
Abstract
BACKGROUND:
Studies on the effects of performing short foot exercises (SFEs) on the medial longitudinal arch (MLA) have been inconclusive.
OBJECTIVE:
This study aimed to conduct a systematic review of the effects of SFEs.
METHODS:
‘SFE’ and ‘intrinsic foot muscle’ were keywords used to search for randomized controlled trials. One researcher screened relevant articles based on their titles and abstracts, and two independent researchers closely read the texts, accepting nine studies for inclusion. Outcomes, intervention duration, frequency, and the number of interventions were investigated.
RESULTS:
Of 299 potential studies identified, the titles and abstracts of 211 studies were reviewed, and 192 were excluded. The full texts of 21 studies were obtained and evaluated according to inclusion and exclusion criteria. Nine studies met the inclusion criteria. Six studies concerning the MLA were identified, with four reporting MLA improvement. There was no consensus concerning the number and frequency of SFEs performed, and the mechanism of MLA improvement was unclear. MLA improvement was observed in participants who undertook
CONCLUSIONS:
The results suggest that performing SFEs for
Introduction
Flat foot deformity
Flat foot deformity is a chronic foot condition that includes flattening of the medial longitudinal arch (MLA), hindfoot valgus, and midfoot abduction [1], with a reported prevalence of 2–23% in adults [2]. The following factors have been associated with flat feet: occupation [2], obesity [3], and age [4]. Recently, injuries to foot ligaments [5] and a decreased muscle cross-sectional area of the intrinsic foot muscles (IFMs) [6] have also been reported in flat feet, suggesting that foot function is impaired. Studies comparing flat feet with normal alignment have reported that flat feet involve a higher incidence of plantar tendinitis [7]. Furthermore, flat feet have been cited as an important etiology of several lower extremity overuse injuries, including low back pain [8] and shin splints [9, 10]. Therefore, treating a flat foot deformity may potentially prevent overuse injuries.
Treatment for flat foot deformity
Flat feet have previously been classified as flexible or rigid [11]. For rigid flat feet, surgical treatment to correct the bony structure is common [12]. For flexible flat feet, clinically asymptomatic cases do not require intervention [13]. For symptomatic cases, conservative therapy such as nonsteroidal anti-inflammatory drugs, weight loss, functional foot orthoses, physical therapy, and exercise therapy remain treatments of choice to relieve pain and prevent progression of the deformity [14, 15]. Exercise therapy for flat feet includes extrinsic muscle and IFM strengthening to maintain the MLA [16, 17]. The effects of toe flexion exercises, such as the toe curl exercise (TCE), have also been reported [18]. However, the TCE involves the use of both IFMs and extrinsic foot muscles, and recent studies have focused on the IFMs alone [19, 20, 21]. It has been reported that patients with flat feet have higher incidence rates of IFM atrophy compared with patients with a normal MLA [7] and there is a correlation between cross-sectional areas of atrophied IFMs, such as the abductor hallucis longus and flexor digitorum brevis muscles, and the severity of flat feet [22]. Short foot exercises (SFEs) have been used as exercise therapy for IFMs.
Short foot exercises
SFEs shorten the length of the foot through contracting the plantar muscles of the foot to pull the first metatarsal towards the heel and heighten the MLA without flexing the toes [23]. In flatfoot deformity, SFEs are used to strengthen the IFMs, which maintain the MLA [24, 25]. Okamura reported that this exercise decreased foot posture index (FPI) values [26]. In chronic ankle instability, an eight-week SFE intervention was shown to increase Cumberland Ankle Instability Tool (CAIT) values [27].
Prior studies have reported that some patients cannot perform SFEs satisfactorily, even after two weeks of practice [28], and that this is one of the most difficult exercise therapies to implement. In addition, studies on the effect of SFEs on MLA improvement in patients with flat feet have reported differing outcomes [29] and this area remains contentious. Furthermore, the number and frequency of SFEs performed, the duration of the intervention, and the types of outcomes evaluated have not been fully investigated.
Study purpose
The purpose of this study was to conduct a systematic review of studies that provided full details concerning the number and frequency of SFEs undertaken, the duration of the intervention, and the types of outcomes, along with the effects of SFEs.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement and was registered in the PROSPERO database under the identification number CRDCRD42020183467.
