
Abstract
BACKGROUND:
Normal alignment of the foot is important because the feet support the body’s weight. The intrinsic muscles of the foot mainly maintain the alignment and movement of the foot, whereas the abductor hallucis (AbdH) aligns the first metatarsophalangeal joint and maintains the medial longitudinal arch.
OBJECTIVE:
This study was conducted to investigate the muscle activity of the AbdH and hallux valgus (HV) angle during three different foot exercises.
METHODS:
Participants included 15 subjects aged 20–24 years with mild HV. All subjects performed three different foot exercises in random order: short foot exercise (SF), toe spread out exercise (TSO), and TSO with a pressure bio-feedback unit (TSOP). The muscle activity of the AbdH and the HV angle were measured during each foot exercise using surface electromyography and X-ray and then compared using one-way repeated-measures analysis of variance, followed by Bonferroni adjustment.
RESULTS:
AbdH muscle activity differed significantly among SF, TSO, and TSOP. AbdH muscle activity was greater in TSOP (89.60%) than in SF (19.99%) and TSO (60.96%) (
CONCLUSIONS:
TSOP can be recommended as an effective AbdH strengthening exercise in subjects with mild HV.
Introduction
Hallux valgus (HV) is a common foot malalignment among adults that is characterized by progressive deformity with lateral deviation of the great toe in the first metatarsophalangeal joint (1MTPj) [1]. This condition causes pain on the medial aspect of the first metatarsal head [2]. The incidence of HV increases with age, reaching approximately 23% in individuals aged 18 to 65 years and 35% in those over 65 years of age [3]. The HV angle is defined as the angle between the medial line of the first proximal phalanx and the first metatarsal bone [4], and the severity of HV is classified into four stages based on this angle:
The AbdH muscle originates from the medial calcaneal tuberosity and attaches to the medial sesamoid and medial aspect of the first proximal phalanx. It contributes to maintaining the alignment of the 1MTPj and performs not only abduction as a main function but also flexion at 1MTPj [13], because it is located below the transverse axis of the 1MTPj [14]. The intrinsic muscles including AbdH, flexor hallucis brevis, and interosseous muscle stabilize the arch of the foot. In particular, the AbdH plays a key role in maintaining the medial longitudinal arch (MLA) and normal alignment of the 1MTPj and is used as a dynamic stabilizer of the MLA during the toe-off phases and late stance of the gait [15]. HV leads to deformity of the muscle structure because the position of the AbdH is shifted to the plantar aspect, causing an abnormal anatomical relationship with the 1MTPj [10] that can result in decreased AbdH activity and abnormal alignment of the MLA [13]. Insufficient strength of the intrinsic muscles may cause the impairment of arthrokinetic foot movements and MLA alignment [13]. Therefore, sufficient strength of the intrinsic foot muscles and AbdH activity are important factors for normal alignment of the MLA and improving HV angle [10]. AbdH muscle activity is significantly lower in subjects with HV than in healthy subjects during foot exercise [16].
Exercises such as picking up objects, toe towel curl, unilateral balance activity, shin curl, and short foot exercise (SF) have been used to strengthen the foot intrinsic muscles [17, 18]. SF is an exercise that elevates the MLA by pulling the head of the metatarsal toward the calcaneus without toe flexion in the sitting or standing position [19]. A previous study reported that SF significantly increased AbdH muscle activity to a greater extent than toe curl exercise [20]; this effect occurs because the anatomical location of the AbdH causes flexion of the great toe at the 1MTPj [14]. Therefore, SF and intrinsic muscle strengthening exercises have been recommended in the fields of rehabilitation and sports medicine to treat rheumatoid arthritis [21], hammer toe deformities, and claw toe including HV [22, 23].
Recently, toe spread out exercise (TSO) was introduced as a novel approach for preventing HV [24]. A previous study reported that TSO significantly increased AbdH muscle activity compared to SF among subjects with mild HV [23]. Another study confirmed the HV angle and cross-sectional area of the AbdH muscle by applying orthosis and TSO in HV subjects [26]; the cross-sectional area of the AbdH was found to increase significantly, and the HV angle was significantly smaller in the TSO group with orthosis [26]. The results of these studies suggest that TSO may be an effective method for preventing HV.
