
Abstract
BACKGROUND:
The first-line contact for patients seeking care for low back pain (LBP) can potentially change the disease course. The beliefs and attitudes of healthcare providers (HCPs) can influence LBP management. Although referring patients with LBP to physical therapy is common, the first-line contact for patients with LBP in Saudi Arabia is the primary care physician (PCP). Physical therapy will soon be integrated into primary care; therefore, it is rational to compare physical therapists’ (PTs) beliefs and attitudes regarding LBP with those of PCPs.
OBJECTIVE:
We compared PCPs’ and PTs’ attitudes and beliefs regarding LBP management.
METHODS:
We employed a cross-sectional, voluntary response sample research design using the Pain Attitudes and Beliefs Scale (PABS). Participants were PTs and PCPs practicing in Saudi Arabia.
RESULTS:
In total, 153 participants completed the PABS (111 PTs and 52 PCPs). PCPs demonstrated significantly higher PABS biomedical subscale scores than did the PTs.
CONCLUSIONS:
HCPs in Saudi Arabia should receive additional training to adopt a biopsychosocial approach to managing LBP. In this study, the HCPs’ treatment recommendations may not correspond with contemporary clinical guidelines. Research to facilitate the implementation of optimal professional education and training to adopt a biopsychosocial approach is an urgent priority.
Keywords
Introduction
Low back pain (LBP) is considered a major musculoskeletal health issue [1] and is one of the most common causes of disability, causing substantial socioeconomic burden worldwide [2]. In Saudi Arabia, LBP is the most commonly reported type of pain, with an overall lifetime prevalence between 63.8% and 89% [3]. Chronic LBP, defined as persistent pain in the lower back for more than three months, was the second most common site of pain after lower extremities in patients with chronic pain (
Although multiple factors can influence the chronicity of LBP, the psychosocial profile of the patient has been reported to be a critical prognostic factor for pain persistence, response to treatment and rehabilitation, and the likelihood of developing disability [5]. Several studies have focused on analyzing the potential link between psychosocial factors, such as catastrophizing, fear avoidance, and the treatment response in patients with chronic LBP, and this topic has been a popular area of research over the past few years [5, 6].
The beliefs and attitudes of healthcare providers (HCPs) can significantly influence their clinical deci-sion-making and the psychosocial status of their patients [7, 8, 9, 10]. All clinical guidelines on LBP are in agreement that HCPs should have a broad psychosocial perspective; however, studies show that the actual beliefs and attitudes of HCPs vary between biomedical or biopsychosocial frameworks [7, 10, 11, 12, 13].
Attitudes and beliefs can influence the extent to which HCPs adhere to the clinical guidelines for managing LBP. For instance, those who focus on biomedical management and have fear-avoidance beliefs themselves have been shown to display suboptimal adherence to LBP guidelines [12]. Further reasons for lack of guideline adherence include a lack of biopsychosocial knowledge, the belief that they are not sufficiently qualified to adapt their practice to a biopsychosocial approach, and patient demands to define pain biomedically; for instance, by imaging [11, 13]. Several measures can be used to assess the attitudes and beliefs of HCPs concerning LBP. Bishop et al. [8] highlighted the Pain Attitudes and Beliefs Scale (PABS) as a reliable and feasible measure to evaluate the attitudes and beliefs of HCPs regarding LBP management.
There is ample evidence supporting the early management of LBP in primary care practice and the use of nonpharmacologic treatments while discouraging medication and imaging for LBP [14, 15, 16, 17]. In Saudi Arabia, physical therapy services are not available in primary care centers yet and are offered only at secondary level centers based on specialist referrals [18].
However, there is an agreement among patients and stakeholders that physical therapy services are best suited to the primary care setting [19, 20] and physical therapy will soon be integrated into the primary care setting. Moreover, various studies from different countries have demonstrated successful implementation of physical therapy at the first point of contact for patients with musculoskeletal conditions [21, 22, 23]. The biopsychosocial and biomedical orientations toward LBP appeared to be low among physiotherapists according to a recent study [24]. A stronger orientation toward biopsychosocial beliefs and attitudes regarding LBP management was associated with a better selection of guideline-based physiotherapy interventions [24]. Multiple publications have indicated a profound biomedical orientation and low adherence to LBP guidelines among PCPs internationally [12, 25, 26]. However, there are no studies exploring the beliefs and attitudes of PCPs regarding LBP in Saudi Arabia.
We hypothesized that PCPs in Saudi Arabia might demonstrate a higher biomedical orientation than PTs; however, both may demonstrate low biopsychosocial orientation. Similarly, we hypothesized that a negative association may be found between the two orientations – biomedical and biopsychosocial – in general, regardless of the study sample. Hence, we aimed to compare the beliefs and attitudes of PCPs and PTs in Saudi Arabia regarding LBP management.