Search method
A combination of the following keywords and their variation were used: (short foot exercise OR (short or foot or exercise) OR SFE) AND (intrinsic muscle OR (intrinsic or muscle) OR IFM) to search for randomized controlled trials (RCTs) up to October 2021. We used PubMed, Physiotherapy Evidence Database (PEDro), and the Cochrane Library (including Cochrane Central Register of Controlled Trials, CENTRAL) as search databases. Two reviewers independently conducted the search.
Inclusion and exclusion criteria
The target studies were selected in terms of the abstracts of related articles identified during the database search. The retrieved studies were screened to determine their relevance. Inclusion criteria comprised: (i) RCTs, (ii) studies that included at least one group using an SFE as an intervention, and (iii) articles published in English. Exclusion criteria comprised: (i) animal experiments, and (ii) abstracts, letters, reviews, systematic reviews, meta-analyses, or case reports.
Flowchart for the selection of included trials.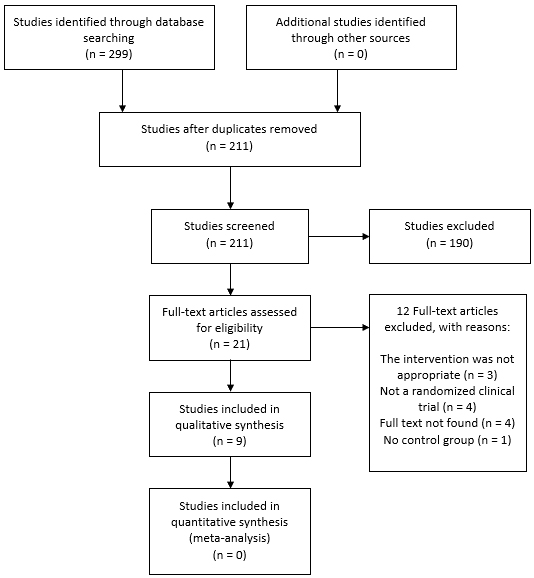
The selected studies were independently and critically reviewed and evaluated by two reviewers using the Cochrane risk of bias tool for randomised trials (RoB 2.0), to assess the methodological quality of the included studies for risk of bias across five domains: (i) the randomization process, (ii) deviations from intended interventions, (iii) missing outcome data, (iv) measurement of the outcomes, and (v) selection of the reported results. Studies with a low risk of bias in all five domains were considered to have a low risk of overall bias, studies with some concerns in at least one domain were considered to have some concerns overall, and studies with a high risk of bias overall or a high risk of bias in at least one domain were considered to have a high risk of bias. Studies with at least one domain of some concern were considered to have a concern overall, whereas those with at least one domain of a high risk of bias or studies with multiple domains of some concern were considered to have a high risk of bias. Disagreements among the reviewers were resolved through discussion [30].
Risk of bias graph: a review of authors’ evaluations concerning each risk of bias item presented as percentages across all included studies.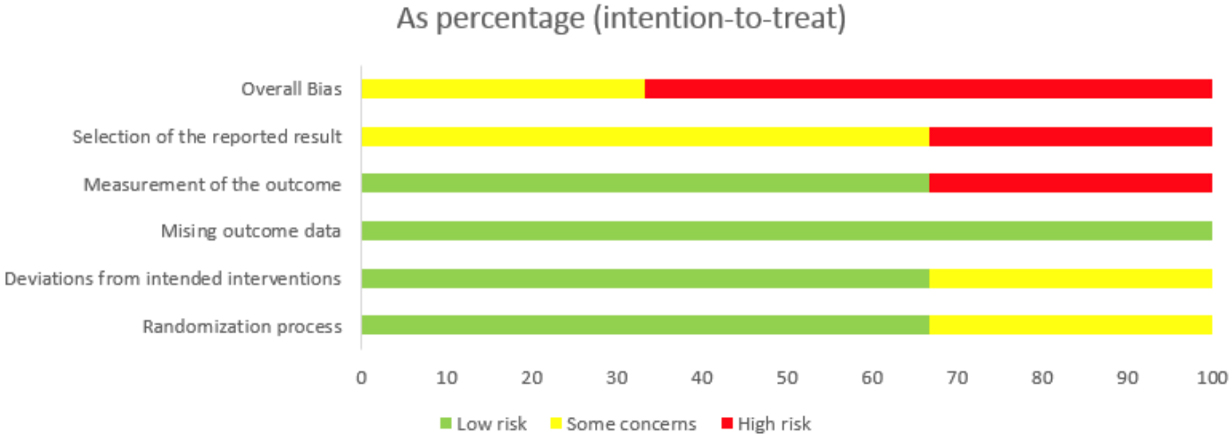
Risk of bias summary: a review of the authors’ evaluations concerning each risk of bias item for each included study.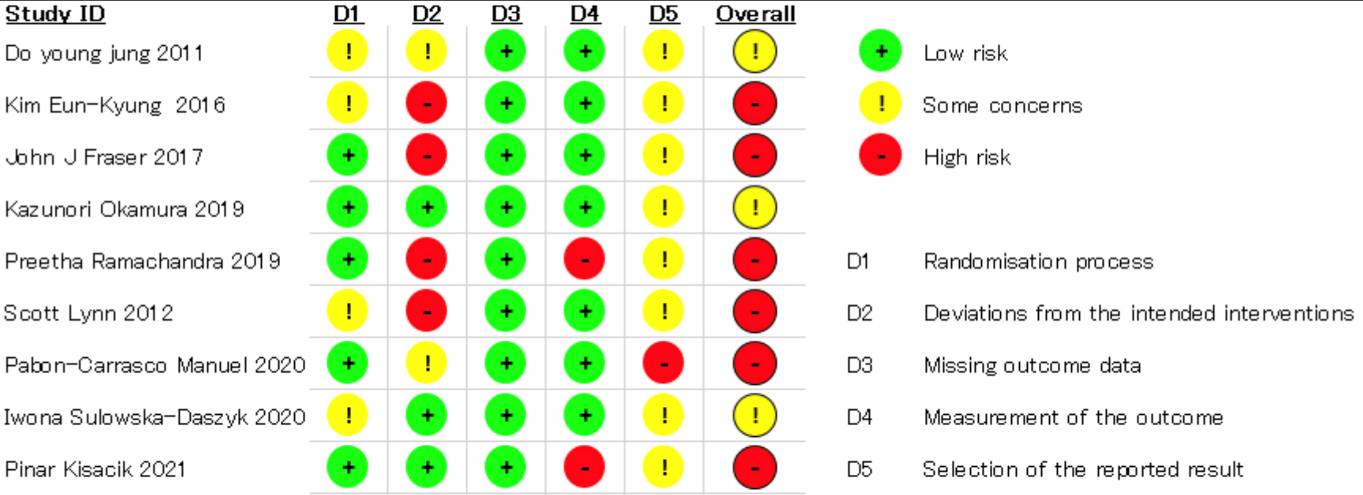
