
Abstract
BACKGROUND:
Although mulligan sustained natural apophyseal glides (SNAG) and maitland mobilization (MM) are common interventions for musculoskeletal disease, no study has directly compared the effectiveness of mid-thoracic spine mobilization in subacute stroke patients.
OBJECTIVE:
To investigate the effects of mid-thoracic spine mobilization (SNAG vs. MM) on postural balance and gait ability in subacute stroke patients.
METHODS:
Fifty subacute stroke patients were randomly allocated to the SNAG (
RESULTS:
Participants reported no adverse events, and there was no loss to follow-up. The SNAG and MM group patients demonstrated significant improvements (
CONCLUSIONS:
Mid-thoracic spine mobilization allows significant improvements in postural balance and gait ability in subacute stroke patients, with no differences between the SNAG and MM techniques.
Introduction
Cerebrovascular stroke causes local neurological dysfunction induced by impaired blood flow due to cerebrovascular abnormalities [1, 2]. In general, muscle paralysis, sensory loss, and cognitive and speech disorders are induced, hindering the performance of independent daily activities [3]. Asymmetrical posture and loss of balance due to hemiplegia can increase the risk of falls [4, 5]. Furthermore, abnormal muscle tension and degraded weight bearing and movement ability lead to changes in the muscles and connective tissue of the paralyzed lower extremity, resulting in abnormal gait patterns [6, 7]. Therefore, improving posture control and balance ability is considered an important factor affecting the rehabilitation of stroke patients.
The thoracic, lumbar-pelvic, and cervico-cranial postures of the human body are interconnected, and dysfunction of the central thoracic vertebrae (T4–8) in particular affects the center and line of gravity [8]. Previous studies have reported that an increase in thoracic kyphosis induces higher multi-segmental spinal loads in the vertical position and exacerbates the pain and degenerative changes in the spinal segments [9]. Relative trunk mobility restrictions and kyphotic posture due to hypomobility of the thoracic segment also adversely affect postural balance control, increasing the risk of secondary falls [10, 11]. In particular, stroke patients exhibit an asymmetrical weight-bearing pattern, which lowers the rearward movement of the center of pressure (COP) when the toe is lifted during the process of gait initiation, causing gait disturbance due to a decrease in propulsion [12].
In clinical practice, Mulligan sustained natural apophyseal glides (SNAG) or Maitland mobilization (MM) are commonly used to improve vertebral joint mobility. MM is a manual therapy technique performed by applying repetitive and rhythmic passive movements of small or large amplitudes within the range of motion of the vertebrae [13]. SNAG involves the movement of the spine combined with the facet joint glide under weight bearing, which is a technique combining the active movement of the patient with the passive additional movement provided by the therapist [14]. These manual therapy techniques ultimately aim to reduce pain and control normal posture through the improvement of joint mobility. Although previous studies have reported improvements in pain and mobility of the vertebral joint using both techniques [15, 16, 17, 18], no high-quality evidence has been found. Furthermore, the therapeutic basis for improving the kyphotic posture of stroke patients is still insufficient. There is a lot of room for discussion about this in clinical practice and studies, which necessitates a study to determine which joint mobilization method is effective. This study aimed to investigate the effects of mid-thoracic spine mobilization (SNAG vs MM) on postural balance and gait ability in subacute stroke patients. We further compared the effects of mid-thoracic spine mobilization using two techniques, SNAG and MM.
Methods
Participants
In this study, 50 subacute stroke patients were recruited from the Department of Rehabilitation Medicine at K-University Hospital from January to March 2019. The following inclusion criteria were applied: diagnosis of stroke by a radiologist; no vision or hearing problems; a modified Ashworth scale score of
Those who had received previous thoracic surgery or had other diseases that could cause poor balance were excluded (e.g., spinal cord pathology, cerebellar ataxia, or Parkinson’s disease).
The number of participants required to obtain significant outcomes was calculated using G*Power 3.1 software [19]. The effect size for this study was set according to an effect size of f(V) 0.485 on the 10-m walk test (10MWT), based on a previous study [20] that compared the effect of dual-task training on balance and gait ability in subacute stroke patients. Allowing for a conservative dropout rate of 10%, the investigators planned to recruit at least 50 participants.