Methods
We used a cross-sectional, voluntary response sample design to examine the attitudes and beliefs of PCPs and PTs regarding LBP management in Saudi Arabia. This study was approved by the Institutional Review Board of the Ministry of Health (IRB# 2019-0060 E). Each participant provided a signed informed consent form prior to participation. We targeted PCPs and PTs in Saudi Arabia whose clinical practice frequently involved treating patients with LBP, and this was an introductory question in the invitation that was sent to them.
Primary care physician sampling
An invitation for PCPs to participate in the study was sent via email to all 400 primary care centers in the Riyadh region, in which, there are 288 currently practicing PCPs. Notably, rural primary care centers service patients two to three days a week.
Riyadh region’s primary care centers account for 20% of all primary centers in Saudi Arabia [27]. Additionally, the capital city of Riyadh encompasses more than 22% of the country’s medical facilities that include more than five tertiary care centers in which patients seek care from around the country [27].
Physiotherapist sampling
As physiotherapy services are not available in primary care centers, PTs were recruited via a web-based survey that was distributed through various social media channels and email.
Self-administered survey
Once the respondents agreed to participate, they were able to access an online survey using a link provided in the email. This survey comprised two sections: the first section collected demographic data, including age (categorical variable), sex, and years of experience, and the second section used the PABS to assess the respondents’ treatment orientation (biomedical or biopsychosocial) toward LBP. The PABS is a 19-item self-administered questionnaire that examines the strength of the two treatment orientations toward LBP: biomedical (10 items) and behavioral (9 items) [8]. Each item is rated on a 6-point Likert scale (“totally disagree”
The test re-test reliability of the PABS was good, with intraclass correlation coefficients for the biomedical scale ranging from 0.73 to 0.81, and 0.65 to 0.82 for the biopsychosocial scale [28]. Additionally. construct validity was confirmed to a two-factor structure using exploratory factor analysis [28, 29]
Data analysis
The analyses were performed using the Statistical Package for the Social Sciences (SPSS, Version 25). The level of significance was set at
Results
The invitation link was visited by 72 PCPs, suggesting a response rate of 58%. Nonetheless, because we used multiple recruitments platforms to invite PTs, the response rate might be difficult to estimate. In total, 153 participants (111 PTs and 42 PCPs) completed the survey. The demographic data of the PTs and PCPs are shown in Table 1. The PT sample was similar to the PCP sample with respect to sex. However, the PCP group was older in age and had more clinical experience than the PT group [
Personal and professional characteristics of physical therapists and primary care physicians
Personal and professional characteristics of physical therapists and primary care physicians
PCP: primary care physician, PT: physical therapist.
The means and SDs of the PABS for PTs and PCPs are presented in Table 2. PCPs had significantly higher PABS biomedical subscale scores (Mdn
Pain Attitudes and Beliefs Scale descriptive statistics
Pain Attitudes and Beliefs Scale descriptive statistics
PCP: primary care physician, PT: physical therapist, SD: standard deviation, PABS: pain Attitudes and Beliefs Scale.
The relationship between the two Pain Attitudes and Beliefs subscale scores in the physical therapy sample.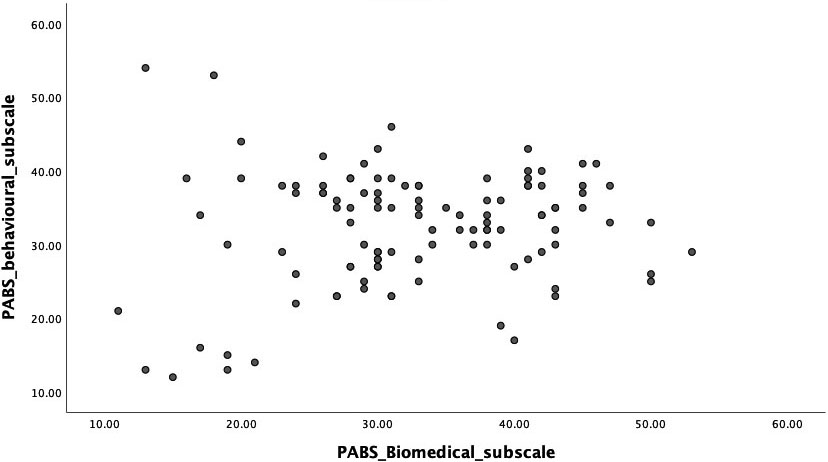
The correlation between the two PABS subscale scores was not significant (
A comparison between the two samples for each of the 19 PABS items is shown in Supplementary Figures S1 to S19.
