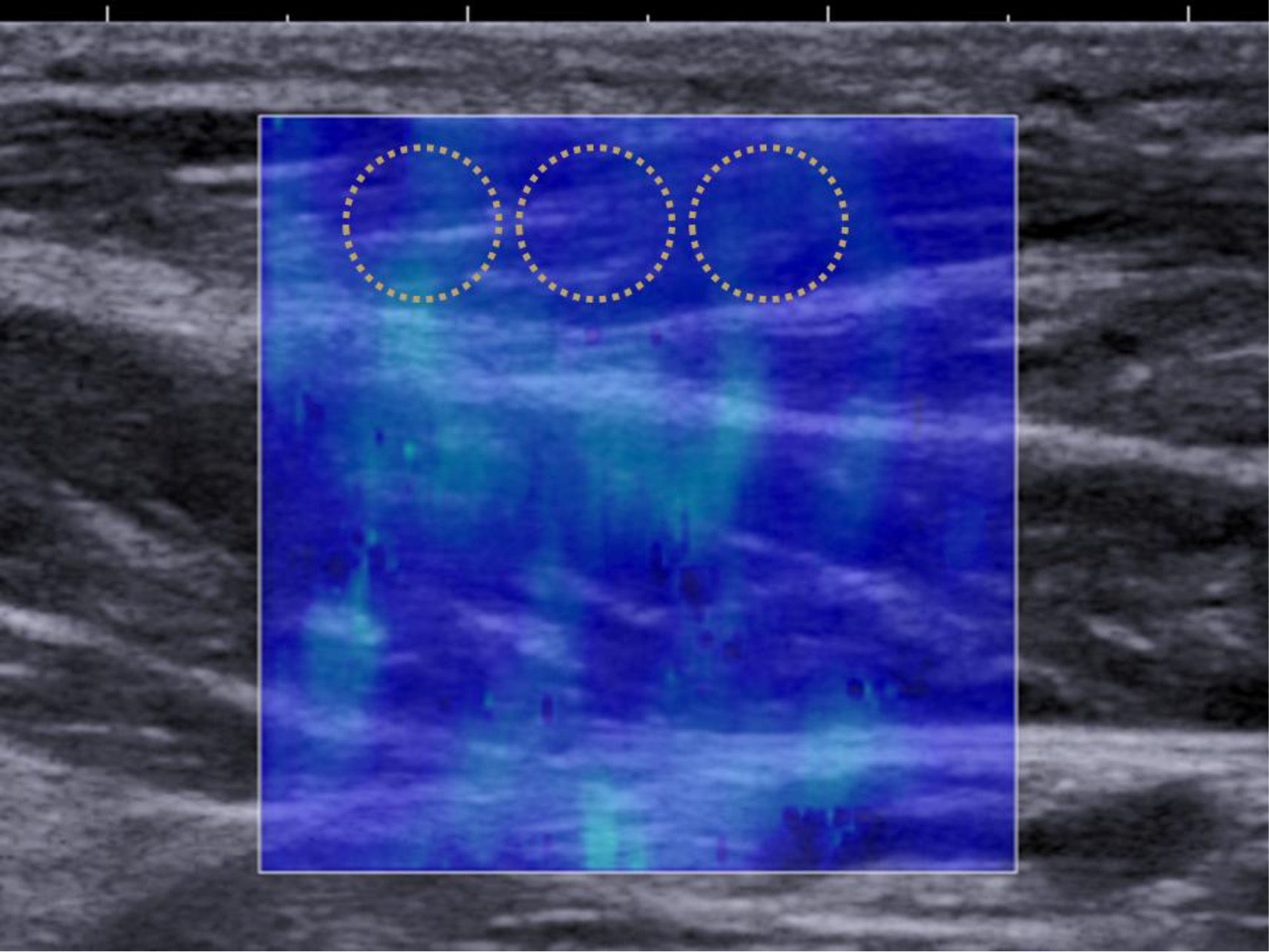
Shear wave elastography images were captured twice in the resting phase, and during MTP flexion and short-foot exercises. Three areas were circled in the relevant regions of the obtained images, and the average Young’s modulus for each circled area was measured using Q-Box software with the ultrasound system [13]. The average value of the three areas was used as the Young’s modulus for each image (Fig. 3). The shear modulus was calculated in this study by dividing the obtained Young’s modulus by 3 [13]. The average value of the two images obtained under all conditions was used in the analysis. The measurements were conducted by a single examiner (KH).
