
Abstract
BACKGROUND:
Even though literature indicates presence of weak hip abductors and lateral rotators’ in Patellofemoral Pain (PFP), studies evaluating the effect of hip abductors and lateral rotators strengthening to improve knee function and quality of life in PFP are limited.
OBJECTIVE:
This study systematically reviews and meta-analyzes the best evidence on the therapeutic value of strengthening hip abductors and lateral rotators muscles for treating PFP with a presumptive hypothesis that strengthening hip muscles stabilizes the patellofemoral joint, relieves pain, and enhances knee functions.
METHOD:
Medline, EMBASE, CINAHL, PEDro and PubMed Central databases were searched between January 1994 and September 2019 using the PICOS tool. The methodological quality of the selected studies were appraised individually using the 20-item McMaster Critical Review Form for Quantitative Studies. Supplemental quality appraisal of randomized controlled clinical trials performed using the Cochrane Collaboration’s ‘Risk of bias’ quality criteria. Data on patient population demographics, interventions, duration of intervention, and outcome measures were extracted and summarized in evidence tables and descriptive analysis. Meta-analyses under both fixed and random-effects models determined pooled effects size from appropriate RCTs.
RESULTS:
All fourteen studies demonstrated that hip muscle strengthening improved pain and knee function. All RCTs, except one, demonstrated that hip muscle strengthening is superior to quadriceps strengthening. Of the five RCTs assessing the additional effect of hip-quad versus quadriceps strengthening, four suggested that hip-quad strengthening is superior to standard quadriceps strengthening alone to improve PFP and knee function.
CONCLUSION:
In adult patients with PFP, strengthening hip abductors and lateral rotators’ have beneficial therapeutic effects than the conventional quadriceps exercises in improving knee pain and function both in the short- and long term. However, the present review data can be used to develop a standardized hip-quad protocol in the future.
Keywords
Introduction
Patellofemoral pain (PFP) is characterized by anterior knee pain emanating from the patellofemoral joint involving patella and fibrous tissue on the mediolateral retinaculum [1]. The aetiology is irregular patellar kinematics due to excessive pressure on the patellofemoral joint, poor proximal neuromuscular control, and hip muscle weakness [2, 3, 4]. The pain in PFP is because of inflammation coupled with damage to the bony, cartilaginous or connective tissues of the patellofemoral joint [1, 2, 5].
The PFP incidence rate is 25–40% of all cases of anterior knee pain, which is considerably high. Hence, therapeutic interventions are imperative to reduce permanent knee disabilities and improve quality of life [5, 6, 7]. The prevalence of PFP is higher in women and athletes than males (2:1) and is even higher (4:1) among athletes [6].
The works of literature on musculoskeletal injuries indicate a positive correlation between hip muscles weakness and PFP [8, 9, 10]. In a case report on PFP, authors noted that excessive hip adduction coupled with the weakness of the hip extensors and abductors are predominantly musculoskeletal concerns [10]. The current physiotherapy evidence strongly supports quadriceps muscle strengthening as an effective strategy to improve overall knee function in patients with PFP [11, 12, 13]. The proximal hip muscle exercises effectively relieved patellofemoral pain and improved knee function compared to knee exercises alone [14]. Therefore, strengthening these muscles underlie the objective treatment of PFP. While quadriceps strengthening is already the standard physiotherapeutic target for PFP, it is plausible that strengthening hip muscles will serve greater benefits because of its effect on greater control over the knee biomechanics [5, 15].
Relationship between hip muscles (abductors and lateral rotators) strength and PFP
Hip muscles (abductors and lateral rotators) are essential for knee and pelvic stabilization during ambulation [5]. The hip abductors and lateral rotators act synergistically to eccentrically control the hip adduction and internal rotation movements [15, 16, 17]. The diminished strength of hip abductors and lateral rotator muscles may result in poor neuromuscular control during activities that require loading on the patellofemoral joint [5, 8, 15]. The weak hip abductors may cause excessive femoral adduction, thereby augmenting lateral forces (Knee Valgum) acting on the patella [16]. In contrast, weak hip lateral rotators result in unrestricted internal rotation of the femur that augments contact pressure between the lateral facet of the patella and lateral femoral condyle [16]. Hence, weak hip muscles (mainly abductors and lateral rotators) are an important aetiological factor for PFP [5, 17, 18, 19].
Many studies compared the effectiveness of hip muscles strength in patients with PFP to matched healthy controls [19, 20, 21, 22]. Ireland et al. reported eccentric muscle strength reduction of 26% in hip abductors and 36% in hip lateral rotators among females with PFP, while Souza and Powers found a reduction of 14% in hip abductors and 17% in hip lateral rotators eccentric muscle strength compared to healthy matched controls [19, 21]. Nevertheless, Piva et al. found no significant muscle strength differences for hip abductors and lateral rotators in patients with PFP compared to healthy age/gender-matched controls; however, Baldon et al. reported significantly reduced strength for eccentric hip abductors, but not for hip lateral rotators among females with PFP to healthy matched controls [20, 22].
The weak hip lateral rotators cause unrestricted internal rotation of the femur about the tibia, enhancing misalignment at the knee joint that in turn leads to a biomechanical imbalance between the hip extensors and lateral rotators that overload the retinaculum and subchondral bone and subsequently potentiate patellofemoral pain and knee dysfunction [19]. Nevertheless, Earl et al. argued that strong hip muscles (abductors and lateral rotators) reverse these effects over the knee joint [3]. Moreover, rotational malalignment and patellar instability are well documented, and weak hip lateral rotator muscles are identified as important contributors [23, 24, 25]. It is important to consider the biomechanical assistance provided by the hip lateral rotator group muscles to maintain the normal alignment of the patella [26].
Ireland et al. and Souza and Powers noted more weakness in hip lateral rotators than hip abductors in patients with PFP [21, 19]. Ferber et al. found that in patients with PFP, the three weeks of isolated hip abductors strengthening reduced patellofemoral pain and increased gait-related knee-joint stability [9]. Two recent randomized controlled trials found that isolated strengthening of hip abductors and lateral rotators effectively relieves pain and improvise knee function in females [4, 27]. The available evidence for PFP considered exercises to strengthen the hip muscles that reduce pain and enhance long-term knee function [3, 4, 6, 27, 28].