The relationship between the two Pain Attitudes and Beliefs subscale scores in the primary care physician sample.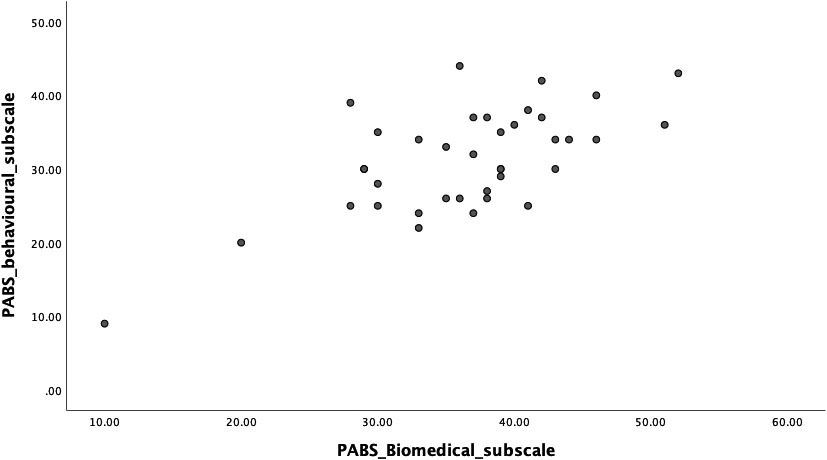
In this study, the PABS was used to compare the attitudes and beliefs of PTs and PCPs in Saudi Arabia regarding LBP management. We found that the total scores on the biomedical and behavioral subscales among the PTs were remarkably close (32.7
Additionally, the results showed that the biomedical score was significantly higher among PCPs than PTs. PTs appear to hold a stronger opinion than PCPs regarding the point that patients with severe back pain would benefit from physical exercise. This is comparable to the findings of a previous study involving Dutch PTs [30]. In contrast, PCPs appear to hold the opinion that patients with back pain should preferably practice only pain-free movements. This corresponds to previous studies, which state that a stronger biomedical orientation among HCPs is associated with higher overall disagreement with the reported recommendations to return to usual activity or work [7, 28, 32]. These reported beliefs among PCPs might reflect fear and are contradictory to the recent recommendations for LBP management that encourage providing clear information on continuation of activities, even if there is some pain [33, 34].
Evidence has shown that HCPs who embrace more biomedical than behavioral beliefs regarding the underlying cause and mechanism of LBP may perceive daily activities as more harmful [7, 10]. Consequently, they are more likely to recommend that their patients limit their daily activity levels and avoid returning to work [9, 10]. This may lead to the patient developing unhelpful beliefs, avoiding activities perceived to be damaging, restricting social participation, and contributing to greater levels of disability [12, 24, 25, 26, 35]. Our results are consistent with the findings of a study in the United Kingdom, which reported that 28% of HCPs would recommend patients with LBP to remain off work, and this advice was significantly related to a higher biomedical score in the PABS [36]. However, further research is required to examine the association between advice based on such beliefs and development of subsequent beliefs and behaviors in Saudi individuals with LBP.
Clinical implications
Overall, the findings of this study suggest that more training should be given to HCPs in Saudi Arabia to adopt a biopsychosocial approach to manage LBP. This is important because LBP is a multifactorial health condition that can be influenced by various biological and psychosocial risk factors [5, 37, 31, 38]. Similarly, disability related to LBP is known to be influenced by factors from different domains, including individual (e.g., age) and psychological (e.g., psychological distress and pain-related fear) factors, in the Saudi population [33, 34]. In addition, there is robust evidence suggesting that the attitudes and beliefs of patients regarding LBP are influenced by the attitudes and beliefs of HCPs [7, 8, 9, 10] as well as other factors, including painful past experiences [39, 40].
Limitations
The study results should be considered within some limitations. First, we sought to reach a representative sample of both PCPs and PTs; however, the number of samples collected in this study may limit the generalizability of the findings. Therefore, further research may be needed. Second, the beliefs and attitudes of HCPs in this study were measured using a self-reported survey, which raises the possibility that the results may reflect an individual propensity to select the behavioral approach. Third, selection bias might have occurred because the study included a higher number of PTs than PCPs, limiting the ability to explore differences between the two research groups. Moreover, all the PCPs and most PTs were from Riyadh which also might have introduced selection bias. Nonetheless, Riyadh is the capital city of Saudi Arabia and is composed of diverse HCPs coming from different regions and backgrounds. Finally, the study was conducted as a convenience sample, which may need further evaluation with a probability population to generalize outcomes to a broader population.
Conclusions
Our results showed ambiguous orientation among PTs, and stronger biomedical orientation among PCPs than PTs. Beliefs regarding treatment recommendations among the participants did not correspond to the clinical guidelines for LBP management. This may negatively influence the attitudes and beliefs of patients and might contribute to unfavorable outcomes in individuals with LBP. This uncertainty and stronger biomedical orientation among participants may have a negative influence on patients’ attitudes and beliefs, thus contributing to the burden related to LBP.
Footnotes
Acknowledgments
This project was supported by the Deanship of Scientific Research at Prince Sattam Bin Abdulaziz University under the research project No: 2019/01/13195. The authors are immensely grateful to the participants of this study.
Conflict of interest
None to report.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-200295.