Flowchart of patient recruitment, randomization and follow-up.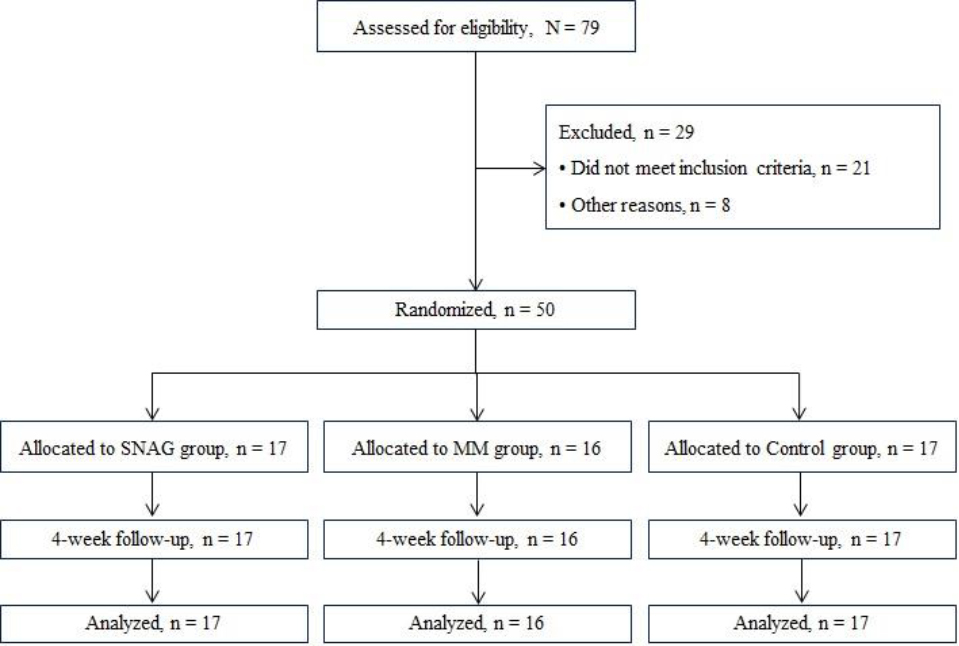
This study was conducted by three physical therapists, one of whom recruited patients who met the eligibility criteria and collected all data on the basic characteristics of the participants. After the baseline examination, 50 patients were asked to select one of three cards in the box, to be randomly assigned to either the SNAG group (
Interventions
This study lasted a total of 4 weeks, the evaluations were performed prior to treatment initiation and post-treatment evaluations were conducted after applying the intervention 20 times. All groups underwent a neuro-developmental therapy (NDT) program for four successive weeks (five sessions per week). The NDT program consisted of upper extremity exercise, lower extremity exercise, and gait training. The SNAG and MM group additionally received (10 min) mid-thoracic spine mobilization, whereas the control group received only the NDT program. Joint mobilization was performed by two physical therapists with more than five years of clinical experience and more than 150 hours of specialized manual therapy training.
The first experimental group, the SNAG group, received SNAG treatment on the mid thoracic spine (T4–8) in a sitting position (Fig. 2). SNAG is a technique that applies the motion of the spine and the facet joint glide to the end range of the joint under weight bearing. Here, the continuous glide should be maintained until returning to the initial starting position, which always needs to be directed forward regardless of the direction in which the movement is restricted. In this study, while the therapist applied the sustained accessory glide by pushing up the articular surface of the facet joint using the hypothenar or both thumbs of the therapist, the patient was instructed to slowly and actively perform trunk extension joint motion.
SNAG and MM used in this study.
