
Abstract
BACKGROUND:
Muscle energy technique (MET) is found to be effective for the management of neck pain and in addition to the muscle specific approach, clinicians may also adopt movement specific approach for METs. However, the literature is deficient in terms of comparison of muscle specific and movement specific METs in the management of mechanical neck pain.
OBJECTIVE:
To compare the effects of muscle specific and movement specific METs in the management of mechanical neck pain.
METHODS:
A single blind parallel design randomized controlled trial was conducted on 66 participants with mechanical neck pain ranging from 40–80 mm on visual analogue scale (VAS), aged between 19–44 years with pain and limitation on cervical motion. Once included, the participants were randomly allocated to two groups, namely the muscle specific MET group and the movement specific MET group. Outcome measures included VAS, Neck Disability Index (NDI) and cervical range of motion (ROM).
RESULTS:
No significant differences (
CONCLUSIONS:
Both muscle specific and movement specific METs are effective in the management of mechanical neck pain, with no significant differences between the two treatment techniques.
Introduction
Neck is the most common site of musculoskeletal discomfort, the occurrence of which has been reported to be as high as 75.7% in healthy young adults [1, 2]. The buildup of this discomfort leads to neck pain, with a 1 year prevalence ranging from 16.7% to 75.1% [3, 4]. Neck pain can result in functional disability, which may be influenced by factors such as self-efficacy, psychological distress, and fear-avoidance beliefs [5]. One of the most initial and common causes of neck pain includes contractile dysfunction including muscular imbalances, muscular weakness, increased muscle tension and muscle shortening. They are not only the major culprits in impaired postures such as upper crossed syndrome and forward head posture [6, 7, 8], but may also lead to neck pain, decreased cervical range of motion [9] and increased joint reaction forces in the facet and intervertebral joints, eventually leading to degenerative joint disorders.
Physical therapy has been found to be effective in the management of mechanical neck pain [10, 11, 12, 13, 14, 15], with manual therapy and exercise being the most preferred and commonly practiced techniques [16]. There are different types of manual therapy techniques such as joint mobilization, neural mobilization and muscle energy technique (MET) focusing on joints, nerves and muscles respectively [10, 12, 13, 17, 18, 19]. Among manual therapy techniques, METs have not only been observed to be effective in improving pain, function, range of motion, muscle strength and cervical curvature [10, 12, 13, 17] in persons with neck pain, but is also reported to be superior to static stretching in the management of mechanical neck pain [10, 12, 17]. One of the proposed reasons for the superiority of METs over static stretching has been the fact that static stretching only addresses the passive component of the muscle tone whereas METs address both active and passive tone components using the mechanism of either autogenic or reciprocal inhibition [10, 12]. Furthermore, studies have shown autogenic inhibition MET to be more effective than reciprocal inhibition MET in the management of mechanical neck pain [10, 12].
Even though, from a physiological point of view, METs are conventionally muscle specific, being applied to an individual muscle at a time and based on its individual function such as anterior, middle and posterior Scaleni, Sternocleidomastoid, Levator Scapulae and upper fibers of Trapezius in the neck region, the clinical goal of using Muscle Energy Techniques (METs) in patients with mechanical neck pain is to improve the range of motion in the neck, including flexion, extension, lateral flexion, and rotation. This goal is important both from the perspective of clinicians and patients. For this reason, some clinicians may follow a movement specific approach, instead of a muscle specific approach, as the ultimate goal is to improve range of motion. However, it is imperative to point out that there is no existing evidence regarding the comparison of muscle specific and movement specific METs in the management of mechanical neck pain, which is the aim of this study. Thus, in the current study it was hypothesized that there is a statistically significant difference between the effects of muscle specific as compared to movement specific MET on neck pain, range of motion and neck disability in persons with mechanical neck pain.