Outcome measures of pain, knee function and health status in PFP
The available studies used self-reported Kujala Anterior Knee Pain Scale (AKPS), Visual Analogue Pain (VAS) scale, 11-point Numerical Pain Rating Scale (NPRS) and Pain Severity Scale (PSS) as an outcome measure to document patellofemoral pain in patients with PFP receiving therapeutic interventions [14, 29, 30].
The knee functions for patellofemoral pain were assessed using the Lower Extremity Functional Scale (LEFS), Tegner Activity Scale (TAS), Lysholm Knee Scoring Scale (LKSC)/Tegner Lysholm Knee Scoring Scale (TLKSS), Knee Outcome Survey-Activities of Daily Living Scale (KOS-ADL) and Functional Index Questionnaire (FIQ) [30, 31, 32, 33, 34].
Although the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) is tailored to examine the functional status of osteoarthritis, it is also used to measure health status for patients with patellofemoral pain (because patients with osteoarthritis often present with anterior knee pain, which is similar to patellofemoral pain) [29].
Since systematic reviews evaluating the effect of hip abductors and lateral rotator strengthening for patellofemoral pain, knee function and quality of life in patients with PFP are extremely limited, primarily this study systematically reviews and meta-analyzes the best evidence on the therapeutic value of strengthening hip abductors and lateral rotators muscles for the treatment of PFP. The presumptive hypothesis is that strengthening hip muscles stabilizes the patellofemoral joint, relieves pain and enhances knee functions.
Methods
Justification of the systematic review approach
Systematic reviews and meta-analyses are important methodologies for the qualitative and quantitative synthesis of published evidence. Shreds of evidence presented in systematic reviews are key for continuous quality and safety improvements in evidence-based clinical practice and, therefore, useful for clinicians and healthcare policymakers. The present review study used Centre for Reviews and Dissemination (CRD) guidance for undertaking reviews in health interventions to assess the value of hip muscle strengthening as therapeutic interventions in patellofemoral pain and knee function in patients with PFP [35]. Additionally, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement, recommended in CRD’s guidance, is used in literature searches to minimize article selection and reporting bias [36]. This study is exempt from Institutional Review Board approval as it is a literature review. The review has been registered with the Open Science Framework with reference doi:
Electronic bibliographic database searches
The controlled clinical trials (randomized and non-randomized), controlled comparative studies and cohort studies ((prospective and retrospective) published in the last 25 years (January 1994 to September 2019) in English language journals were performed across five electronic databases [Medical Literature Analysis and Retrieval System Online (Medline); Excerpta Medica Database (EMBASE); Clinical Index of Nursing and Allied Health Literature (CINAHL); Physiotherapy Evidence Database (PEDro) and The Cochrane Central Register of Controlled Trials (CENTRAL)]. Appropriate combinations of Medical Subject Headings (MeSH) or CINAHL headings with keywords (Table 1) using Boolean Operators (AND, OR and NOT) along with PICOS (target population, intervention, comparator, outcomes and study design) were used [37].
Medical Subject Headings (MeSH) terms and keywords for PICOS search strategy
Medical Subject Headings (MeSH) terms and keywords for PICOS search strategy
Additional electronic searches are done in the Meta Register of Controlled Trials (mRCT) via the Current Controlled Trials (CCT) database to locate ongoing RCTs with potentially relevant data useful for the present systematic review. The potentially relevant clinical controlled trials and cohort studies (otherwise not indexed in any of the five electronic bibliographic databases and mRCT), electronic searches were supplemented by searching unpublished papers from the OpenGrey (formerly SIGLE) database. The literature searches were additionally supplemented with manual bibliographic searches of relevant systematic reviews, editorials and thesis reports published by the digital libraries of the University of Manchester, University of Central Lancashire and Australian Digital Thesis programmes, including ProQuest. Authors of potentially relevant unpublished reports were contacted by e-mails seeking clarification of their respective studies with the possibility of inclusion in the present review.
The study selection was performed using thePRISMA flowchart (Fig. 1), where returned hits for each electronic bibliographic database were screened by two independent reviewers initially based on title and abstracts. The number of potentially relevant articles was noted, citations were imported into the Endnote citation manager (EndNote X7), and full-text articles were retrieved for further eligibility screening by the two independent reviewers. Studies were included based on the following criteria:
