
Abstract
Background:
Generalized joint hypermobility (GJH) has been identified as a risk factor for injury in various athletic patient populations.
Purpose:
To evaluate GJH as a predisposing risk factor for injury in a population of National Collegiate Athletic Association (NCAA) Division I football players.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
The Beighton score was collected for 73 athletes during their preseason physical examinations in 2019. GJH was defined as a Beighton score ≥4. Athlete descriptive characteristics, including age, height, weight, and playing position, were recorded. The cohort was evaluated prospectively for 2 years, and the number of musculoskeletal issues, injuries, treatment episodes, days unavailable, and surgical procedures for each athlete during this period were recorded. These measures were compared between the GJH and no-GJH groups.
Results:
The mean Beighton score was 1.4 ± 1.5 for the 73 players; 7 players (9.6%) had a Beighton score indicating GJH. During the 2-year evaluation, there were 438 musculoskeletal issues, including 289 injuries. The mean number of treatment episodes per athlete was 77 ± 71 (range, 0-340), and the mean number of days unavailable was 67 ± 92 days (range, 0-432 days). There were 23 athletes who required 25 operations, the most common procedure being arthroscopic shoulder stabilization (n = 6). The number of injuries per athlete was not significantly different between the GJH and no-GJH groups (3.0 ± 2.1 vs 4.1 ± 3.0; P = .13), nor were there any between-group differences in the number of treatments received (74.6 ± 81.9 vs 77.2 ± 71.5; P = .47), days unavailable (79.6 ± 124.5 vs 65.3 ± 89.3; P = .61), or rates of surgery (43% vs 30%; P = .67).
Conclusion:
A preseason diagnosis of GJH did not place NCAA football players at a greater risk for injury during the 2-year study period. Based on the findings of this study, no specific preparticipation risk counseling or intervention is warranted for football players who are diagnosed with GJH as defined by the Beighton score.
Joint laxity in a healthy patient population was first described in 1964 by Carter and Wilkinson. 4 Three years later, Kirk et al 13 introduced generalized joint hyperlaxity (GJH) and described its relationship with articular pain. In 1973, the Beighton score was identified as an appealing method of diagnosing GJH because it utilized 5 basic clinical tests and had a simple 9-point scoring system. 1,8,27 These early studies suggested that GJH predisposed patients to recurrent dislocation, early arthritis, effusions, ligamentous injury, and premature osteoarthritis. 7
More recently, the anterior cruciate ligament (ACL) literature has brought attention to GJH, which is now a well-recognized risk factor for poor outcomes after ACL reconstruction and has been implicated as a potential risk factor for ACL injury. 12,17,19,23,32,34 The use of a simple clinical screening test for injury, such as the Beighton score, is appealing because it would allow physicians and trainers to identify at-risk athletes and initiate injury prevention measures. Therefore, researchers have taken a specific interest in better defining how GJH is associated with injury in sport. Currently, the relationship of the Beighton score with injury in an athletic patient population is not well defined, and GJH rates are known to vary widely between different sports. 2,5,6,14,21,29 –31,33
The goal of this study was to evaluate GJH as a predisposing risk factor for injury in a population of National Collegiate Athletic Association (NCAA) Division I football players. We hypothesized that athletes with GJH would have a higher rate of injury when compared with athletes without GJH.
Methods
Participants
This study was approved by the institutional review board of our university health system as well as the research review committee of the athletic department. Written consent was obtained from each athlete. Football players who were registered with the athletic department and completed their preseason physical examinations were included in the study. We excluded athletes with a preexisting injury preventing their ability to complete the examination and athletes with missing data in the injury capture system. A power analysis confirmed that the number of available players on the football roster was sufficient to detect differences in the number of injuries, musculoskeletal (MSK) issues, treatment episodes, and days unavailable between the 2 cohorts.
Data Collection
Beighton scores were measured during the players’ preseason sports physical examinations in April 2019. A goniometer was utilized to ensure accurate measurements, and no additional information was collected at the time of examination to limit examiner bias. Measurements were made as described by Beighton et al 1 and included small-finger hyperextension beyond 90°, wrist flexion and thumb abduction to touch the thumb to the volar forearm, elbow hyperextension beyond 90°, knee hyperextension beyond 90°, and forward bending to place bilateral palms on the floor while keeping the knees fully extended. The bilateral measurements were each assigned 1 point for each side. GJH was defined as a Beighton score ≥4. Each athlete’s descriptive characteristics were recorded from the university’s electronic medical record system and included age, position, height, and weight.
