
Abstract
Background:
The Kujala score is a useful diagnostic tool to evaluate patellofemoral pain syndrome (PFPS). However, no validated Indonesian version of the Kujala score has been available.
Purpose:
To develop and validate an Indonesian version of the Kujala score.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
This was a cross-sectional study to develop an Indonesian version of the Kujala score by using a forward-backward translation protocol. The resulting questionnaire was given to 51 patients diagnosed with PFPS. The validity of the questionnaire was evaluated by correlating the final score with the Indonesian version of the 36-Item Short Form Health Survey (SF-36). Reliability was measured by evaluating the internal consistency (Cronbach alpha) and test-retest reliability (intraclass correlation coefficient [ICC]).
Results:
The Indonesian version of the Kujala score had a positive correlation with the physical components of the SF-36. The internal consistency was fairly high (α = .74), and the test-retest reliability was excellent (ICC, 0.996).
Conclusion:
The Indonesian version of the Kujala score was proven to be a valid and reliable tool to diagnose PFPS. Future epidemiological studies could implement this score to find the prevalence of PFPS in Indonesia. Further, ensuing studies could explore the application of this scoring system in posttreatment and postoperative settings.
Patellofemoral pain syndrome (PFPS) is defined as a nontraumatic, diffuse anterior knee pain aggravated by the loading of the knee joint, such as during jumping, squatting, running, and stair climbing and descending. 3 PFPS is one of the most prevalent causes of knee pain, affecting as much as 22.7% of the world population. 18 This condition is found in all age groups, especially adolescents and adults age 50 to 59 years. 7,16,17 There is a 2:1 female predominance regarding both the incidence and prevalence of PFPS. 2
Past studies have proposed some diagnostic criteria for this condition; however, none gave satisfactory consistency. 15 Thus, Kujala et al 9 developed the Anterior Knee Pain Scale (AKPS), known as “the Kujala score,” an independent questionnaire that aims to assess the severity of symptoms and physical limitations in patients with PFPS. The Kujala score is one of the most commonly used assessments that has been developed for this purpose. It is a self-administered questionnaire for patients with PFPS that consists of 13 questions that relate to specified activities, pain severity, and clinical symptoms. 9 The sensitivity of this tool is 80%, and the specificity is 90%. 12 The other diagnostic tool recently used to diagnose PFPS is the Survey Instrument for Natural History, Etiology, and Prevalence of Patellofemoral Pain Studies (SNAPPS) questionnaire. The SNAPPS questionnaire has also shown high sensitivity and specificity (>90%). 22 However, this online questionnaire is less widely used compared with the Kujala score and has been used only in an epidemiological study in China.
The Kujala score has been translated into several languages, including Persian, Turkish, Thai, and German. 1,4,6,10,13 To date, there is no self-administered PFPS measurement in the Indonesian language that has been used and validated for the population. The purpose of this study was to develop an Indonesian version of the Kujala score and evaluate the validity and reliability of this version.
Methods
Study Design and Sample
This was a descriptive cross-sectional study of patients with PFPS. The participants consisted of 51 patients with PFPS from the knee outpatient clinic of our hospital; there was no loss to follow-up in this study. The inclusion criteria were patients with anterior knee pain who were diagnosed with PFPS, age 13 to 60 years, and fluent in the Indonesian language. The diagnosis of PFPS was made by an orthopaedist from our hospital (K.Y.P.) through history taking and physical examination. The diagnostic criteria were anterior knee pain, aggravated by partial squatting and persisting for more than 2 weeks. Exclusion criteria were patients who were younger than 13 or older than 60 years and those with knee disorders besides patellar instability. Data collection was performed from July 2019 to August 2019. This study was reviewed by an institutional review board and received ethical clearance. Figure 1 depicts the patient selection and study process.

Flowchart of the study process.
Development of the Indonesian Version of the Kujala Score
We received permission to undertake translation of the Kujala score from the original authors, Kujala et al. The translation process was done using a forward-backward translation protocol.
The translation was conducted by 2 independent translators: an orthopaedics expert and another person who was not a health care worker. The 2 versions were then compared and discussed to correct any discrepancies. The resulting Indonesian translation was then translated back to English by another orthopaedics expert and another non–health care worker (different from the people who conducted the forward translation). The resulting back-translation was assessed to ensure similarity to the original English version.
Further, 3 orthopaedics experts reviewed the resulting Indonesian translation. It was also assessed by an expert committee consisting of translators, health care workers, and academic methodology experts in addition to all study authors. The committee’s consideration was used to design a preliminary version of the Indonesian Kujala score. The preliminary version was translated back to English and sent to Professor Kujala to be reviewed and corrected.
Preliminary Testing of the Indonesian Version of the Kujala Score and Finalization
The preliminary version was tested on 10 participants with and without knee pain to assess understanding and the interpretation of each item. After all necessary changes were processed, the finished Indonesian version of the Kujala score was finalized by the committee.