PRISMA flowchart for articles search strategy, screening and eligibility evaluation.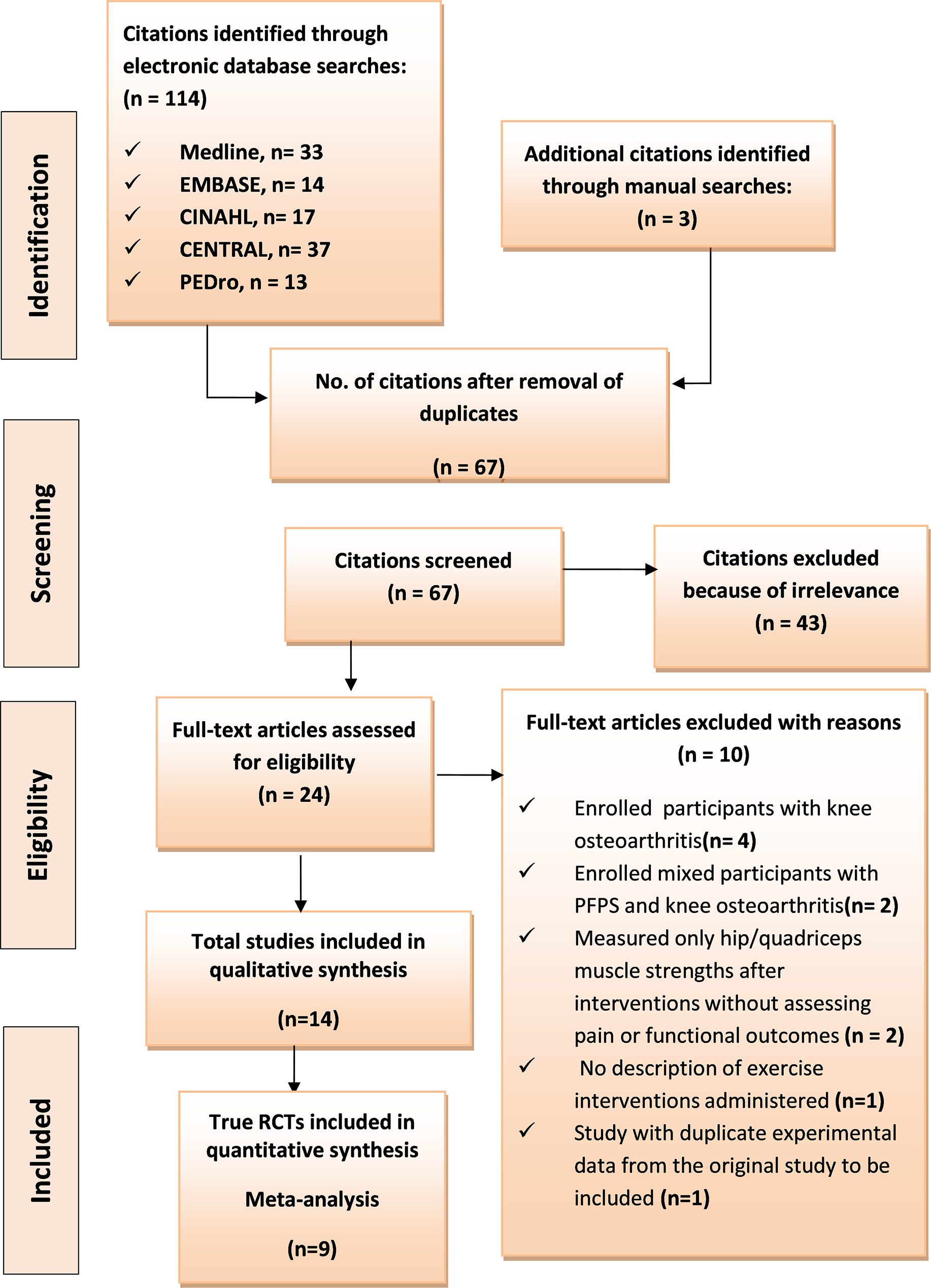
Methodological quality of selected studies rated on McMaster critical review form
RCT
Studies that enrolled adolescents ( Studies involving patients with the confirmed clinical diagnosis of patellofemoral pain presented with anterior or retro patellar knee pain during physical activities, i.e. running, climbing a staircase, squatting, hopping, and kneeling or prolonged sitting. Only controlled clinical trials (RCTs, Non-RCTs, and comparative studies) and cohort studies assessing the effect of hip abductors and/or lateral rotators strengthening on pain and functional outcomes of patients with a confirmed diagnosis of patellofemoral pain. Studies published as books, chapters or conference abstracts or interim results in the mRCT database provided that authors were contacted successfully. Studies comparing strengthening of hip abductors and/or lateral rotators muscles with standard quadriceps strengthening or no exercises. Studies where the intervention group received hip muscles strengthening exercises coupled with quadriceps strengthening provided that the comparator group received only the quadriceps strengthening protocol. Studies measuring pain by VAS, AKPS, 11-point NPRS, PSS, and functional outcomes examined on TAS, LKSS, FIQ, TLKSS LEFS, PFJES, or WOMAC instruments. Studies published in English only were included for the review.
Studies that were not quantitative such as reviews, editorials, commentaries, which merely reviewed the physiotherapeutic benefits of hip muscle strengthening to patients with patellofemoral pain. Studies published more than 20 years ago. Studies that recruited PFP patients with other underlying knee pathologies, such as knee osteoarthritis, cartilaginous knee injuries, meniscal tears or knee surgery. Studies that included the non-exercise co-inter-ventions such as electro-muscular stimulation (electrotherapy), patella taping, and orthotics. Studies reported neither patient pain nor function.
A third senior reviewer was contacted to reach a consensus on any disagreement among the two reviewers regarding the inclusion or exclusion of an article.
The McMaster Critical Review Form for Quantitative Studies was applied to examine the methodological quality of all selected studies for study’s objectives, literature survey, study design, sample population, intervention, outcome measures, results, significance, limitations, and conclusions (Table 2) [14]. Knowing that biases are the main threats to RCTs’ internal and external validity, quality appraisal of RCTs was performed using The Cochrane Collaboration’s ‘Risk of bias’ tool tailored specifically for RCTs [38]. The risk of patient selection bias was examined for the selected RCTs for the sufficiency of random sequence generation and concealment allocation to interventional and control groups. This helped to determine the comparability of the study groups at baseline. The risk of performance bias was evaluated based on measures (e.g. single blinding or double-blinding) employed to ensure study participants and personnel are blinded to interventions and outcomes. The risk of detection bias was assessed to know if the assessors were adequately blinded to patient group allocation. The risk of attrition bias and incorporation bias were examined based on the dropout rate and pattern of participants, handling incomplete outcome data, and the indications of intention-to-treat (ITT) analysis. Finally, the risk of reporting bias is evaluated based on the possibility of selective outcome reporting. The reproducibility of exercise therapies prescribed confounding/modifying effects of co-interventions and the levels of supervision and patient compliance to the prescribed physiotherapy during the trial were also evaluated across the RCTs studies.
Data extraction and qualitative synthesis
Data on effect measures were extracted for baseline patellofemoral pain levels, hip exercise interventions, including the comparator treatment, quantitative assessment of patient outcomes for patellofemoral pain and functions, follow-up duration and post-intervention practices during the follow-up periods. Statistical results (mean differences from baseline and effect measures
Quantitative synthesis (meta-analysis)
Using MedCalc software version 14.10.2 (MedCalc Software Ltd., Ostend Belgium), data from RCTs that provided the mean difference of pain or knee function between the intervention and the comparator groups were pooled by random or fixed-effect models to obtain standardized mean differences. Separate forest plots were generated for pain and knee function outcomes.