In subjects with mild HV, the activity ratio between the AbdH and AddH muscles was found to be closer to 1:1 during TSO than during SF [23]. Therefore, TSO was suggested to be a more effective exercise than SF for AbdH activity and changes in HV angle in subjects with non-ideal HV [23, 24]. However, to date, studies of TSO for increasing AbdH muscle activity have been performed without consideration of the MLA. Therefore, this study was conducted to investigate which kind of exercise effectively activates the AbdH muscle while also considering the MLA, by modifying TSO using a pressure bio-feedback unit (PBU). In this study, we compared the AbdH muscle activity and the HV angle during three different foot exercises: short foot exercise (SF), TSO, and TSO with a PBU (TSOP). We hypothesized that AbdH muscle activity and the HV angle would be significantly different among SF, TSO, and TSOP exercise. Our results may be used to recommend exercise methods to selectively strengthen the AbdH muscle in subjects with HV.
Methods
Three different foot exercises. (A, B) Short foot exercise. (C, D) Toe spread out exercise. (E, F) Toe spread out exercise with pressure biofeedback unit. Each exercise is shown in antero-posterior and medio-lateral view, respectively.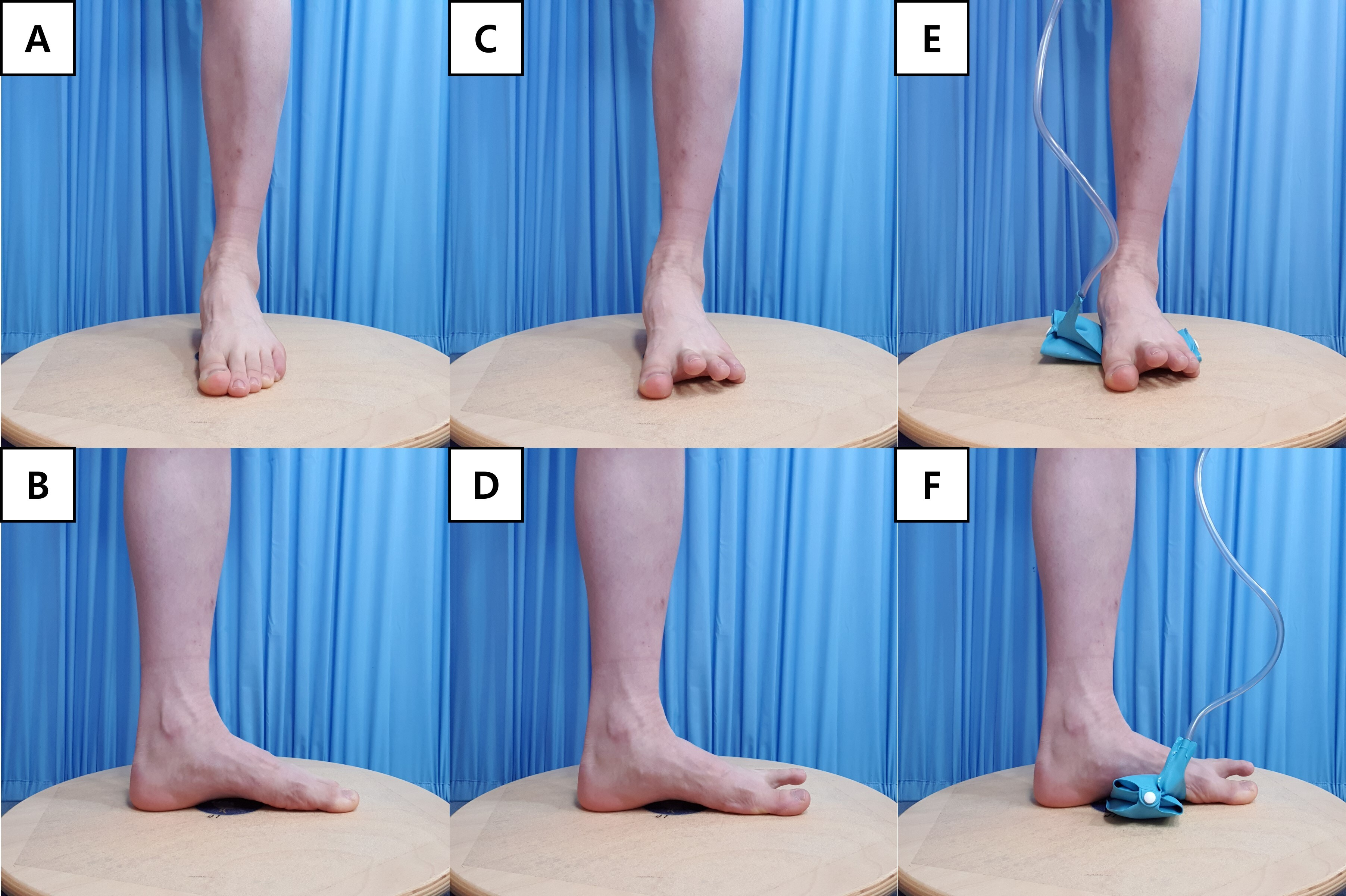
The G-v3.1.2 power analysis software (Franz Faul, University of Kiel, Kiel, Germany) was used in a preliminary study that included five subjects. The software was set at a power of 0.80,
Data collection
AbdH muscle activity
AbdH muscle activity was measured using a wireless electromyography (EMG) feedback system (EMG System 1000, BTS, Italy). The bandpass digital filter was set between 20 and 450 Hz. The sampling rate was 1024 Hz. Root mean square (RMS) data were calculated; the moving window was 50 ms. We used a PBU (Chattanooga Stabilizer, Chattanooga Group Inc., USA) for MLA control through biofeedback during TSOP. The EMG signal was recorded for 5 s while the subject maintained the end position of the foot