After 2 years, in April 2021, each athlete’s chart was reassessed for MSK issues, injuries, athletic trainer treatments, and days unavailable from practice or game play. Playing time was identified as a likely confounding variable, so the football team’s publicly available statistics were also reviewed to identify the number of games in which each athlete appeared.
Statistical Analysis
MSK-related data within the 2-year period were grouped by body location and were compared between the GJH and no-GJH groups. Categorical data were compared with the chi-square test, and continuous variables were compared using the Student t test. A subgroup analysis was performed to identify differences between athletes who underwent surgery and those who did not have surgery. A second subgroup analysis looked at the mean Beighton score, GJH, and outcomes by player position. Pearson correlation analyses were performed to assess the relationship between the number of games played and number of injuries, as well as the relationship between mean Beighton score and mean athlete body mass index (BMI) according to player position. All data and statistical analyses were performed using SPSS software (Version 23; IBM Corp). An alpha level of .05 was set for all comparisons.
Results
The Beighton score was collected for 78 football players. There were 3 athletes with active injuries precluding examination (an Achilles tendon tear, lower extremity fracture, and back strain), and there were 2 athletes with incomplete training room and injury logs; these players were excluded. (Figure 1). The mean Beighton score for the 73 included football players was 1.4 ± 1.5. The most frequent Beighton score among the athletes was 0 (36%), followed by a score of 1 (23%). There were 7 athletes (9.6%) with a Beighton score ≥4, indicating GJH (Figure 2).

Flowchart of available athletes, excluded athletes, and those eligible for the study.
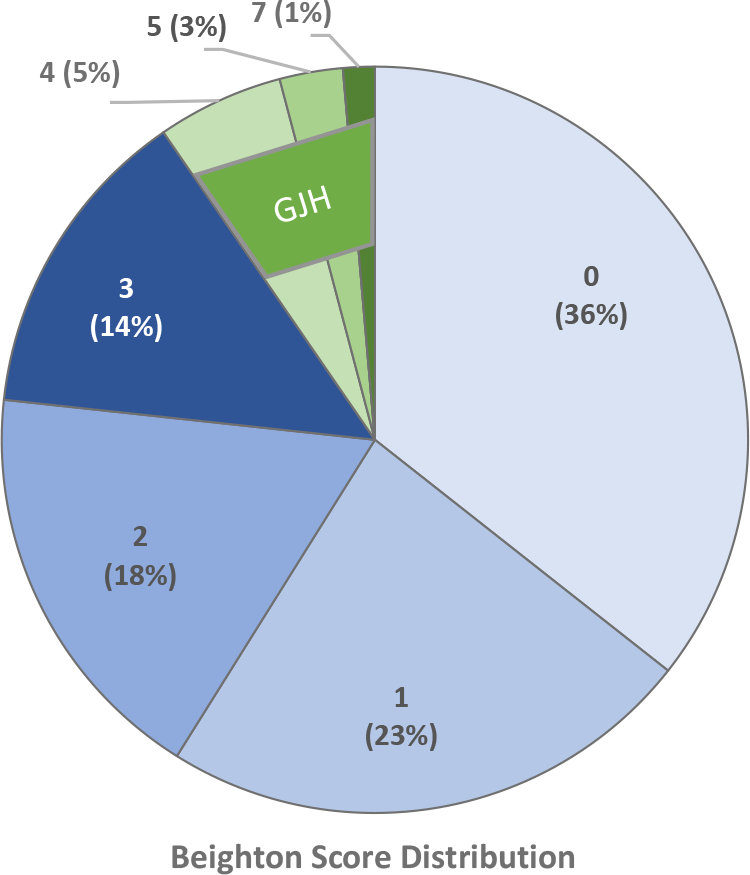
Distribution of Beighton scores and generalized joint hypermobility (GJH) among the study cohort (N = 73).
During the 2-year study period, the athletes played a mean of 1.7 ± 0.46 seasons and appeared in a mean of 11.1 ± 7.0 games. There were 22 athletes (30%) who graduated or transferred before the second season. There were 438 MSK issues that initiated an evaluation by an athletic trainer, physical therapist, or physician; 289 were classified as injuries. The most common anatomic regions affected were the shoulder (n = 54), thigh (n = 48), and hand (n = 39) (Figure 3). The mean number of treatments received was 77 ± 71 (range, 0-340), and the mean number of days unavailable was 67 ± 92 days (range, 0-432 days). There were 23 athletes who underwent 25 operations during the 2-year study period. The most common operations were arthroscopic shoulder stabilization (n = 6), arthroscopic partial meniscectomy (n = 3), scapholunate ligament repair (n = 3), and hip arthroscopy for femoroacetabular impingement (n = 2) (Figure 4).