BioRescue.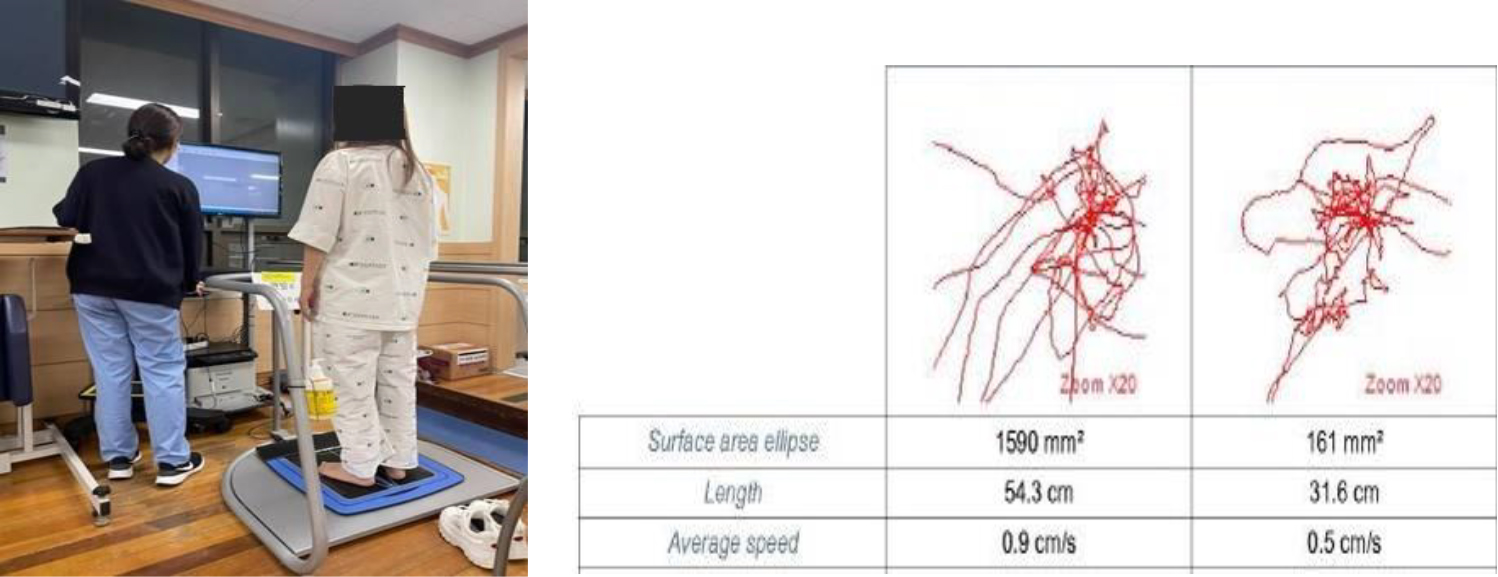
In the second experimental group, the MM group, repeated oscillation mobilization was performed on the central thoracic vertebrae (T4–8) using both thumbs in a prone position (Fig. 2). The therapist performed one 30-second bout of grade III or IV central posterior-anterior mobilization at the spinous process, as described by Maitland [13]. During joint mobilization, the patient’s discomfort was assessed and the procedure was conducted three times per segment. The joint mobilization lasted a total of
The primary outcome measure used in this study was the postural sway, as measured by BioRescue (RM INGENIERIEK, Rodez, France). BioRescue is a 61,058,010-mm platform comprising a total of 1,600 pressure sensors, where the data samples are collected at 100 Hz via the sensors. The postural sway is the degree of movement of the COP on the basal plane, and the surface area of the ellipse, length, and speed of the movement of the COP are identified. The participant was asked to observe the marked point in front of them while standing on the platform, and then to maintain the standing posture for 60 seconds before measuring the displacement of the COP (Fig. 3) [21].
Secondary outcome measures included the Five times sit-to-stand test (FTSST), Functional reach test (FRT), 10MWT, 6-minute walk test (6MWT) and global rating of change (GRC).
FTSST is a tool to measure dynamic balance ability through the time of sitting and standing on a 43 cm high chair and performing five repetitions of sitting and standing at the fastest possible speed. The test-retest reliability of this tool is ICC
FRT measures a patient’s dynamic balance ability when performing arm extension in a standing position, which is known as a test method with high inter-rater reliability of ICC
The 10MWT measures the walking time on a straight 12-m walking path, and the 10-m walking speed in the middle section, excluding the initial and final 1 m, is measured. Auxiliary tools and braces are used when necessary, and high reliability has previously been achieved in stroke patients with ICC
The 6MWT measures the total walking distance in 6 minutes as a measure to evaluate walking endurance [25]. The intraclass correlation coefficient for distance was 0.94.
