Abstract
BACKGROUND:
Persistent symptoms in patients with systemic joint laxity (SJL) are often equivalent with complications. Screening for SJL is an important part of the assessment of musculoskeletal phenotype. The common measuring tool, the Beighton score (BS), still has unclear evidence.
OBJECTIVE:
To assess the Beighton score in a clinical context for (1) ability to classify SJL as absent or present (criterion validity), and (2) interrater reliability (physician-physiotherapist), for a dichotomous cut-off (yes/no), as well as for interpretation in categories (no, some, clear SJL).
METHODS:
This real-world observational study included 149 consecutive patients seeking secondary care for investigation of possible myalgic encephalomyelitis/chronic fatigue syndrome. Assessment was done during a routine examination. Data were evaluated with Cohen’s kappa and Spearman’s rho.
RESULTS:
BS criterion validity showed poor agreement with the assessment of SJL: percentage agreement was 74 % and kappa 0.39 (3-cut level), 73 % and kappa 0.39/0.45 (4-/5-cut level). The best interrater reliability was moderate (rho 0.66) for interpretation in categories.
CONCLUSIONS:
The BS alone was not a reliable proxy for SJL and should be supplemented with a targeted history. Nevertheless, its interrater reliability was acceptable, and the categorised score appears to have greater clinical relevance than the dichotomous score.
Keywords
Background
Musculoskeletal conditions are the main cause (17%) worldwide behind ‘years lived with disability’, according to the World Health Organization [1]. These conditions limit mobility and capacity, leading to early retirement, lowered quality of life and constrained societal participation [1].
Systemic joint laxity because of overly elastic connective tissue, here defined as a range of motion beyond normal limits in multiple joints [2], is common, being present in 20–30% of the population [3] and with women in majority [4]. When this is accompanied by persistent symptoms, it is termed hypermobility spectrum disorder [2], or the hypermobility type of Ehlers-Danlos syndrome [5] (definition-wise, the latter encompasses a more pronounced over-elasticity in soft tissue), with a prevalence of around 0.2% [6]. Patients who have a hypermobility spectrum disorder risk to develop persistent grave discomfort, including the condition chronic fatigue syndrome (CFS), also referred to as myalgic encephalomyelitis (ME) [7]. ME/CFS is a complex and debilitating disorder that account for a large portion of the primary care work load [8]. ME/CFS is similar to conditions such as fibromyalgia and whiplash-associated disorder (WAD) [9, 10], in that it is a ‘central sensitivity syndrome’ [9, 11]. Post-exertional malaise (PEM) is considered to be distinguishing for ME/CFS [12]. This has been more acknowledged in recent years [7, 13], and stricter standards are needed for accurate clinical assessment of systemic joint laxity in the initial health care contact [14]. Perhaps the most common instrument today is the Beighton score (BS). Given its prominent place in diagnostics, it must also be dependable at a primary level of care, in a bedside assessment in less experienced hands. A scientific evaluation of the Beighton score’s factual classification capacity would result in better-defined study populations in research, and would pave the way in the clinic for adequate interventions and a suitable regimen when the musculoskeletal durability to load was challenged.
The outcome of the BS has traditionally been dichotomised to reflect its role in the clinic. Either a 4- or a 5-cut level is usually considered a positive test outcome indicating systemic joint laxity [15]. To acknowledge the patient’s past joint mobility status (and not just their current status), the Five-part Questionnaire (5PQ) [16] is considered to be a psychometrically sound method. Both the BS and the 5PQ are widely used and have the prerequisites to contribute to the investigation [15]. The latest systematic review on the BS measurement properties [17] concluded that it is a highly reliable tool, but that the reproducibility between assessors from different professional fields has not yet been studied. A systematic review from 2017 deemed its criterion validity not sufficiently researched, especially regarding modes of interpretation [15]. Since systemic joint laxity is a continuum [18, 19], an interpretation of the degree of such laxity may be expected to serve patient management better than a dichotomous one. To the best of our knowledge, only one previous study [19] examined the stability of an interpretation in categories, and no previous study used an entirely clinical setting for this large group of patients. Our hypothesis was that the BS would also live up to earlier acceptable results for interrater reliability in this clinical setting. We further hypothesised that there would be a better unity and thereby a better measurement stability in the instrument when hypermobility was handled as a graded phenomenon. Furthermore, we assumed a BS alone would be able to identify or exclude systemic joint laxity to a great extent.