Methods
Study design
CONSORT diagram (scheme of study).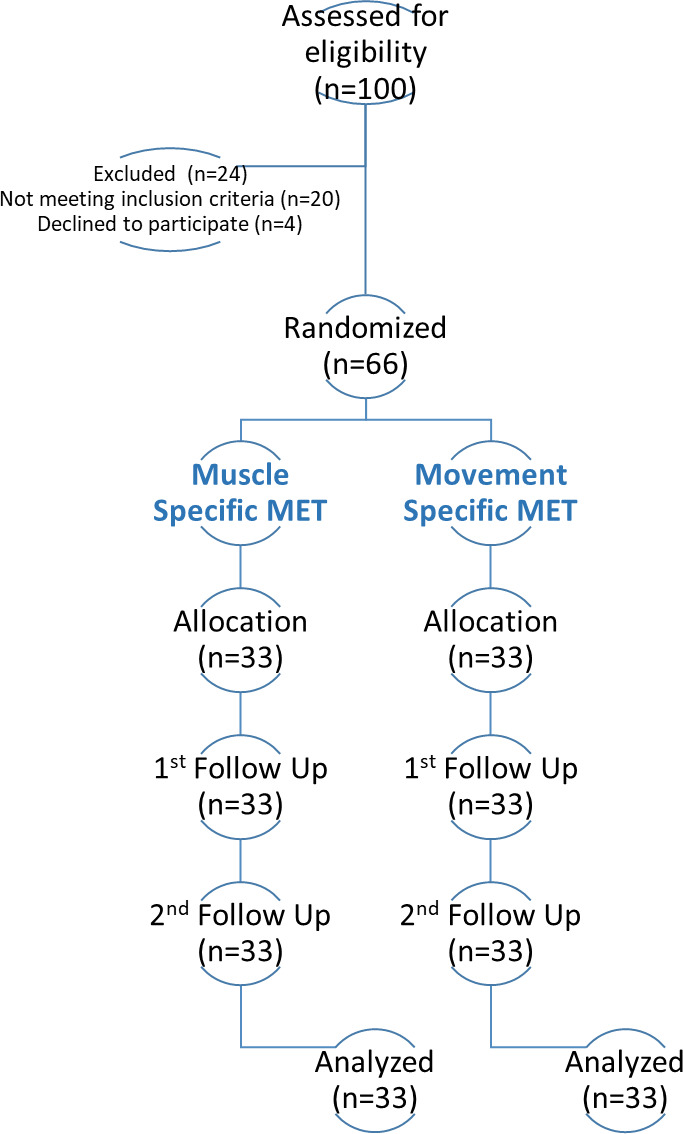
A single blind parallel design randomized controlled trial was conducted on 66 participants at Foundation University Islamabad (FUI), from April 2017 to January 2019. The participants were blind to the group allocation.
Ethical approval was acquired from Foundation University Islamabad Ethical Review Committee and Brainstorm Research Ethical Review Committee in accordance with the Declaration of Helsinki and CONSORT guidelines. Informed consent was taken from all participants before inclusion in the study and the participant information was kept confidential.
Sample size calculation
Sample size was calculated using a minimal detectable change of 10.2 for Neck Disability Index (NDI) [20], with a pooled standard deviation of 13.19, a confidence level of 0.05 and a power of 0.8, based on which a total sample size of 56 was calculated, using the Harvard Sample Size Calculator [21]. However to account for potential drop outs a sample of 66 participants was included in the study.
Participant selection and random allocation
A total of 66 participants with mechanical neck pain ranging from 40–80 mm on visual analogue scale (VAS), aged between 19–44 years with pain and limitation on cervical motion were included in the study via purposive sampling. Participants with a positive history of fracture, surgery or trauma in the neck region, cervical radiculopathy, myelopathy, spondylosis, or syringomyelia, thoracic outlet syndrome, infection, any malignancy, inflammatory, or rheumatic disorders, and vascular syndromes such as vertebrobasilar insufficiency were excluded from the study [10, 12]. The participants were first screened by a medical practitioner. Once included, the participants were randomly allocated into two groups, namely the muscle specific MET group and the movement specific MET group, via coin toss method. The participants were not aware of their allocated treatment group, nor were they aware of the treatment other participants were receiving to ensure blinding. Treatment practitioner and outcome assessor was the same person and was not blind to the participant allocation.
Intervention
All participants were given 10 minutes of Trans Cutaneous Electrical Nerve Stimulation in combination with hot pack, followed by 3 sets of Maitland’s unilateral postero-anterior glide (10–15 oscillations) regardless of the group they were allocated to [10, 12, 18]. After the aforementioned protocol the participants of both the groups were given 3–5 repetitions of post-isometric relaxation (PIR) MET with 30% to 50% of maximal isometric contraction for 7 to 10 seconds, followed by 5 seconds of rest and then a stretch was maintained for 10 to 60 seconds [10, 12, 22, 23]. However, the approach of PIR was either muscle or movement specific based on the treatment group.