A meta-analysis was conducted on dynamic balance, specifically the Y-balance test. One reviewer extracted all the relevant data separately. The extracted and tabulated data included the lead author, year of publication, the number of participants, total score (number of SFEs, frequency of intervention, duration of intervention), type of muscle contraction, posture of execution, duration of muscle contraction, and type of outcome.
Total score
The amount of load was also compared.
Statistical analysis
This meta-analysis was performed using Review Manager Version 5.4 software. Statistical calculations were performed for all included studies using detailed data for SFE alone, SFE combined with other exercise therapies, and exercise therapies alone. An SFE group (SFE combined with exercise therapy) and an exercise therapy group (exercise therapy only) were compared using a random-effects model. Statistical reliability was calculated using 95% confidence intervals (CIs). Statistical heterogeneity was assessed using
Results
Study selection
A database search identified 291 potential studies, and 211 abstracts remained after duplicate studies had been removed. The abstracts were then reviewed, and a preliminary evaluation was conducted to assess the eligibility of 21 full-text articles. Nine studies met our inclusion criteria and 12 were excluded, as the interventions in those studies were deemed inappropriate (Fig. 1).
Study characteristics
SFE setting
The basic characteristics of the nine selected studies are shown in Tables 1 and 2. Concerning the number of times a single SFE intervention was conducted, the minimum was five times and the maximum was 104 times. Interventions were provided 2–7 days per week, and the intervention period ranged from 4–14 weeks. The total score ranged from 120 to 6552. One study did not provide details concerning the number of repetitions; therefore, the total score could not be calculated.
The MLA
Navicular height, the navicular drop test (ND), and the FPI were used to measure the MLA. Six reports concerning the MLA were identified, of which four reported an improvement in the MLA. Kim et al. conducted a five-week SFE study among university students with flat feet and reported a significant decrease in ND post-intervention [33]. Okamura et al. conducted SFEs with electromyographic biofeedback in university students with flat feet and reported a significant post-intervention improvement in the FPI at eight
Characteristics of the selected studies
Characteristics of the selected studies