Research Procedure
The Indonesian version of the Kujala score was used concurrently with the Indonesian version of the 36-Item Short Form Health Survey (SF-36). The Kujala score was originally developed to evaluate symptoms and functional disability in patients with patellofemoral disorder. The scoring system consists of 13 questions regarding functional aspects, including limping, support, walking, stair descending and ascending, squatting, running, jumping, prolonged sitting with the knees flexed, pain, swelling, kneecap movement, thigh atrophy, and flexion deficiency. The maximum score is 100, with a higher score signifying a better result. 9
The SF-36 is routinely used to assess health-related quality of life. The SF-36 evaluates 8 components: physical functioning, role physical, bodily pain, general health, vitality, social functioning, emotional role, and mental health. The first 4 components evaluate the physical health/physical component summary (PCS), and the other 4 evaluate the mental health/mental component summary (MCS). The maximum score is 100, and a higher score signifies higher quality of life. The Indonesian version was developed in a previous study. This scoring system is widely used for several musculoskeletal problems, as it evaluates general health aspects and is applicable to all age groups. 14,23
Statistical Analysis
The validity of the Indonesian version of the Kujala score was assessed by correlating its result with the result of the Indonesian version of the SF-36. The final score of the Indonesian Kujala score was correlated with the 8 components of the Indonesian SF-36, both the PCS and the MCS and the final score. The correlation was conducted by use of the Pearson correlation test. The result was considered statistically significant if the P value was less than .05.
The reliability of the Indonesian Kujala score was determined by evaluating the internal consistency and test-retest reliability. Internal consistency was measured by determining the Cronbach alpha. The test-retest reliability was evaluated by measuring the intraclass correlation coefficient (ICC). The test and retest procedure were performed 7 days apart. This interval was chosen because the clinical symptoms of patients with PFPS do not generally change in such a short period of time. The patients received oral medication and physiotherapy treatment during the 7-day interval. All statistical analysis was performed via SPSS (Version 25.0; SPSS Inc).
Results
This study included 51 patients, all of whom had anterior knee pain and had been diagnosed with PFPS by the orthopaedist through history taking and physical examination. All of the patients were treated nonoperatively by pharmacologic agents (analgesics) and physical rehabilitation. Of the patients, (66.7%) were male and of reproductive age, and almost 40% were 20 to 29 years old. Table 1 depicts the demographic characteristics of the patients.
Demographic Characteristics of the Patients (N = 51)

The Pearson correlation test showed significant correlations between the final score of the Indonesian version of the Kujala score and the physical components of the SF-36. However, an exception was found regarding the general health component. Moreover, a positive correlation was observed between the Indonesian Kujala score and the total score of the SF-36. A strong correlation (r > 0.6) was found regarding physical functioning, pain, and the PCS.
Only 1 mental component had a positive correlation with the Kujala score (social function), but the correlation was weak (r = 0.29). The other mental components did not have a significant correlation with the Kujala score. Table 2 depicts the correlation test results.
Results of the Pearson Correlation Test Between the Indonesian Version of the Kujala Score and the SF-36
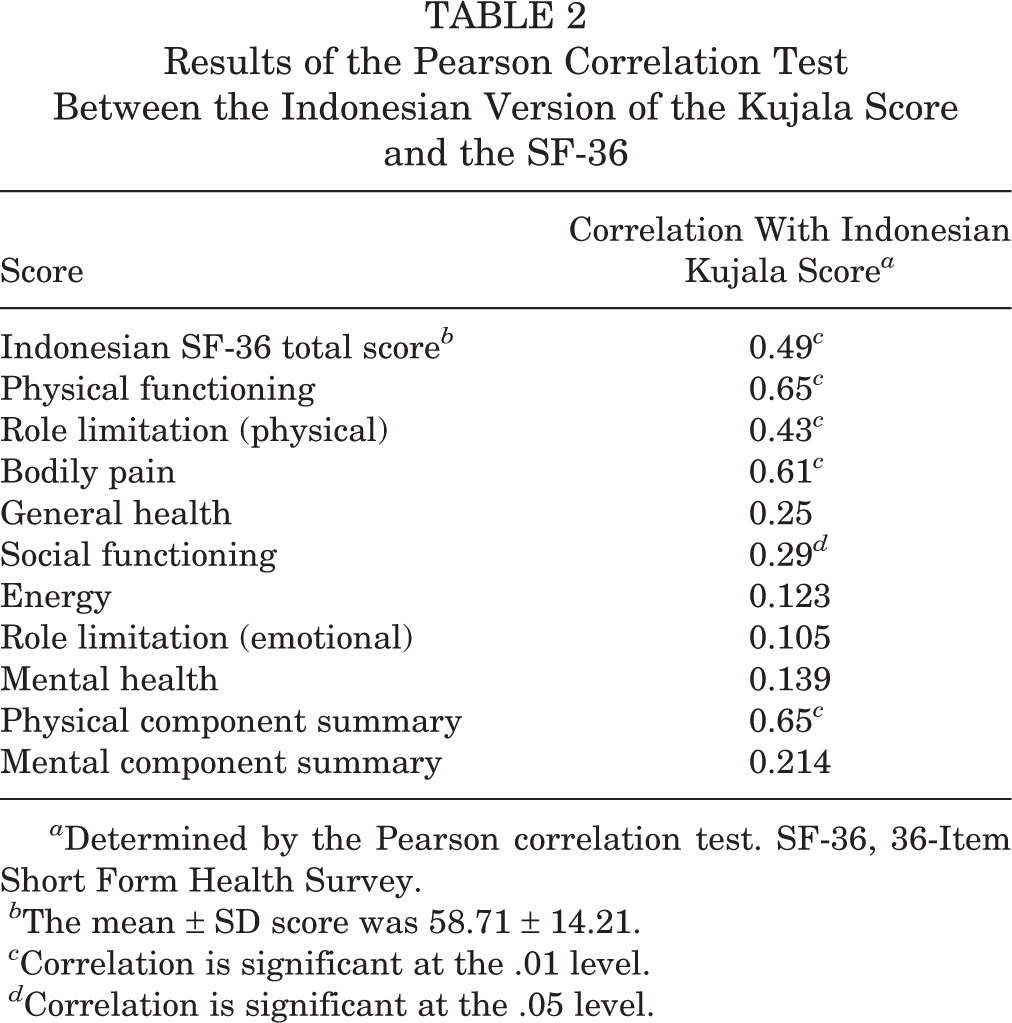
a Determined by the Pearson correlation test. SF-36, 36-Item Short Form Health Survey.
