
Abstract
BACKGROUND:
Up to now there is not enough evidence that supports the use of electrotherapy in the treatment of Bell’s palsy.
OBJECTIVE:
Through a systematic review, we aimed to verify whether the use of electrotherapy is effective for treating Bell’s palsy or peripheral paralysis.
METHODS:
Publications were searched in PubMed, EBSCO and Web of Science. The present systematic review included studies that analyzed the electrotherapy as a therapeutic method for treating individuals with Bell’s palsy, in order to recover the function of facial muscles.
RESULTS:
Seven studies involving a total of 131 cases and 113 controls were included in this systematic review. In the studies analyzed, patients received electrotherapy combined with other treatments such as hot-wet facial napkins, massages and muscle reeducation. Although the effect of electrotherapy alone was not evaluated, the use of electrotherapy combined with other treatments produced a significant improvement in the individuals evaluated.
CONCLUSIONS:
Due to the diverse methodologies used and the small number of individuals included in the studies, we could not fully prove the efficacy of electrotherapy for treating Bell’s Palsy. Future studies with larger samples and homogenous populations should be performed to obtain conclusive results.
Introduction
Facial peripheral paralysis, or Bell’s palsy, is an acute mononeuropathy of the facial nerve. It is of unknown cause and can affect a single nerve; it starts with pain in the mastoids region and partial or total paralysis of one side of the face [1, 2]. Bell’s palsy affects equally males and females, with an incidence of 11.5 to 40.2/100 000 [3, 4]. The incidence is higher in individuals with Diabetes Mellitus, immunocompromised patients, individuals with arterial hypertension, patients who have had a viral infection of the upper respiratory tract, and pregnant woman [5]. Although Bell’s palsy can happen at any age, there are peaks of incidence between 15–45 years of age, mean age 40 years [6]. Bell’s palsy is usually idiopathic (75% of cases), and less frequently a secondary paralysis (25%) [2]. Several etiologic mechanisms have been proposed to explain the development of Bell’s palsy including herpes virus, infectious mechanisms, ischemic mechanisms and autoimmune mechanisms; nevertheless, these are not completely understood [7, 8, 9].
The treatment of Bell’s palsy is divided into acute and maintenance treatments. The acute treatment consists of using corticosteroids and antivirals that must be initiated within the first 72 hours after the onset of clinical signs [8]. The use of corticosteroids represents a highly-recommended intervention with evidence of improvement [3, 10]. Regarding the use of antivirals, it is recommended that antiviral drugs are not prescribed in isolation [3, 11]. The maintenance treatment includes interventions such as eye care, mouth care, physical therapy, Botulinum toxin injections and even complementary medicine treatments such as acupuncture [8].
Another type of treatment is physical therapy. However, according to the general-international Guidelines and some systematic reviews, physical therapy is not a highly recommended treatment due to the scarce evidence of improvement observed in individuals with Bell’s palsy who received any type of physical therapy [3, 12, 13, 14]. Nonetheless, in a recent systematic review, it was reported that the combination of pharmacological treatment with some modalities of physical therapy, favored a better recovery than pharmacological treatment alone [15]. Therefore, our systematic review will determine if the use of electrotherapy is recommendable when treating individuals with Bell’s palsy. The objective of this systematic review is to demonstrate the benefits and efficacy of electrotherapy for treating patients with facial paralysis (Bell’s palsy), in comparison to patients who did not receive electric stimulation.
Quality assessment of the studies using the GRADE system
Quality assessment of the studies using the GRADE system
This systematic review followed the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) criteria. The protocol of this systematic review was registered in PROSPERO (
Inclusion and exclusion criteria
Inclusion criteria
The studies had to be published in peer-reviewed journals; had to be written in English; had to be cross-sectional or case-control designs. The studies had to provide information regarding time of exposure and the effects of the electrotherapy when treating patients with Bell’s facial paralysis. Finally, the electrical stimulation had to be performed with electrodes.
Exclusion criteria
Controlled clinical trials that did not include electrotherapy as part of the Bell’s facial paralysis treatment. Protocol articles for future studies were also excluded [16].
Search and selection of articles
We performed a search in PUBMED and Web of Science databases. We used the terms “Bell’s palsy”, “electrical stimulation”, “rehabilitation” and combinations such as “Bell’s palsy and electrical stimulation” and “Rehabilitation and facial paralysis”. The search was concluded in January 2017. Initially, the electronic search generated 1,148 potentiality relevant papers; of those, we excluded 517 because they were duplicates. Then, we excluded 580 more, as they were of no relevance for this systematic review, or were written in other language than English, or were systematic reviews. Additionally, 27 papers were excluded after reading the abstract. Finally, we considered 24 papers; however, after reading and analyzing the contents, only 7 papers were included in this systematic review (Fig. 1).