The aims of this study were to evaluate in a clinical context (1) if the BS alone was indicative of the condition systemic joint laxity (criterion validity), with 3-, 4- and 5-cut level (3 points being the minimum indication of the mid category, some systemic joint laxity) [19] for a group with persistent severe fatigue; and (2) interrater reliability in the BS, for dichotomous interpretation (yes/no) and for interpretation in categories (no, some, clear systemic joint laxity).
Methods
The screening was part of a routine clinical investigation with standardised content chosen at the clinic. The present report complies with the quality standards of the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) for cohort studies [20].
The Beighton score measurement tool [23]
The Beighton score measurement tool [23]
This was a prospective diagnostic observational study conducted at the privately managed, publicly funded clinic in Stockholm, Sweden. The clinic is a specialist clinic for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and thus investigates patients with severe persistent fatigue throughout Sweden. All study participants were referred to the clinic for ME/CFS investigations. At the time, recommendations for referring physicians were posted in the digital support hub for primary healthcare professionals, as follows: If medical specialist care necessary, if rehabilitation with a team-based approach necessary, or in cases of diagnostic doubts after the initial management within the primary healthcare system. All adults (
Inclusion criteria: 1) Patients with severe fatigue affecting physical and/or mental functioning for a minimum of 6 months and who were admitted for investigation at Bragée Clinics. Exclusion criteria: 1) Any acute or chronic condition that would limit study participation, and 2) being unable to communicate in English or Swedish.
The required sample size was estimated to be a little less than 100 patients, based on recommendations by Shoukri et al. [21] with the parameters a required statistical power of 80%, a minimum accepted agreement of kappa 0.4 and an expected agreement of kappa 0.7, and with the prevalence of systemic joint laxity among patients attending the clinic estimated to be about 0.55, as for fibromyalgia [22]. However, the current study was part of a larger project with 275 participants, so the same group (
The first screening for hypermobility consisted of the BS, and the second screening of a semi-structured history, the 5PQ, and the BS. Here, a semi-structured history meant gathering information about musculoskeletal health (current and past), possible instability of the ankles and sometimes such matters as were brought to attention in an extended discussion with the patient around the 5PQ, such as their experiences of physical activity and exercise. No education or training for assessors took place prior to the data collection. Screening 1 was done by one of four specialist physicians (family medicine, anaesthesiology, neurology, psychiatry) and screening 2 by a specialist physiotherapist (sports medicine). Both the physicians and the physiotherapist had many years of clinical experience. The physiotherapist had no knowledge of the outcome of screening 1.
The electronic health records (Take Care) of all study participants were reviewed. For those who had had a screening, data were extracted from the responsible physician’s/physiotherapist’s documentation and were grouped in an Excel file, in the following main categories: quantitative outcome of first screening; quantitative outcome of second screening; and integrated assessment regarding systemic joint laxity according to assessor 2 (present/not present). Age and sex were also documented, as was the timespan between the first and second screening. In cases where notes in the patient’s file were lacking, so that interpretation was not possible, notes were filed as missing data. In cases where the assessor had registered a point interval instead of a valid score (e.g. 2–4), the mean was used (3 in the example).