Participants allocation in intervention and non-intervention groups with the duration of intervention and frequency of therapy in weeks
Participants allocation in intervention and non-intervention groups with the duration of intervention and frequency of therapy in weeks
Using the PICOS search strategy, the primary electronic searches in the five bibliographic databases returned 114 potentially relevant citations. Through careful screening for duplicates based on titles and authors, 50 citations were excluded. The 43 articles were excluded after careful screening of titles and abstracts from the remaining 64 articles because they were irrelevant. The full texts of the remaining 21 articles were evaluated rigorously for eligibility based on the inclusion and exclusion criteria, and through this process, ten studies were excluded because of the following reasons.
Six articles were excluded because they involved patients with knee osteoarthritis or mixed participants with PFP and osteoarthritis, Two studies were excluded because they focused on hip/quadriceps muscle strengths as the only outcome measure after interventions without assessing pain or functional outcomes, One study appeared relevant but lacked the description of exercise interventions administered, Lastly, one study contained duplicate experimental data from another included original study.
Three potentially relevant studies were identified through manual bibliographic hand searches of three recent systematic reviews [14, 39, 40]. The complete process yielded 14 studies. Ten were controlled clinical trials (CCTs), three were cohort studies, and one was a case series [3, 4, 6, 9, 27, 28, 41, 42, 43, 44, 45, 46, 47, 48]. The three cohort studies met the inclusion criteria for qualitative synthesis. Nine controlled clinical trials were true randomized controlled trials (RCTs) presenting data suitable for quantitative synthesis (meta-analysis) [4, 6, 27, 28, 41, 42, 43, 45, 46]. The literature search strategy and article selection process are summarised in the PRISMA flowchart (Fig. 1) [36].
A total of 383 participants from the 10 CCTs received either hip-strengthening exercises (
Follow-up duration and interval post-intervention pain/functional outcome measures
Follow-up duration and interval post-intervention pain/functional outcome measures
*Month.
In all CCTs, the hip muscles strengthening protocol focused on hip abductors and lateral rotators. The hip exercise protocol included hip abduction against an elastic band while standing, or with weights in side-lying position coupled with lateral hip rotation against an elastic band while seated and hip extension; quadriceps strengthening involved closed kinetic chain exercise or seated knee extension, leg press, squatting and stretching of hamstrings and quadriceps; and, hip-quadriceps strengthening involved the combination of hip-quadriceps protocol. The duration of intervention ranged from 3 to 8 weeks, while the frequency of therapy sessions ranged from 2 to 4 per week (Table 3).