In the muscle specific MET group, the participants were given post-isometric relaxation MET targeted at muscles of the neck region that are prone to get short, including anterior, middle and posterior Scaleni, Sternocleidomastoid, Levator Scapulae and upper fibers of Trapezius muscle [10, 12]. In the movement specific group, the participants were given post-isometric relaxation MET targeted at specific movements of the cervical spine including flexion, extension, rotation and lateral flexion. The participant was asked to perform a specific movement such as rotation towards the right side, and then the participant was instructed to try to perform a movement towards the opposite side (rotation towards left) using 30% to 50% of maximal force while the therapist resisted the movement for 7 to 10 seconds, and then the participant was asked to relax, following which the therapist would move the head and neck towards the point of restriction (rotation towards right) where the therapist would maintain a stretch for 10 to 60 seconds. All participants received consecutive treatment sessions for 5 days.
Outcome measures
Participant characteristics at baseline
Participant characteristics at baseline
BMI, body mass index; MET, muscle energy technique; VAS, visual analogue scale; NDI, neck disability index; ROM, range of motion; S.D, standard deviation.
The outcome measures included VAS for pain, Neck Disability Index (NDI) for function and goniometry for cervical range of motion (ROM). Pain and ROM were measured at baseline, after 1
The VAS is a pain assessment tool consisting of a 0–100 mm or 0–10 cm line. Patients were instructed to indicate their level of pain severity by placing a mark on the line, with higher scores representing greater levels of pain. VAS has been established as a valid and reliable instrument for evaluating neck pain, and is frequently utilized as an outcome measure. A minimum clinically important difference of 4.6 to 21.4 mm has been documented in VAS scores for neck pain, indicating its sensitivity to changes in pain intensity [24].
Cervical Range of Motion (ROM)
The ROM of the cervical spine was quantified using a universal goniometer. All pre- and post-treatment ROM measurements were performed in sitting position by the same investigator. The Intra-class Correlation Coefficient (ICC) for the intra-rater reliability of universal goniometer has been observed to be 0.83, 0.86, 0.84–0.85 and 0.78-0.90 [25], and the interrater-reliability has been observed to be 0.78, 0.83, 0.77–0.83 and 0.84–0.87 for cervical flexion, extension, lateral flexion and rotation respectively [26]. Research has shown decreased ROM to be related with poorer outcomes and greater or optimum ROM is linked with more favorable outcomes in neck pain [27].
Neck disability index (NDI)
NDI is a 10 item self-reported condition specific functional status questionnaire and is the most frequently used self-reported outcome measure for patients with neck pain [28] with an established validity and a test-retest reliability of
Statistical analysis
The data was analyzed using Statistical Package for Social Sciences (SPSS v 21). Shapiro Wilk and Kolmogorov Smirnov tests were used to determine the normality of data. Independent
Results
A total of 66 participants were included in the study with 18 males and 48 females, with an equal male to female ratio in both groups. No significant differences were observed between the two groups at base line in terms of age, weight, height, body mass index (BMI), VAS, NDI and ROM (Table 1).
Pain and function
Inter group comparison after 1
treatment session
Inter group comparison after 1
MET, muscle energy technique; VAS, visual analogue scale; NDI, neck disability index; ROM, range of motion; S.D, standard deviation.
Inter group comparison after 5
MET, muscle energy technique; VAS, visual analogue scale; NDI, neck disability index; ROM, range of motion; S.D, standard deviation.
A significant difference (
A significant difference (
Pre- and post-treatment analysis muscle specific MET
Pre- and post-treatment analysis muscle specific MET
VAS, visual analogue scale; NDI, neck disability index; ROM, range of motion; S.D, standard deviation.
Pre- and post-treatment analysis movement specific MET
VAS, visual analogue scale; NDI, neck disability index; ROM, range of motion; S.D, standard deviation.