All statistical analyses were performed using statistical software (SPSS Statistics 22.0, IBM Corp, Armonk, NY, USA). A repeated measures ANOVA was used to compare the muscle shear modulus between the resting phase, and during MTP flexion and short-foot exercises. The Bonferroni post-hoc test was performed. A
Results
The muscle shear modulus measurements are shown in Fig. 4 and Table 1. The shear modulus of the AbdH and FHB muscles was significantly greater during MTP flexion exercise and short-foot exercise than in the resting phase (AbdH,
Mean values of muscle shear modulus and comparison among resting phase, MTP flexion exercise, and short-foot exercise. (Standard deviations in parentheses)
Mean values of muscle shear modulus and comparison among resting phase, MTP flexion exercise, and short-foot exercise. (Standard deviations in parentheses)
Muscle shear modulus during the resting phase, MTP flexion exercise, and short-foot exercise. (a) abductor hallucis (AbdH), (b) flexor hallucis brevis (FHB), (c) flexor hallucis longus (FHL), (d) flexor digitorum brevis (FDB), (e) quadratus plantae (QP), (f) flexor digitorum longus (FDL). * P< 0.05. MTPF, MTP flexion exercise; SF, short-foot exercise.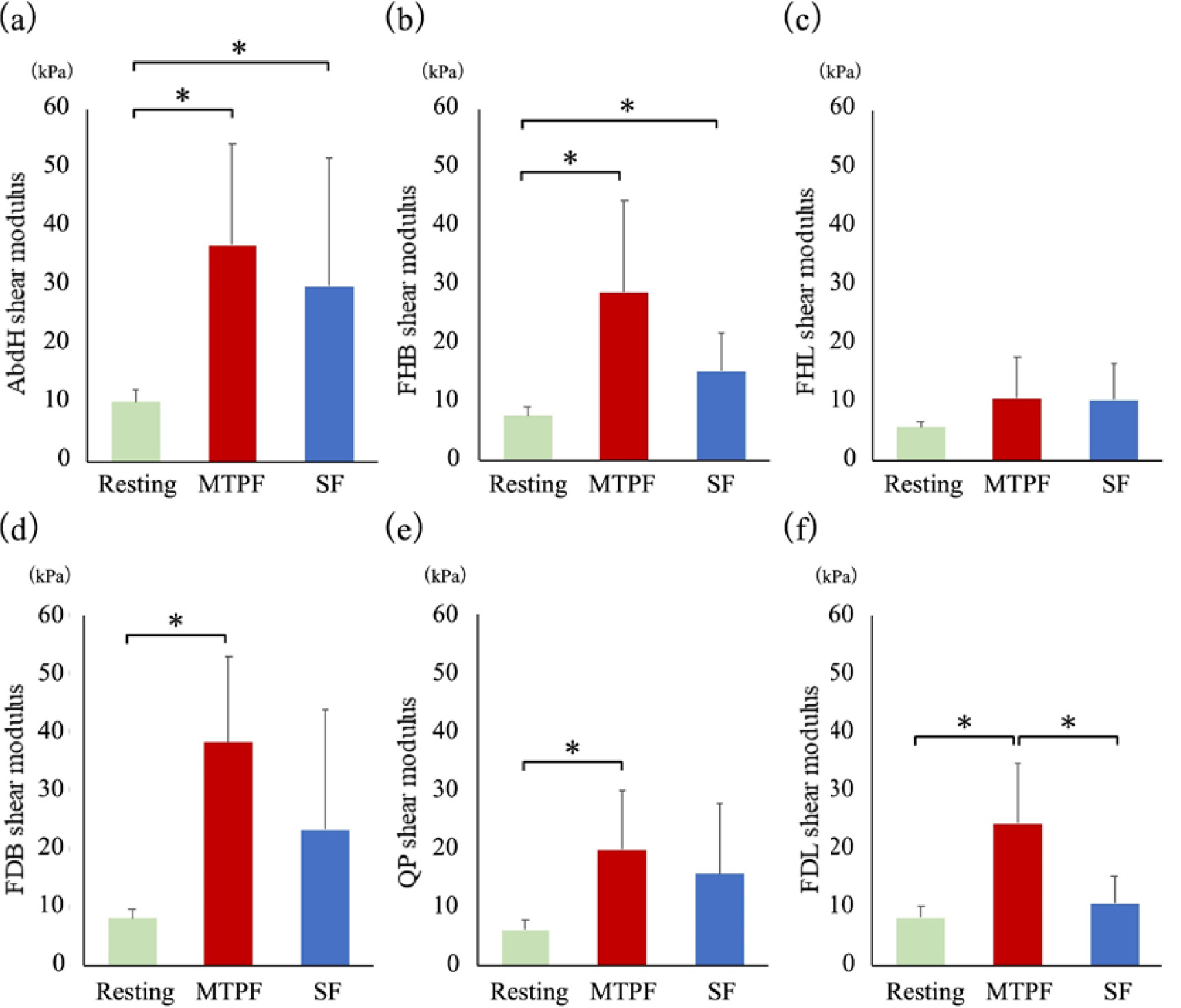
This study showed that the shear modulus during MTP flexion exercise was significantly greater than in the resting phase in the investigated muscles, except the FHL muscle. Furthermore, the FDL muscle exhibited a greater shear modulus during MTP flexion exercise compared to both the resting phase and short-foot exercise. The shear modulus during muscle contraction has been reported to positive correlate with the contraction intensity and activity in various muscles such as shoulder muscles [14], the biceps brachii [15], gastrocnemius [20], and quadratus plantae of the foot [17]. Our data suggested that MTP flexion exercise could induce equivalent or higher contraction activity in the investigated muscles than short-foot exercise.