Musculoskeletal (MSK) issues and injuries recorded during the 2-year study period (n = 438).

Surgical procedures performed during the 2-year study period (n = 25). ACL, anterior cruciate ligament; FAI, femoroacetabular impingement; ORIF, open reduction and internal fixation.
Comparison of Athletes With Versus Without GJH
The overall number of MSK issues per athlete during the 2-year study period did not differ significantly between the GJH and no-GJG groups; however, the number of hip-related issues (0.1 ± 0.4 vs 0.5 ± 0.8 per athlete; P = .04) and wrist-related issues (0.0 ± 0.0 vs 0.1 ± 0.2 per athlete; P = .04) were significantly lower in the GJH group (Table 1).
Comparison of MSK Issues by Location Between the GJH and No-GJH Groups a

a Data are reported as mean ± SD. Boldface P values indicate a statistically significant between-group difference (P < .05; 2-sample t test). GJH, generalized joint hypermobility; MSK, musculoskeletal.
The mean number of seasons completed in the GJH group was the same as in the no-GJH group (1.7 ± 0.21 vs 1.7 ± 0.24; P = .93); however, athletes with GJH appeared in significantly fewer games compared with the athletes without GJH (6.1 ± 4.0 vs 11.6 ± 7.0; P = .008). There were no significant differences between the GJH and no-GJH groups in mean number of injuries or mean injuries per game. The numbers of the most common injuries per athlete (ankle sprain, hamstring injury, and shoulder instability) were also independent of GJH, as were the number of injury treatments received, number of days unavailable, and athletes who underwent surgery (Table 2).
Comparison of Injuries, Treatment, and Days Unavailable Between the GJH and No-GJH Groups a

a Data are reported as mean ± SD or % (No. of athletes). GJH, generalized joint hypermobility.
b Fisher exact test used for categorical variables, 2-sample t test for continuous variables.
Results of Subgroup Analyses
In the subgroup analysis, there were no differences in any of the study variables between athletes who underwent surgery (32%) and those who did not (Table 3). In the subgroup analysis by player position, significant differences were found in the Beighton score (P = .007), rate of GJH (P = .011), and BMI (P < .0001) according to player position (Table 4). Quarterbacks demonstrated the highest Beighton score (2.8 ± 1.8) and GJH rate (60%), while defensive linemen demonstrated the lowest Beighton score (0.4 ± 0.7). No lineman, offensive or defensive, demonstrated GJH. Among the 3 most common types of injury, only the hamstring injury rate differed significantly by player position (P = .014). Linebackers had the highest hamstring injury rate (63.6%), while the offensive and defensive linemen had no hamstring injuries (0.0%) (Table 4).
Results of Subgroup Analysis of Athletes Who Underwent Surgery a
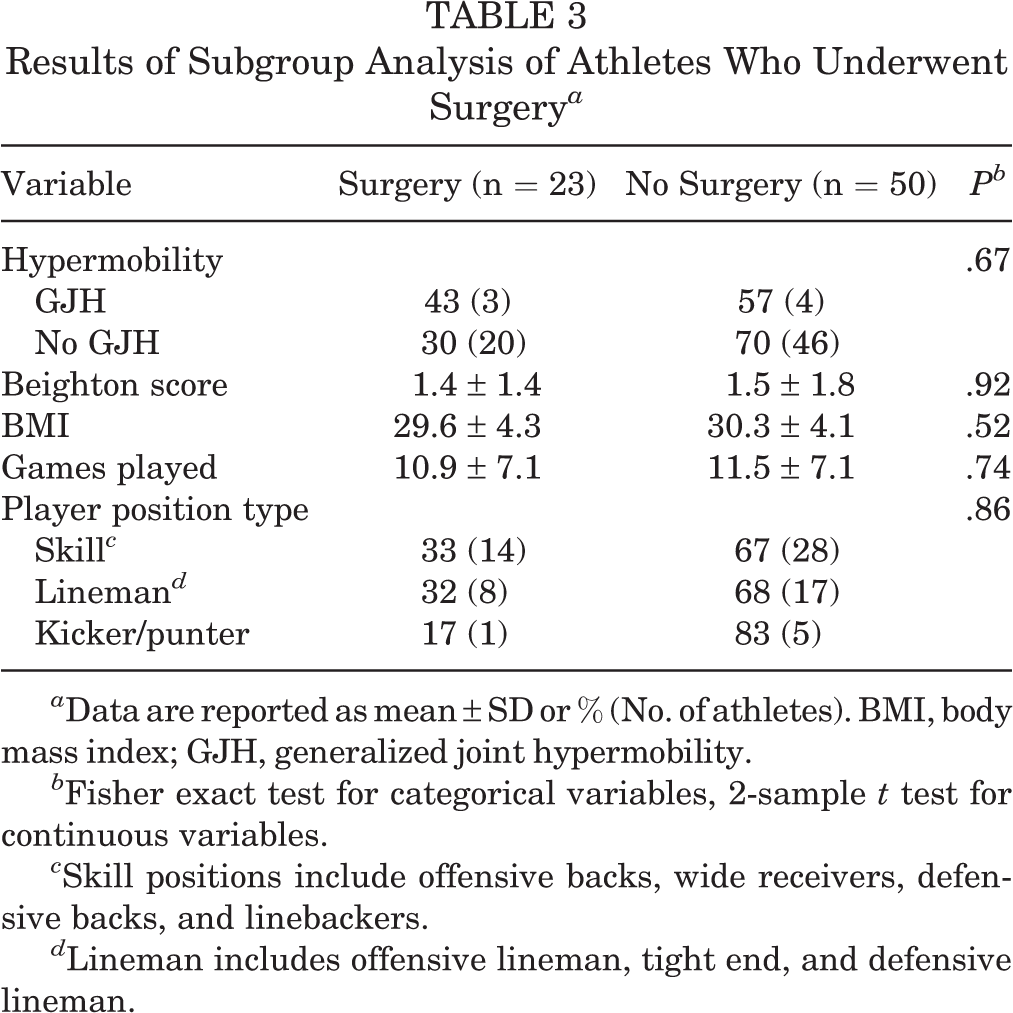
a Data are reported as mean ± SD or % (No. of athletes). BMI, body mass index; GJH, generalized joint hypermobility.