Flowchart showing the search strategy used in the systematic review.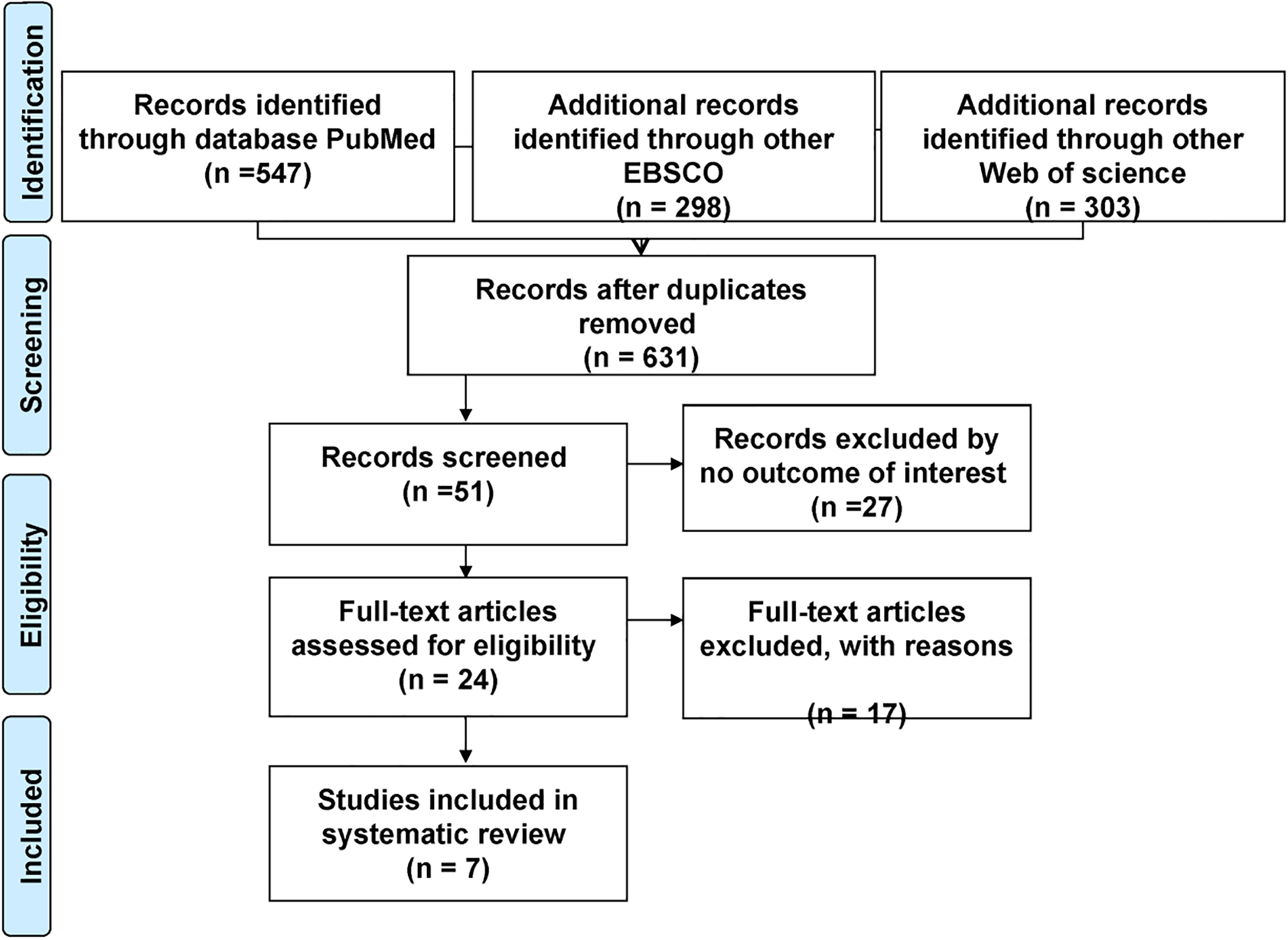
Data was extracted by two independent investigators (EGBP and MSM). Each reviewer extracted the following data: author, year of publication, location, number of controls, number of cases, diagnoses and evolution of the palsy, characteristics of the treatment in the clinical trials and also additional treatments.
Data analysis
The selected studies were assessed using the GRADE system (Grading of Recommendations Assessment, Development and Evaluation Scale) (
Results
This systematic review analyzed seven studies related to facial paralysis or Bell’s palsy and rehabilitative treatment. The descriptive characteristics of each study are shown in Table 2.