Short-foot exercise is one of the most commonly used intrinsic foot muscle exercises, and its effects have been investigated in the basic [3, 18] and clinical studies described above. During this exercise, the toes push the floor by slightly flexing the MTP joints with IP joint extension. This position is similar to MTP flexion exercise and both exercises induce the isometric contraction of the toe flexor muscles. The activity of the AbdH muscle, as evaluated by electromyography, was significantly greater during short-foot exercise than during toe curl exercise, which is also widely used for toe flexor strength training [3]. A magnetic resonance imaging study compared plantar intrinsic muscle activation among four types of foot exercises (short-foot exercise, toes spread out, first toe extension, and second to fifth toe extension) [18]. All evaluated muscles (the AbdH, FHB, FDB, QP, abductor/flexor digiti minimi, adductor hallucis oblique, interossei, and lumbricals) showed increased activation after all exercises, especially the short-foot exercise and toes spread out.
Resisted flexion of the toes in the position of MTP joint flexion and IP joint extension should facilitate plantar intrinsic muscle activity [13], while the long toe flexors are less activated. The short-foot and MTP flexion exercises are performed in this position. Garth et al [21] described this position as an “intrinsic positive pattern”. The extrinsic muscles, FHL and FDL, are inserted into the distal phalanx and are responsible for the flexion of the IP joint. In contrast, intrinsic muscles, such as the FHB, AbdH, and FDB, flex the MTP joint, and the lumbrical muscle flexes the MTP joint while extending the IP joint [11]. Due to these anatomical features, both exercises are considered specific to the intrinsic muscles of the foot. Both exercises induced significantly greater shear modulus in the intrinsic muscles (AbdH and FHB) compared to the resting phase The primary differences between the two exercises lie in the method of resistance application to the toes and the affected toes. During short-foot exercise all toes receive force from the floor simultaneously. However, the primary objective of this exercise is to raise the medial longitudinal arch of the foot, rather than increasing resistance to the toes [4, 5]. In contrast, in MTP flexion exercise, resistance force is passively applied to the toes, and this force can vary based on each participant’s toe function. Furthermore, resistance force is applied to the hallux and lesser toes separately. We believe that these methodological differences resulted in significant differences in shear modulus for FDB, QP, and FDL.
Previous studies have reported that some patients cannot perform short-foot exercise satisfactorily and that this is one of the most difficult exercise therapies to implement [4, 10]. The MTP flexion exercise is easy to understand and perform because it only flexes the MTP joint while maintaining the IP joint in a neutral position. This exercise has the advantage that the resistance can be changed manually. Progressive overload, which is one of the principles of muscle strength training, can be applied. Static and dynamic strength trainings are also possible. Furthermore, a box or floor can be used instead of the hand to apply resistance to the toes. Therefore, we believe that the MTP flexion exercise can be applied in clinical settings and training as a simple and useful exercise for the intrinsic muscles of the foot.
This study has several limitations. We evaluated muscle activity during exercise in a relatively small sample of an asymptomatic population. The effects are unknown in children, older individuals, and patients with foot disorders. Further studies are needed to clarify the effects of these exercises in improving physical performances such as muscle strength, jumping ability, and balance. However, the effects of short-foot exercises have been proven in previous studies; hence MTP flexion exercises may achieve similar or superior effects.
Conclusions
The shear modulus of the investigated muscles except the FHL muscle was significantly greater during MTP flexion exercise compared to the resting phase. The FDL muscle showed greater shear modulus during MTP flexion than during short-foot exercise. It is believed that the measured shear modulus represents muscle contraction intensity. Hence, our data suggested that MTP flexion exercise could induce equivalent or higher contraction activity in the investigated muscles than short-foot exercise. In the MTP flexion exercise, the passive resistance force can vary depending on the individual’s toe function, and this force can be applied separately to the hallux and lesser toes with the goal of inducing targeted muscle contraction in each toe Thus, the MTP flexion exercise can be expected to be an effective training method for strengthening the intrinsic muscles of the foot.
Author contributions
All listed authors made valuable contributions to the development of this manuscript. Conception: KH, KW; Data collection: KH, KN; Interpretation and analysis of data: KW, KH, HM, MW; Preparation of the manuscript: KH, KW; Revision for important intellectual content: KW, AT; Supervision: AT.
Ethical approval
The study was approved by the Institutional Review Board of Sapporo Medical University (Approval number: 1-2-70).
Funding
The study was funded by Japan Sports Medicine Foundation 2018 and a Grant-in-Aid for Scientific Research (JSPS KAKENHI Grant Number JP20K11284).
Informed consent
An informed consent form was included at the beginning of the survey, which presented the necessary information and recorded the participant’s willingness to participate in the study. Written informed consent was obtained through participants’ signature on the consent form.
Footnotes
Acknowledgments
The authors would like to thank Editage (
Conflict of interest
None to report.