exercise, and the initial and final seconds of the signal were discarded [27]. To minimize resistance, the skin to which the electrode was attached was cleaned with alcohol-soaked cotton. The EMG electrode was attached the belly of the AbdH muscle at 1–2 cm posterior to the tuberosity of the navicular [10]. Muscle activity was normalized by measuring the maximum voluntary isometric contraction (MVIC) of the AbdH muscle. The investigator fixed the heel in the supine position and applied resistance in the opposite direction to abduction of the 1MTPj [28]. The MVIC of the AbdH muscle was recorded as an average of three trials. EMG data for the AbdH muscle were collected during SF, TSO, and TSOP and expressed as %MVIC.
HV angle measurement
The HV angle was measured using radiographic imaging (KOB, Donga X-ray, Anyang, Korea). A radiologist with 5 years of clinical experience used the Centricity PACS RA1000 v2.1.0 software package (GE Healthcare Integrated IT Solutions, Barrington, USA) to measure the HV angle, defined as the angle formed by the intersection of the medial line of the proximal phalanx and the metatarsal bone. Each subject sat on a chair on an ultrasound table with a neutral ankle joint (0
Procedures
Flow chart of the experimental procedure. HV, hallux valgus; SF, short foot exercise; TSO, toe spread out exercise; TSOP, toe spread out exercise with pressure biofeedback unit; %MVIC, percentage maximal voluntary isometric contraction.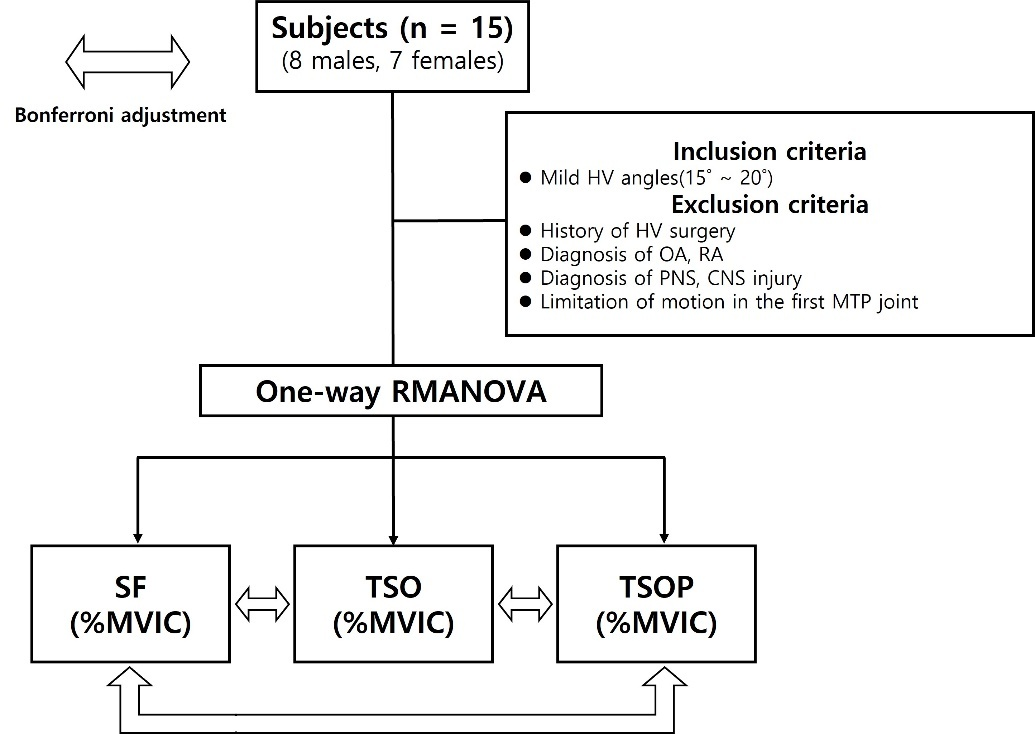
Prior to performing the exercise, each subject practiced the exercise three times in a sitting position. The exercises were performed in random order, and subjects were blinded to the effects of the exercises. AbdH muscle activity was measured for 5 s while the maximum contraction was maintained. The subject was asked to return to the resting position after 5 s. In all exercises, muscle activity was calculated as an average of three trials. Subjects rested for two minutes between exercises to minimize muscle fatigue [30].