The purpose of the current study was to compare the effects of muscle specific and movement specific METs in the management of mechanical neck pain in terms of pain function and range of motion. In the current study post isometric relaxation (PIR) MET, which is an autogenic inhibition MET was administered to muscle specific as well as the movement specific MET group, as previous studies have shown autogenic inhibition PIR-MET to be superior to both static stretching and reciprocal inhibition MET in the management of mechanical neck pain [10, 12, 30]. In terms of pain both muscle specific and movement specific METs were found to be effective in improving pain, immediately after the 1
In terms of function both muscle specific and movement specific METs were found to be effective in improving NDI scores after 5 consecutive treatment sessions. This finding was in accordance with the findings of the previous studies showing METs to be effective in improving function in persons with mechanical neck pain as well as cervical spondylosis [10, 13, 17, 31]. Previous studies have shown METs to be even more effective than stretching in improving function and neck related disability in persons with mechanical neck pain [10, 17], however one study conducted on persons with cervical spondylosis showed conventional stretching to be more effective than MET [31] in terms of function and neck related disability Moreover, studies has also shown autogenic inhibition MET to be more effective than reciprocal inhibition MET in terms of improving neck related disability, function and isometric muscle strength in persons with mechanical neck pain [10, 12]. Furthermore, no evidence has been identified regarding the comparison of the effects of muscle specific and movement specific METs on function and neck related disability in persons with mechanical neck pain, however the current study has shown no significant differences between the two treatment methods in terms of NDI.
In terms of cervical range of motion both muscle specific and movement specific METs were found to be effective when measured immediately after 1
Moreover, research has also shown METs to be effective in improving cervical curvature and isometric muscle strength in persons with mechanical neck pain [12, 13], with autogenic inhibition METs being more effective than reciprocal inhibition MET [12], however those outcomes were not observed in the current study. The results of the present study indicate that both muscle-specific and movement-specific muscle energy techniques (METs) are effective interventions for the management of mechanical neck pain, with no significant differences observed between the two groups. It is possible that in direction-specific muscle energy techniques, specific muscle fibers are being targeted in all directions, which could explain the lack of significant differences observed between muscle-specific and movement-specific METs. Additionally, the observed improvements in range of motion may favor direction-specific METs, as the technique is applied in specific movement directions (such as flexion, extension, side bending, and rotation) and range of motion is subsequently measured in those same directions. Therefore, it may have been more appropriate to measure resting muscle tone using electromyography to determine the true effect of the two METs on individual muscles. Nevertheless, the main concerns of patients with neck pain are pain, function/disability, and range of motion, and the current study demonstrated no significant differences between the two MET interventions in terms of those outcomes. The lack of a control group in the study may impact internal validity, as other therapeutic modalities may have contributed to the observed treatment effects beyond the MET interventions. However, previous studies have already shown that METs are superior to conventional static stretching when administered with electrotherapy, heating, and joint mobilization in terms of pain, function, range of motion, and isometric muscle strength among individuals with mechanical neck pain [10, 12]. Moreover, in order to improve the internal validity of the study, the use of more objective measurement tools such as pain pressure threshold (algometry) could have been employed to assess pain. It is important to note that the external validity of the current study’s findings is limited to individuals with mechanical neck pain, as the etiology of neck pain can vary depending on the specific subtype. Hence, the results of this study should be applied with caution when considering other types of neck pain.
Conclusion
The current study’s findings indicate that muscle specific and movement specific METs are both effective for reducing pain and disability, as well as improving range of motion in individuals with mechanical neck pain. However, the study did not detect any statistically significant differences between the two techniques in terms of managing mechanical neck pain.
The current study only looked at the immediate and short-term effects of muscle specific and movement specific METs in the management of mechanical neck pain and future studies with long term follow ups should be conducted. Objective measurements such as pain pressure threshold and EMG should be carried out in future studies.
Disclaimer
This manuscript represents a component of a broader investigation on METs in neck pain registered under Ref# FF/FUMC/217-Phy/16, which received approval from the Foundation University Islamabad Ethical Review Committee. Ethical approval specific to the present study was also obtained from the Brainstorm Research Ethical Review Committee (Ref# BR/ERC/2017/1). The study was registered with clinicaltrials.gov (Ref# NCT05063890). A segment of the outcomes of this study was presented at the “18th International Forum for Back and Neck Pain Research in Primary Care”, held at the University of Groningen, The Netherlands, from August 31st to September 1st, 2023. The manuscript underwent a language and grammatical check utilizing AI tools, including ChatGPT and Grammarly.
Informed consent
Consent was taken from all patients participating in the study.
Funding
The current study was funded by Brainstorm Research (brainstormresearch.org) – Internal Funding Grant (Ref# BR/funding/2017/1).
Author contributions
Muhammad Osama was responsible for the conception of the idea, study design, data collection, data analysis, and drafting the manuscript.
Footnotes
Acknowledgments
None to declare.
Conflict of interest
The author was a member of the Brainstorm Research Ethical Review Committee, but was not involved in the ethical review of the current study.