Outcome measures
All CCTs examined both pain and functional outcomes except one, which assessed only pain [45]. The pain was commonly evaluated using 10-cm VAS by all CCTs except two, which used the 11-point NPRS [4, 28]. The pain was evaluated during ascending and descending stairs [4, 28, 45], squatting, usual pain [45],
Evidence table for controlled clinical trials
Evidence table for controlled clinical trials
Descriptions and critique of the reviewed 10 controlled clinical trials (CCTs)
RCT, randomised controlled trial; CCT, comparative control trial; RCT-p, randomised controlled pilot study; CS, cohort study; CSr, case series.
Evidence table for follow-up studies (cohort, case-control, case series and case reports)
Hip versus quadriceps strengthening on PFP .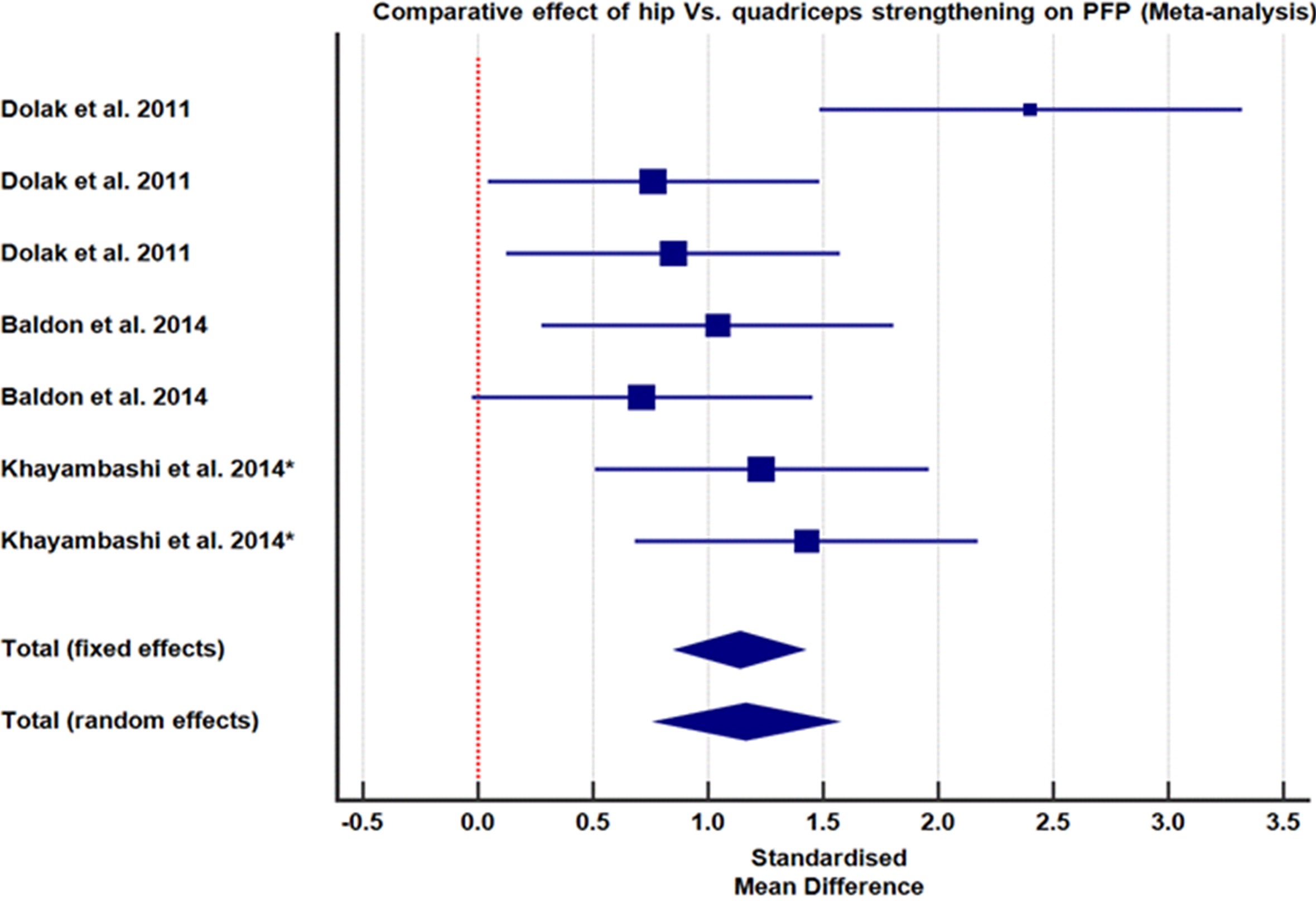
Comparative effect of hip versus quadriceps strengthening on knee function.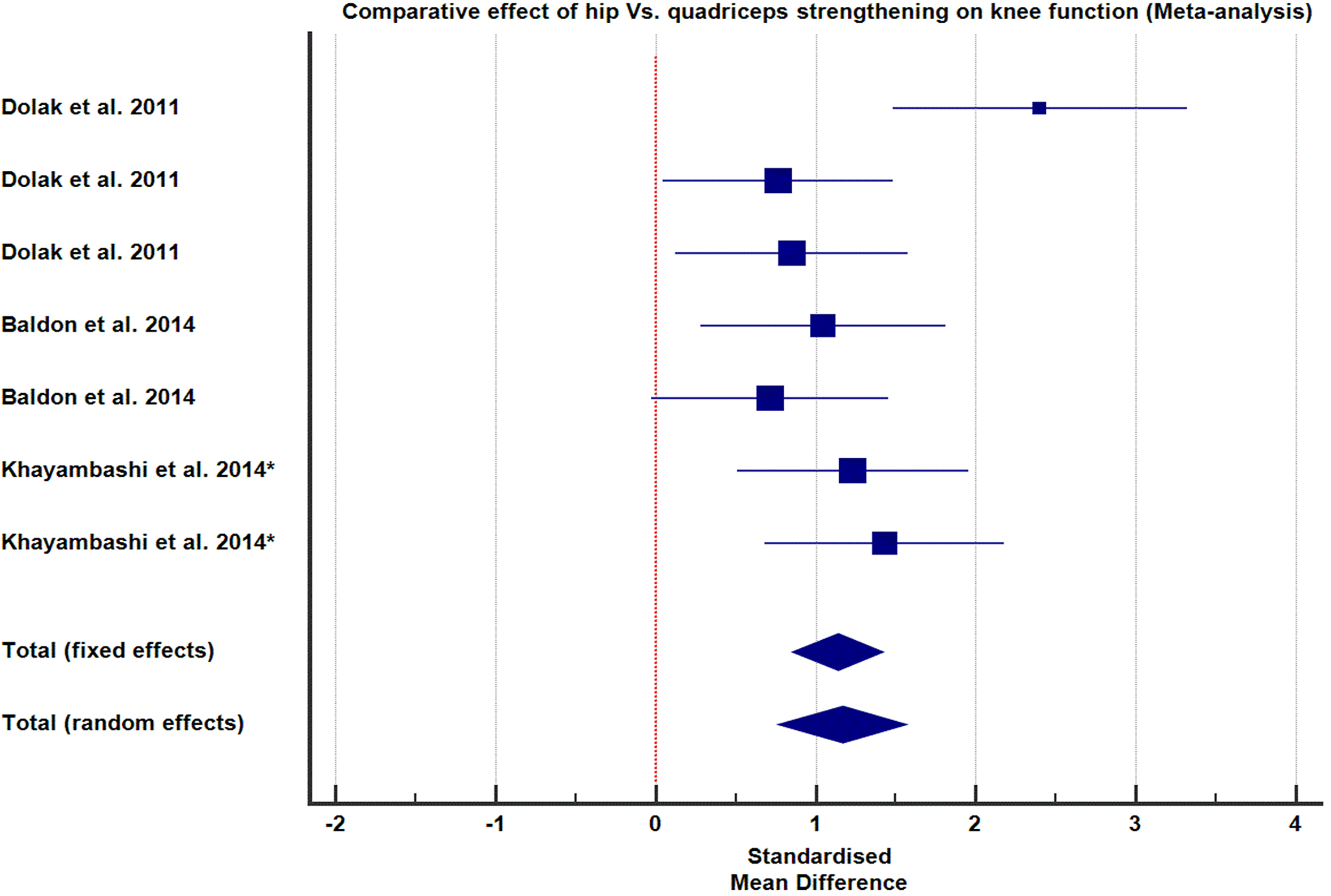
Hip-quad strengthening results in significant pain improvements compared to the standard quadriceps strengthening alone. 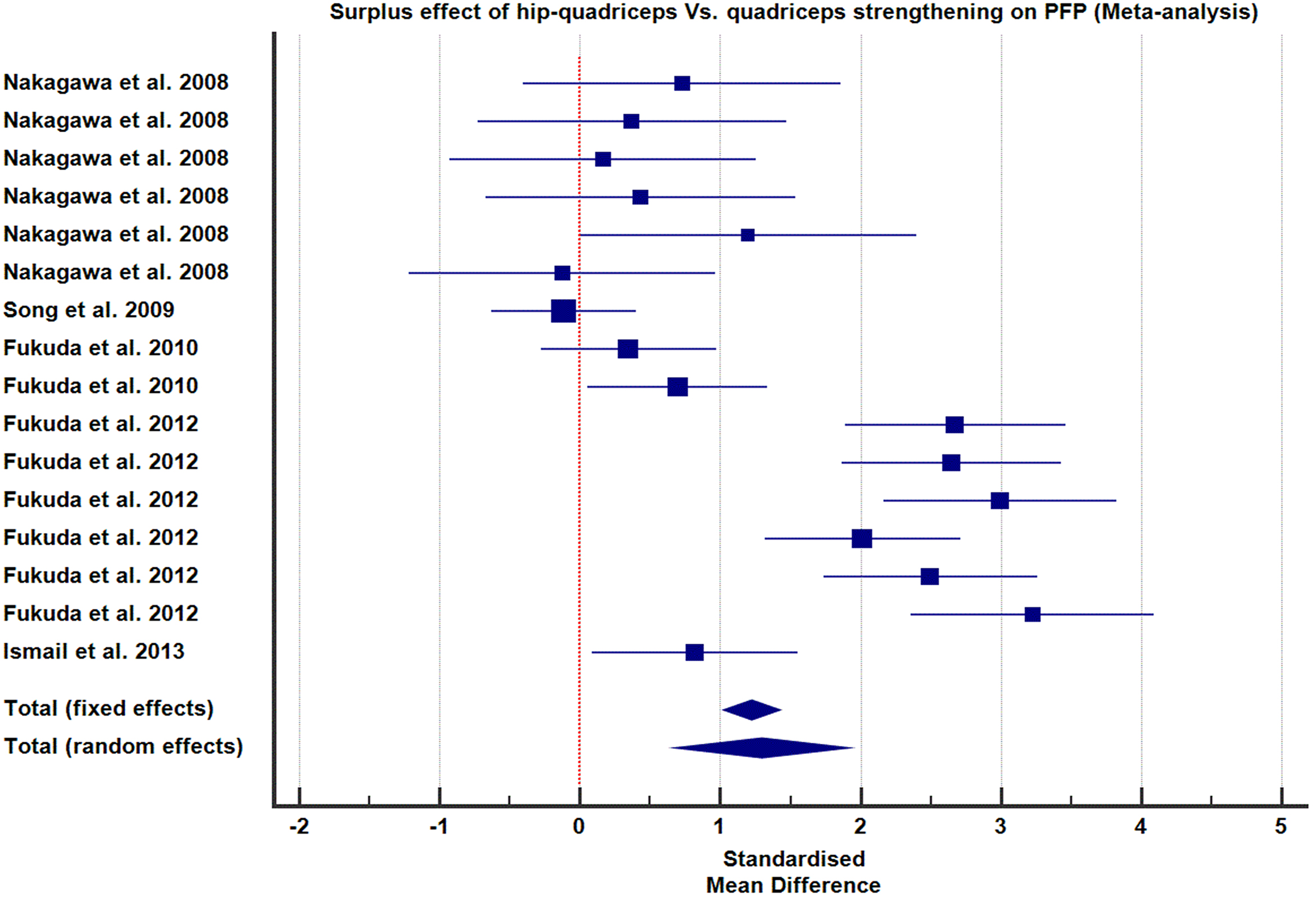
Hip-quad strengthening resulted in a greater functional improvement than the standard quadriceps strengthening alone.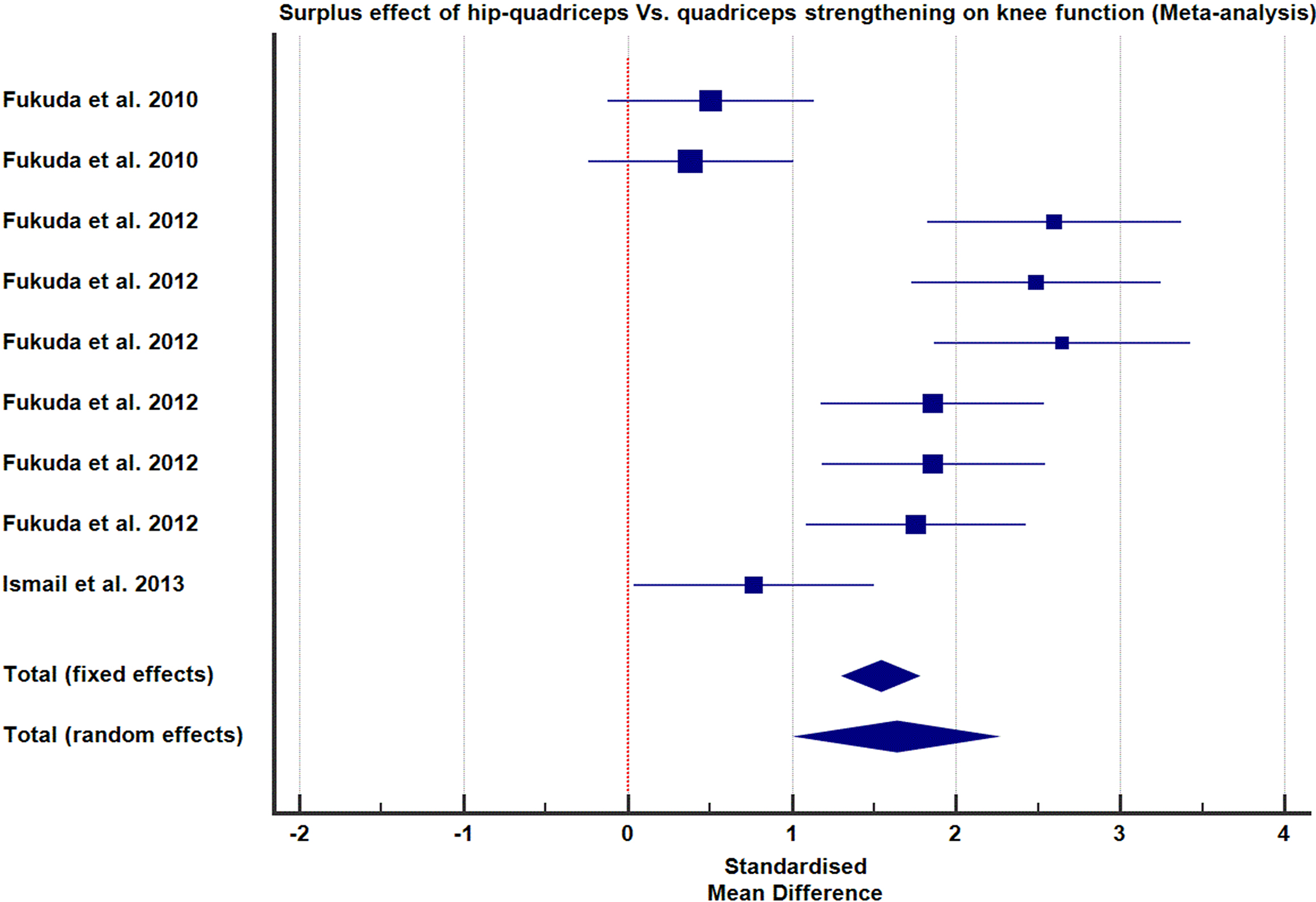
and worst knee pain in the previous week [6, 27, 43, 44, 45, 46]. Functional outcomes were assessed using LEFS [4, 6, 28, 42], AKPS [4, 6, 28, 43], PFJES [41], TLKSS [46] and WOMAC [27, 44].