b Fisher exact test for categorical variables, 2-sample t test for continuous variables.
c Skill positions include offensive backs, wide receivers, defensive backs, and linebackers.
d Lineman includes offensive lineman, tight end, and defensive lineman.
Results of Subgroup Analysis of Outcomes by Player Position a

a Boldface P values indicate a statistically significant difference among positions (P < .05; analysis of variance). BMI, body mass index; GJH, generalized joint hypermobility; MSK, musculoskeletal.
Results of Correlation Analysis
In the correlation analysis, the number of MSK injuries was positively correlated with the number of games an athlete played (r = 0.37; P = .0012) (Figure 5), and the Beighton score was inversely correlated with the mean BMI per player position (r = –0.60; P = .086) (Figure 6).

Scatterplot demonstrating the relationship between the number of musculoskeletal injuries and the number of games played.

Scatterplot demonstrating the relationship between the Beighton score and mean body mass index (BMI) according to player position.
Discussion
When compared with the nonhypermobile cohort, the athletes with GJH did not have statistically different rates of MSK issues, injuries, athletic trainer treatments, days unavailable, or surgeries. These results were contrary to our hypothesis. This study demonstrated that a diagnosis of GJH did not place NCAA Division I football players at a greater risk for any negative outcome after 2 years of evaluation. To our knowledge, this is the only football-specific study in the literature evaluating MSK issues and injuries in athletes with GJH.
This is also the first study to demonstrate that Beighton scores vary significantly by position on the football field. Quarterbacks demonstrated the highest laxity with a mean Beighton score of 2.8 and GJH rate of 60%, and defensive lineman had the lowest, with a mean Beighton score of 0.4 and no players with GJH. Overall, when compared with a population of healthy male college students studied by Russek and Errico, 26 our cohort of collegiate football players had a lower prevalence of GJH (27% vs 9.6%).
There was a significant difference in the mean number of games played by the GJH group compared with the nonhypermobile group. The players without GJH appeared in nearly 2 times the number of games versus the players with GJH (11.6 ± 7.0 vs 6.1 ± 4.0; P = .008). Although this difference was significant, the causation of this finding is unknown. It is possible that the lower game appearance rate of the athletes with GJH confounded our injury and outcome analyses, as Rechel et al 24 estimated that 55% of the high school football injuries occur during competitive game play. So, it would be reasonable to deduce that less game play in the GJH group would have led to fewer injuries. However, our data showed that there was also no difference in the number of injuries per game between the GJH and no-GJH groups (P = .61).