Subjects evenly distributed their body weight on the soles in a sitting position. Each subject was asked to pull the head of the metatarsal toward the heel without toe flexion and to arch the foot (Fig. 1A and B). The metatarsal head and heel were supervised to avoid detaching from the floor while performing the exercise [19].
TSO
Subjects evenly distributed their body weight on the soles in sitting position. Each subject was asked to lift all of the toes with the attached head of the metatarsal and heel. Next, the subject put the little toe down in the lateral direction and put the great toe down in the medial direction (Fig. 1C and D). The metatarsal head and heel were supervised to avoid detaching from the floor while performing the exercise [24].
TSOP
The PBU was placed below the MLA of the subject in a sitting position and the target pressure of the PBU was set at 30 mmHg. While performing TSO, the subject pulled the first metatarsal toward the heel to reduce the target pressure of the PBU at 20 mmHg (Fig. 1E and F). The metatarsal head and heel were supervised to avoid detaching from the floor while performing the exercise.
Statistical analyses
All statistical data were analyzed using the SPSS v18.0 software (SPSS IL, Chicago, IL, USA). The measured data were tested for normality using the Kolmogorov–Smirnov test. To assess the effects of exercise, the effect size was calculated using Cohen’s d value. Values greater than 0.8 were considered as strong, values greater than 0.4 to less than or equal to 0.8 were rated as moderate, and values less than or equal to 0.4 were regarded as weak [31]. One way repeated-measures analysis of variance (ANOVA) was used to compare the values of dependent variables (Fig. 2). The effect of each exercise was compared using Bonferroni adjustment. Statistical significance was evaluated at a level of
Results
Electromyography activity of the abductor hallucis (AbdH) muscle during three different foot exercises. %MVIC, percentage maximal voluntary isometric contraction; SF, short foot exercise; TSO, toe spread out exercise; TSOP, toe spread out exercise with pressure biofeedback unit. 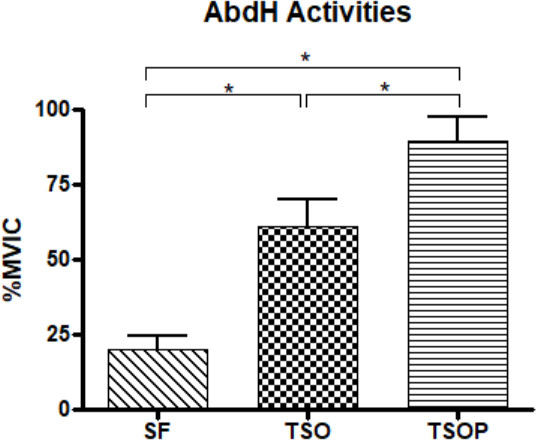
Comparison of abductor hallucis activity among three different foot exercises (
SD, standard deviation; SF, short foot exercise; TSO, toe spread out exercise; TSOP, toe spread out exercise with pressure biofeedback unit.
Comparison of hallux valgus angles among three different foot exercises (
HV, hallux valgus; SD, standard deviation; SF, short foot exercise; TSO, toe spread out exercise; TSOP, toe spread out exercise with pressure biofeedback unit.
In this study, 8 males (53%) and 7 females (47%) participated. A significant difference was observed among the three different foot exercises in activating the AbdH (
We compared the effects of three foot exercises (SF, TSO and TSOP) in terms of increasing AbdH muscle activity and decreasing the HV angle. AbdH muscle activity was significantly higher during TSOP than during SF exercise (69.62%) and TSO (28.64%). The HV angle was significantly smaller during TSOP (15.72
A previous study compared AbdH muscle activity between SF and TSO in subjects with normal HV angle and found that both exercises were effective for increasing AbdH activity in healthy subjects, although there was no significant different between SF (65.05%) and TSO (80.84%) [32]. Another previous study reported significantly higher AbdH muscle activity during TSO exercise (89.38%) than during SF exercise (44.42%) in subjects with mild HV [23]. Thus, we infer that TSO is a more effective exercise for subjects with a non-ideal HV angle. Based on these results, we investigated effective exercises in consideration of the MLA in subjects with mild HV.