Post-intervention measures were immediately carried out in all studies, at the end of the intervention period. However, the post- interventional follow-up period ranged from one to twelve months (Table 4).
Critical appraisal
Methodological quality assessment of the 10 CCTs based on the Cochrane Collaboration’s ‘Risk of bias’ tool tailored for RCTs is detailed in Tables 5 and 6 [38].
Cohort and case series studies
The three cohort studies had 88 participants [PFP (
Intervention protocol
In one cohort study, the experimental group was given hip muscles exercise protocol (strengthening of hip abductors and lateral rotators), and the control group received knee exercises. The subjects of the other two cohort studies received quadriceps-strengthening [47, 48]. The duration of intervention ranged between three and six weeks. The case series participants completed an eight-week exercise programme focusing on hip muscles strengthening and improving dynamic misalignment (Table 7).
Meta-analysis (pooled effect size)
The meta-analysis was done to determine the additional effect of hip muscle strengthening as adjunctive therapy to the standard quadriceps strengthening for PFP and knee function.
The comparative effect size of hip versus Quadriceps strengthening on pain and function
Two RCTs [6, 42] and one comparative control trial [44] provided data that compared the effect of the isolated strengthening of hip muscles (abductors and lateral rotators) versus the standard quadriceps strengthening on PFP and knee function. One hundred participants were randomly assigned to receive hip (
Additional effect of hip-quad versus quadriceps strengthening on pain and function
Five RCTs contributed data assessing the additional effect of hip muscle strengthening coupled with quadriceps strengthening compared to the standard quadriceps strengthening alone on PFP and knee function [4, 28, 43, 45, 46]. For both groups (hip-quad and quadriceps alone), 16 data sets were collected from 98 participants. The pooled effects of results are presented in forest plots Figs 4 and 5 as cumulative SMD with 95% CI, under both fixed and random-effects models.
Discussion
Two recent systematic reviews have demonstrated that proximal exercises targeting quadriceps and hip muscles strengthening effectively relieved pain and improved knee function in patients with PFP, both the short- and long-term [14, 40]. However, this systematic review was important to delineate the effect of the isolated strengthening of hip abductors and lateral rotators on pain and knee function in patients with PFP compared to non-exercise interventions, and to identify if hip muscle strengthening is superior to the quadriceps strengthening alone, among them.
Quality of the summarised evidence
The methodological quality of the fourteen studies except five, i.e., [6, 9, 41, 47, 48] included in the present review is excellent because it fulfilled 14 of the 16-item McMaster critical review criteria. The common methodological issue observed in most of the selected studies was the lack of sample size justification (sample size not determined or not achieved) [6, 27, 41, 43, 44, 47]. All studies with sample power inadequacy issues achieved results with statistical significance, suggesting that the measured pain and functional outcomes reflect the comparative effect of the interventions. However, subject contamination in Dolak et al. was evident because hip and quadriceps groups were combined to receive functional strengthening exercises (as co-interventions for the last four weeks of the intervention) [6]. Such subject contamination might have caused patient bias for their pain and functional outcomes, especially if they know the intervention of their cohorts in the opposite arm of the study [49].
This risk of bias is a critical methodological issue in RCTs and warranted supplementary quality appraisal of all RCTs on the Cochrane Collaboration’s Risk of bias tool [38] to highlight methodological flaws (indicative of ‘Risk of bias’ threatening interval consistency) (Table 6). All RCTs except two recruited participants with a confirmed diagnosis of PFP [27, 44]. However, these studies were included because they enrolled patients presented with anterior keen pain based on symptoms matching the inclusion criteria of the remaining RCTs, which recruited patients with a confirmed diagnosis of PFP. Here, 383 participants from all RCTs presented with anterior knee pain associated with prolonged sitting, climbing stairs and descending stairs in the absence of signs/symptoms of meniscal or other intra-articular pathological conditions or history of other knee pathologies, surgeries and injuries. These are classical symptoms for the diagnosis of PFP [14, 40]. However, these symptoms may indicate knee osteoarthritis, but it may not be so likely because patients enrolled in RCTs were not older than 50 years of age and therefore not likely to present with ageing associated PFP [50].
Four studies included a mixed population of both adults and adolescents aged 17 to 50 years [6, 42, 43, 45]. Since adolescents are physically active and at risk of PFP, hence, the inclusion of this age group [50]. To minimize the possibility of recruiting participants with underlying knee pathologies, i.e. knee osteoarthritis, no studies recruited patients with PFP who were older than 50 [50]. The four studies examined only female participants; therefore, the outcome may only be generalized for the female patients with PFP, but not for the males [4, 6, 28, 42]. The three studies [43, 45, 46] included both male and female participants (proportion of females was higher than males), indicative of females being at a greater risk of PFP than males [6]. This may be attributed to females’ lower hip muscle mass compared to males [51]; therefore, females exhibit lower hip muscle strength than males [51, 52].
The symptom duration is a direct measure of severity of PFP that has a significant influence on therapeutic outcome [53]. Therefore, patients with an early diagnosis of PFP are likely to respond well to therapy compared to those with late diagnoses [18]. Thus, symptom duration is a key confounding variable that must be adjusted via the subject’s stratification. In this systematic review, the mean duration of symptoms of participants with PFP in eight studies ranged from 17 to 21 months. However, six studies [27, 41, 42, 43, 44, 45] did not report the mean duration (months) of PFP symptoms. None of the studies performed the subject’s stratification for the PFP severity and symptom duration. This might have positively skewed pain and functional outcomes in patients with a shorter mean duration of symptoms [18]. Additionally, the subject’s characteristics were barely explained in three studies [42, 44, 45] and not detailed in one study [41]. These findings undermine the quality of the summarised shreds of evidence.