Three other studies have attempted to evaluate ligamentous laxity and its role in football injuries. The first evaluation of ligamentous laxity in American football players was completed in 1970 by Nicholas, 20 who clinically evaluated an athlete’s laxity based on a 5-point scale including floor touch, knee recurvatum, knee-ankle rotation, hip rotation, and forearm hypersupination. After following the athletes for ≥1 season, Nicholas reported an increased risk of knee ligamentous injury associated with increased ligamentous laxity. Five years later, Kalenak and Morehouse 11 designed a study to quantitatively grade “loose-jointed” and “tight-jointed” football players at the collegiate and professional levels using a custom apparatus that placed varus and valgus stress through the knee. After following their cohort for 3 seasons, the authors determined that knee ligamentous injuries occurred in equal rates between athletes with “loose” and “tight” knees. Later, in 1996, Krivickas and Feinberg 16 showed that male collegiate athletes with a Beighton score 1 SD above the mean had a 0.34 relative risk for injury, but this finding was not specific to American football.
A few studies have demonstrated a higher risk of injury in athletes with GJH participating in other contact sports, including soccer, rugby, and martial arts. 14,15,21,31,25 Conflicting results have been published in populations of lacrosse and netball players, where GJH was not associated with any increased incidence of MSK injury. 6,30 A 2010 systemic review analyzed the body of literature at that time and concluded that athletes with GJH had a significantly increased incidence of ligamentous knee injury during contact activities. 22 A more recent systematic review in 2018 found evidence associating GJH with lower extremity injury incidence but not with upper extremity injury or injury severity. 33
GJH has implications beyond just increased risk of joint injury in athletes. One study by Hardin et al 9 demonstrated that athletes with GJH had slower rehabilitation times when returning to play after injury. In ACL injuries in particular, GJH has been associated with ACL injury risk and inferior outcomes after ACL reconstruction. 34 Furthermore, patients who underwent revision ACL reconstruction had higher GJH scores on average than patients who underwent primary ACL reconstruction. 34
During the 2-year study period, 25 orthopaedic procedures (12.5 per year) were performed, which was lower than previously published rates. Mehran et al 18 followed an NCAA Division I football team for 10 years and reported 23.4 orthopaedic procedures per year, and the most common procedures were shoulder labral repair, partial meniscectomy, ACL reconstruction, and hip labral repair with femoral and acetabular osteoplasty. Our rate was likely lower for 2 reasons: (1) we followed a cohort of athletes over 2 years and did not include athletes who joined the team during the second year of analysis, and (2) this study was significantly affected by the coronavirus 2019 pandemic. Beighton scores were measured during the 2019 preseason physical examination. The 2019 season was completed in full, and the team competed in 12 regular-season games; however, the pandemic delayed the 2020 season by approximately 2 months, and only 9 regular season games and 2 postseason games were played. This undoubtably had a profound effect on our cohort of athletes and their injury rates. However, the pandemic affected both the GJH and no-GJH groups equally, so the comparison of outcomes between our 2 study groups was valid.
Limitations
There were other limitations to this prospective cohort study. Among the 73 study athletes, 51 (70%) completed both seasons; thus, the mean evaluation period was 1.7 years. The athletes who joined the team in 2020 were not examined and were not included in the cohort. There were also athletes on the roster who did not complete their annual physical examinations on campus during the standard preseason physical examinations; these players were not captured by the study. Two additional players had missing data in the training room log and injury capture system; neither patient demonstrated GJH (Beighton scores of 1 and 2). These missing data were managed by excluding these 2 players from analysis. Each player’s examination was performed by a single examiner; multiple independent examinations may have produced more precise scores. However, previous studies looking at the Beighton score measurement in adults have demonstrated substantial to excellent interexaminer and intraexaminer reliability, so redundant examinations were not required. 3,10,28 This study was underpowered to demonstrate differences among specific injuries or surgical procedures and their relationship to GJH; however, it was designed to be sufficiently powerful in order to identify a difference in number of injuries, MSK issues, treatment episodes, and days unavailable. Additionally, this study evaluated a very specific patient population, and thus the study results are likely not generalizable outside of a population of football players.
Conclusion
A preseason diagnosis of GJH did not place collegiate football players at a greater risk of injury during the 2-year study period. Based on the findings of this study, no specific preparticipation risk counseling or intervention is warranted for football players who are diagnosed with GJH as defined by Beighton score.
Footnotes
Final revision submitted October 12, 2022; accepted November 9, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.A.T. has received speaking fees from Arthrex and Smith & Nephew and hospitality payments from Medwest Associates. V.K.T. has received education payments from Arthrex and consulting fees and speaking fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Northwestern University (reference No. STU00207434).