Brief description of each study included
The study by Targan et al. in the USA [17] included twelve individuals with idiopathic facial paralysis and five individuals with a history of surgically affected nerves were recruited [17]. Diagnoses were based on latency and the House-Brackmann scale. They obtained the correlation coefficients between clinical residuals and nerve conduction latency (
Another study performed in India included 59 individuals diagnosed with Bell’s palsy [18]. Patients were divided into a control group (
In a recent study performed in the region of South Africa [19], 16 individuals were recruited and divided into a re-education group (
In a different study [20], individuals with Bell’s palsy were divided into a group that received electro stimulation (
Finally, in a study performed by Kim et al. in Korea [21], 60 individuals with Bell’s palsy in early phase were selected and separated into two groups, control (
Descriptive and clinical characteristics of the studies
Descriptive and clinical characteristics of the studies
In a study conducted in Finland by Hyvärinen et al., ten individuals with chronic facial paralysis were enrolled [22]. When electrical stimulation was applied in the facial nerve, patients showed improvement, and the distal latency obtained improved (
Discussion
This study was conducted in order to determine if the use of electrotherapy is helpful in the treatment of Bell’s palsy. The results of this systematic review showed that there is an improvement in patients who received electrotherapy, in both phases, acute and chronic. Although there is not enough evidence regarding the effectiveness of electrotherapy for treating Bell’s palsy [24], the results found in this systematic review are oriented towards a positive response to the treatment.
In the present study, we analyzed 131 cases and 113 controls. We included seven publications, while both of the previous systematic reviews only included three or four publications. For instance, the review about physical therapy for treating Bell’s palsy performed by Teixeira et al. [25], analyzed 3 trials and reported no significant improvement in patients who received electrical stimulation, questioning its cost-effectiveness. In the update of the same review [14], four trials were analyzed and the results obtained were similar. It is necessary to emphasize that these previous reviews did not aim to specifically evaluate electrotherapy, but multiple physical therapies. In addition, the trials analyzed were not very recent.
On the other hand, there are several countries without an up to date guide for the long term treatment of Bell’s palsy [26]. Although it has been stated that receiving electrotherapy in the acute phase of Bell’s palsy is beneficial for patients [19, 20, 21, 27], and it is highly used in the Mexican clinical practice (for diagnosis and management of Bell’s palsy), there is not enough evidence to support the efficacy of electrotherapy in acute cases.
It is necessary to mention that although patients who received electrical stimulation improved their condition in all the studies evaluated, the methodology used in each one was different. For instance, in the study by Tuncay et al. [20], the electro stimulation with a current wave phase began four weeks after diagnosis. The results showed differences in facial re-education according to the House-Brackmann scale. Furthermore, Hyvärinen [22] used 20 Hz electro stimulation and 100
Unlike previous studies, Manikandan [18] used electrostimulation via galvanic and faradic current for facial muscles stimulation. Although patients showed improvement, we must emphasize that electro stimulation therapy was combined with facial rehabilitation exercises, through which much of this improvement was obtained. In more recent studies [19, 20, 21], the results of electrical stimulation treatment in the early phase of Bell’s Palsy demonstrated a significant recovery. It is important to mention that this improvement was observed in studies with a considerable
Given the importance of the treatment in Bell’s palsy, our findings suggest that the use of electrotherapy may play an important role in the improvement of patients. It would be necessary to develop further studies with similar characteristics such as parameters of frequency, intensity, pulse duration, treatment time, number of sessions, number of contractions and even the same area of stimulation, with the purpose of clarifying the genuine role that electrotherapy plays in Bell’s palsy treatment.
Footnotes
Conflict of interest
The authors have no competing interests to report.
Appendix: PRISMA checklist
Section/topic
#
Checklist item
Reported
on page #
Title
Title
1
Identify the report as a systematic review, meta-analysis, or both.
Title page
Abstract
Structured summary
2
Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number.
Abstract
Introduction
Rationale
3
Describe the rationale for the review in the context of what is already known.
3
Objectives
4
Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS).
4
Methods
Protocol and registration
5
Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number.
NA
Eligibility criteria
6
Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale.
4–5
Information sources
7
Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched.
4–5
Search
8
Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated.
4–6
Study selection
9
State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis).
5–6
Data collection process
10
Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators.
5–6
Data items
11
List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made.
4
Risk of bias in individual studies
12
Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis.
4–6
Summary measures
13
State the principal summary measures (e.g., risk ratio, difference in means).
NA
Synthesis of results
14
Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I
5–6
Risk of bias across studies
15
Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies).
Additional analyses
16
Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified.
6,
Results
Study selection
17
Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram.
6
Study characteristics
18
For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations.
6–9,
Risk of bias within studies
19
Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12).
Results of individual studies
20
For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot.
6–8
Synthesis of results
21
Present results of each meta-analysis done, including confidence intervals and measures of consistency.
NA
Risk of bias across studies
22
Present results of any assessment of risk of bias across studies (see Item 15).
Additional analysis
23
Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression (see Item 16)).
NA
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi: 10.1371/journal.pmed1000097.
Section/topic
#
Checklist item
Reported
on page #
Discussion
Summary of evidence
24
Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers).
9–11
Limitations
25
Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias).
9–11
Conclusions
26
Provide a general interpretation of the results in the context of other evidence, and implications for future research.
9–11
Funding
Funding
27
Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review.
12