Supervised therapeutic exercises enhance participants’ compliance because unsupervised participants may refrain from pain-provoking exercises [18, 54]. Two previous RCTs reported that supervised exercises for PFP result in less pain and better knee function at short- and long-term follow-up than usual care [18, 54]. In the present systematic review, all studies involved exercises administered in physiotherapy facility/rehabilitation setting under supervision by qualified physiotherapists, except two [6, 45], where two-thirds of exercise sessions were self-administered in patient’s homes (unsupervised). At the same time, one-third had rehabilitation under supervision in a facility. It had an important bearing on patient compliance to intervention and the outcome. Even then, results were significant in these two studies, suggesting that partial supervision too can yield clinically significant results.
Isolated hip musculature strengthening
All fourteen studies demonstrated that isolated strengthening exercises of hip abductors and lateral rotators for two to four times per week up to three to eight weeks duration effectively relieve pain and improve knee function compared to quadriceps strengthening and non-exercise interventions. Kooiker et al. reported variations in quadriceps, hip and hip-quadriceps strengthening protocols in selected studies and opined for the unavailability of standardized protocols for PFP [40]. The common hip exercise protocol included hip abduction against an elastic band while standing and with weights in a side-lying position coupled with lateral hip rotation against an elastic band while seated and hip extension (3 sets of 10 repetitions). Conversely, quadriceps strengthening in all studies generally involved weight-bearing and non-weight-bearing exercises such as closed kinetic chain exercises, seated knee extension, leg press, squatting and stretching of hamstrings and quadriceps (3 sets of 10 repetitions).
The hip protocol generally improved pain and knee function after three to eight weeks of training, with long-term effects observed as late as twelve months post-intervention [28]. Four studies evaluated the comparative therapeutic value of quadriceps versus hip muscle strengthening in treating PFP [6, 41, 42, 44]. One study by Khayambashi et al. reported superiority of hip muscles strengthening strategy over the quadriceps strengthening for both pain and functional improvement in PFP [44]. The remaining three studies argued that isolated hip and quadriceps strengthening strategies have comparable therapeutic value for the PFP [6, 41, 42]. However, a meta-analysis of the effect measures (pain and function) as measured on VAS and LEFS or WOMAC revealed that hip strengthening significantly favours the standard quadriceps strengthening (
Additional therapeutic effect of hip muscles strengthening
Although the proximal strengthening exercises involving quadriceps and hip muscles are commonly effective in treating PFP, Kooiker et al., Peters and Tyson argued that a combination of hip-quadriceps strategy could add to the therapeutic outcome for patients with PFP [6, 14, 40, 41, 42]. The present systematic review included five RCTs to examine the additional therapeutic outcome of hip-quadriceps strengthening exercises over the standard quadriceps [4, 28, 43, 45, 46]. Except for one, all studies; supported that the hip-quadriceps strategy was superior to the standard quadriceps [46].
The findings of these five RCTs have both internal and external validity and are, therefore, acceptable. Furthermore, meta-analyzed data of these five studies strongly indicated that quadriceps coupled with hip muscle strengthening has significant additional therapeutic benefits over the conventional quadriceps or hip exercises in the treatment of PFP (
Limitations
The summarised evidence supported by meta-analyses indicates that strengthening hip muscles is effective in treating PFP for pain and knee function of physically active male/female adolescents and adults. However, a few important limitations must be noted;
This systematic review and meta-analysis initially were intended to review a minimum of 20 studies to examine the therapeutic outcome of hip muscle strengthening versus quadriceps alone on pain and knee functions for patients with PFP. The expanded literature search yielded only 14 studies that are adequate for systematic review, limiting the strength and generalisability of the summarised findings over a wider population of patients with PFP. Avraham et al. study (included in this review) used a non-exercise (electrotherapy) as a co-intervention that might have uni-directionally augmented the therapeutic effects [41]. Although the proportion of females to males is higher in all studies (included in this review), this may not be considered as a limitation to generalisability for a wider group of patients with PFP because it truly reflects the characteristics of patients with PFP that would be encountered in day-to-day clinical practice.
The evidence from the present review has important implications in routine clinical practice for the patients with PFP:
Strong shreds of evidence favour hip muscle strengthening exercises for two to four times a week, up to three to four weeks, to have effective therapeutic outcomes compared to standard quadriceps strengthening exercises alone in patients with PFP. This implies that therapists should consider hip muscle strengthening as a standard therapeutic measure while treating patients with PFP. Meta-analysis of the effect measures (both pain and function) has strongly supported that hip muscles coupled with quadriceps (hip-quad) strengthening have superior therapeutic effects than the individual isolated hip or quadriceps strengthening exercises. This evidence strongly implies that therapists should consider a combination of hip and quadriceps strengthening exercises to treat patients with PFP. However, this may imply longer duration of intervention lasting 6 to 8 weeks and more sessions per week that may influence patients’ compliance to intervention, especially if prescribed as self-efficacy [57]. In the present review, only one study [28] out of fourteen had followed patients up to twelve months, which was a good attempt to determine the long-term therapeutic effect of hip versus quadriceps strengthening exercises on PFP and knee function. This indicates evidence to be generalized only for the short-term instead of long-term pain and functional outcomes.
Must consider stratification of patients/results based on the symptom duration before the intervention to eliminate the effect of time-delay modification on pain and functional outcomes following hip muscles strengthening in patients with PFP.
Conclusion
This systematic review and meta-analysis indicate that isolated strengthening of hip abductors and lateral rotators have therapeutic benefits compared to quadriceps strengthening alone for the treatment of PFP. It is also clear that the hip-quadriceps strategy gives a beneficial therapeutic outcome than isolated quadriceps or hip muscle strengthening. Therefore, we recommend developing a hip-quadriceps exercise strategy for the treatment of PFP to encourage improved compliance, even in unsupervised patients.
Footnotes
Conflict of interest
The authors have no financial or non-financial conflicts of interest to declare that are relevant to the content of this article.
Funding
No funds, grants, or other support was received for conducting this study.