Test positions included in the Beighton score. © Susanne Staubli University Children’s Hospital Zurich, published with permission.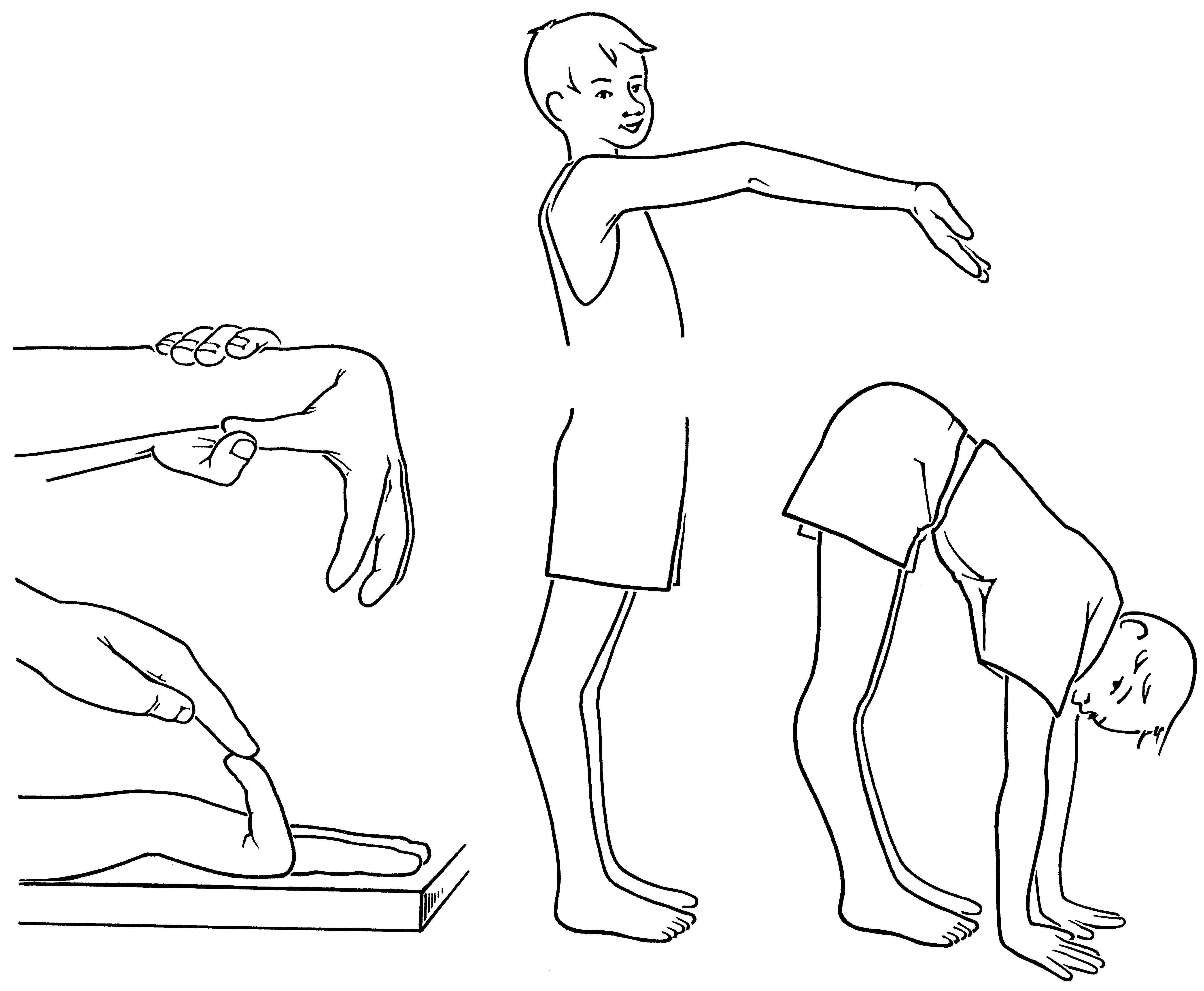
Recommended qualitative judgements of correlation coefficients