The GRC was used to assess self-perceived improvement at post intervention [18]. GRC was used to objectively test the improvement of the patient symptoms to identify the intervention effect and the satisfaction after finishing the treatment in clinical practice. This scale has demonstrated acceptable levels of reliability and validity. The MCID for the GRC has been reported as a 3-point change from baseline [26].
Baseline demographics of the two groups
Baseline demographics of the two groups
The baseline characteristics of patients were compared between treatment groups, using independent
Comparison of the outcome measures within and between groups
Comparison of the outcome measures within and between groups
The baseline characteristics between the groups were similar for all variables (
The postural sway used as a primary outcome measure in this study showed a statistically significant improvement in the mobilization groups compared to that in the control group (
Discussion
The results of this study demonstrated that both SNAG and MM are safe and effective therapeutic techniques for improving balance and gait in subacute stroke patients. The novelty of the present study is that mid-thoracic spine mobilization using two treatment techniques can help improve the center and line of gravity of stroke patients and help improve balance and gait ability secondarily. However, there was no statistically significant difference between the two techniques, which is consistent with the results of previous studies on cervicogenic dizziness patients [27].
During the subacute period after the onset of stroke, the aerobic activity of the body decreases, leading to trunk instability and cardiopulmonary function decline due to unilateral paralysis [28]. In particular, dysfunction of the thoracic spine in the kyphotic posture directly or indirectly affects the movement of the trunk [8]. Therefore, in this study, the passive intervention method, MM, and the active assistance intervention method, SNAG, were applied to the central thoracic spine for subacute stroke patients, a period in which significant neuroplastic changes occur. As a result of this study, the postural sway used as a primary outcome measure showed a statistically significant decrease, with improved postural stability after four weeks in both groups. The postural sway is the degree of movement of the COP on the basal plane, the surface area measures the spatial variability of the COP, and the length indicates the path of the COP. In other words, the lower the resultant value of the measurement item, the less the postural sway, thus denoting a state of high postural stability. Therefore, it was confirmed that mid-thoracic spine mobilization effectively improved postural control by restoring the abnormal center and line of gravity of stroke patients. In a similar previous study, thoracic spine mobilization significantly reduced the amount of change in postural sway and fall index in patients with lumbar instability, reporting an improvement in static balance ability [29]
Hemiplegia in stroke patients results in decreased postural stability, and postural sway due to this instability is associated with movements that require weight shift [30]. In particular, the analysis of COP can help evaluate the onset of gait in stroke patients [31], and the risk of unilateral falls is said to increase with a decrease in dynamic postural control [32]. In this study, secondary outcome measures to investigate changes in dynamic balance and gait ability showed statistically significant effects after four weeks in both groups. This was consistent with the results of previous studies that confirmed the correlation with improvements in balance and walking ability through COP [33, 34, 35]. Although the mechanism of joint mobilization used in this study has not yet been clearly elucidated, the sensitivity of mechanoreceptors [36] and the biomechanical relationship of the spine can be improved through continuous passive stimulation of soft tissue, reducing stress on spinal motion segments [37, 38]. Therefore, the results of this study suggest that the shortened abdominal wall was straightened due to the improvement of thoracic hypomobility, improving the trunk movement in stroke patients. In other words, the dynamic balance and gait ability seemed improve as the abnormal center and line of gravity induced by the kyphotic posture were restored. Although there was no difference in effect between the two experimental groups in this study, MM allowed accurate maneuvering according to posture fixation, whereas SNAG has conflicting advantages according to the active movement of the patient, influencing the outcome of the intervention. We also speculate that the specificity of subacute stroke patients might have influenced the outcome of the intervention. In other words, other physical disorders, such as muscle weakness due to hemiplegia and degenerative changes in joints due to aging, may have acted as variables. In this study, after four weeks of intervention, 76.5% and 75% of participants in the SNAG and MM groups, respectively, scored
Conclusion
This study demonstrates that subacute stroke patients who receive the mid-thoracic spine mobilization demonstrate significant improvements on postural balance and gait ability. Although there was no difference in the improved effectiveness between the two mobilization techniques, this study provides the first documented clinical evidence of the positive benefits of mid thoracic spine mobilization for improvement of postural balance and gait ability in subacute stroke patients. Future studies should investigate the effectiveness of different types and dosages of manual therapy and include long-term follow-up data collection.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
The authors report no funding.