b The mean ± SD score was 58.71 ± 14.21.
c Correlation is significant at the .01 level.
d Correlation is significant at the .05 level.
The internal consistency was measured by calculating the Cronbach alpha. The internal consistency was good, with a Cronbach alpha of 0.74. The test-retest reliability was measured by calculating the ICC, which was 0.996. In addition, no floor or ceiling effects were observed in the final score, as no patient achieved the lowest score of zero or the highest score of 100. The lowest score achieved was 18 (n = 1), and the highest score was 98 (n = 1).
Discussion
PFPS accounts for 25% of all causes of anterior knee pain, and its diagnosis is challenging given the complex causes and lack of a specific test. 5 Kujala et al 9 developed a scoring system to assess the severity of functional symptoms in patients with anterior knee pain. The Kujala score has proven to be valid and reliable in the diagnosis and screening of anterior knee pain. 3,8
The Indonesian version of the Kujala score showed positive correlations with the physical functioning, bodily pain, and PCS sections of the SF-36 Indonesian version. This result is understandable, as the Kujala score was designed to diagnose a pain-related syndrome. In addition, we found a positive correlation with the total score of the SF-36.
With regard to the mental components of the SF-36, a positive correlation was observed only in the social functioning component. This result may be explained by the fact that the Kujala score does not measure any mental or emotional components. The same result was observed in the validity test of the German version of the Kujala score, although the validation study compared the Kujala score with the SF-12. 4 However, some studies suggest that the results of the SF-12 and SF-36 are comparable. 11,21 A different result was described by Apivatgaroon et al, 1 in which the Thai version of the Kujala score showed positive correlations with both physical and mental components of the SF-36. However, the correlations of the physical components were stronger than the correlations of the mental components. The overall results of the present study suggest that the Indonesian version of the Kujala score is valid to diagnose PFPS.
The test-retest reliability of the Indonesian Kujala score showed excellent reliability (ICC, 0.996). This is comparable with the Thai version (ICC, 0.908), 1 the German version (ICC = 0.93), 4 the Spanish version (ICC, 0.99), 6 the Persian version, 13 and the English version (ICC, 0.81). 3 The internal consistency was measured by the Cronbach alpha. The internal consistency was good, with a Cronbach alpha of 0.74. Although this value is still lower compared with the Thai version (α = 0.95), 1 the Spanish version (α = .80), 6 the German version (α = .87), 4 and the Dutch version (α = .78), 20 it is still considered fairly high. 19 The content validity of the Indonesian Kujala score was also good, as no floor or ceiling effects were observed.
The current study had some limitations. We compared the Indonesian version of the Kujala score with only 1 other scoring system (SF-36). However, until now, no other validated tool in the Indonesian language has been available to evaluate knee pain or function. Further, the patients received treatments during the 7-day test-retest interval, which may have altered their symptoms, although we told the patients to describe their initial symptoms during the retest. Nevertheless, this study is the first validation study for a tool that evaluates anterior knee pain in Indonesian patients.
Conclusion
The Indonesian version of the Kujala score is both valid and reliable. Thus, it is applicable to assess PFPS in the Indonesian population as an objective measurement tool.
Future investigators could implement the Indonesian version of the Kujala score to conduct an epidemiological study, determining the prevalence and causes of PFPS in Indonesia. The Indonesian Kujala score could be used to evaluate PFPS after procedures such as anterior cruciate ligament reconstruction and total knee arthroplasty.
Footnotes
Acknowledgment
We extend our gratitude to Professor Urho Kujala, MD, PhD, for allowing us to translate and validate the Kujala score into the Indonesian language.
Final revision submitted October 31, 2019; accepted December 17, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Saiful Anwar General Hospital-Universitas Brawijaya Institutional Review Board.