For this research, TSOP was performed with great toe abduction at 1MTPj and elevated MLA, accompanied by pressure biofeedback. Because TSOP was performed by decreasing the pressure of the PBU placed below the MLA from 30 to 20 mmHg while performing TSO, the MLA was elevated, and the great toe was abducted. A previous study reported that AbdH muscle activity was significantly increased during exercise consisting of elevated MLA in a sitting position and a one-legged standing position [20]; the findings of that study were consistent with our results. The increased AbdH muscle activity observed in the present study may be explained by the position of the AbdH muscle, which is anatomically located below the transverse axis of the foot, whereas the AbdH tendon is linked with the flexor hallucis brevis muscle to perform abduction and flexion at the1MTPj [33]. Thus, elevation of the MLA during TSOP due to pressure biofeedback may have contributed to increased AbdH muscle activity. In the previous study, the postural change of the MLA was measured only in the end position of each exercise using video motion analysis software. Therefore, postural changes of the MLA during each exercise were not fully considered in real time, and it was not possible to capture movement while the exercise was being performed. In contrast, TSOP is an effective approach for performing continuous elevation of the MLA, because pressure changes can be monitored in real time throughout the exercise using the PBU. In another previous study, the thickness of the AbdH muscle was increased during exercise by elevating the MLA, contributing to the activation of the intrinsic muscles [34]. The MLA was similarly elevated by pressure biofeedback in the present study. This factor may contribute to increasing co-contraction with intrinsic and AbdH muscle activity during TSOP.
Osteokinematic movement during TSOP occurs in the sagittal and transverse planes; therefore, AbdH muscle activation was greater during TSOP than during SF and TSO. Movement in the sagittal plane occurs relative to the medio-lateral axis during SF, because this exercise is performed by pulling the metatarsal head toward the heel without toe flexion [13]. TSO was performed by putting the little and great toes down in the lateral and medial directions while the head of the metatarsal was fixed on the floor. In this exercise, movement in the transverse plane occurs relative to the vertical axis [13]. However, TSOP was performed with multi-angled toe movements in both the sagittal and transverse planes, because it involves abducting the great toe and pulling the metatarsal head toward the heel using pressure biofeedback. This osteokinematic factor may contribute to AbdH muscle activation originating from the medial calcaneal tuberosity and attachment to the medial proximal phalanx of the great toe in the shortened position. Due to these factors, AbdH muscle activity was increased to a greater extent during TSOP than during SF and TSO.
The mean HV angles during SF, TSO, and TSOP were 18.85
Our study had several limitations. First, our findings cannot be generalized to different ages because all of the subjects were in their 20 s. Further study is needed to investigate age effects. Second, it is impossible to confirm the results of our study for other HV severity levels because only subjects with mild HV were included. Further research is needed to confirm the effect of exercise on subjects with moderate or severe HV. Third, contraction of the flexor hallucis brevis and adductor hallucis was not investigated. Further study is required to compare the muscle activity ratio between the AbdH and the adductor hallucis. Finally, because our study was a cross-sectional study of AbdH muscle activity and the HV angle during three different foot exercises, more long-term research will be needed to investigate the lasting effects of these foot exercises.
Conclusion
Controlling the height of the MLA using a PBU may contribute to AbdH muscle activity. Therefore, TSOP is recommended for effective AbdH muscle activation in subjects with mild HV.
Ethical approval
The study protocol was approved by the Hoseo University Institutional Review Board (1041231-180320-HR-071-04).
Funding
This research was supported by the Academic Research fund of Hoseo University in 2021 (No. 20210464).
Informed consent
Informed consent was obtained from all participants prior to enrollment.
Author contributions
Conception and design, or acquisition, or analysis and interpretation of data: JIC. Drafting the article or revising it critically for important intellectual content: HBH, JIC. Final approval of the version to be published: HBH, JIC.
Footnotes
Acknowledgments
The authors express their gratitude to all participants for their valuable time and dedicated participation in the present study.
Conflict of interest
The authors declare that they have no conflict of interest.