
Abstract
BACKGROUND:
The human sacroiliac joint (SIJ) in vivo is exposed to compressive and shearing stress environment, given the joint lines are almost parallel to the direction of gravity. The SIJ supports efficient bipedal walking. Unexpected or unphysiological, repeated impacts are believed to cause joint misalignment and result in SIJ pain. In the anterior compartment of the SIJ being synovial, the articular surface presents fine irregularities, potentially restricting the motion of the joints.
OBJECTIVE:
To clarify how the SIJ articular surface affects the resistance of the motion under physiological loading.
METHODS:
SIJ surface models were created based on computed tomography data of three patients and subsequently 3D printed. Shear resistance was measured in four directions and three combined positions using a customized setup. In addition, repositionability of SIJs was investigated by unloading a shear force.
RESULTS:
Shear resistance of the SIJ was the highest in the inferior direction. It changed depending on the direction of the shear and the alignment position of the articular surface.
CONCLUSION:
SIJ articular surface morphology is likely designed to accommodate upright bipedal walking. Joint misalignment may in consequence increase the risk of subluxation.
Introduction
The sacroiliac joint (SIJ) is located in the posterior pelvis. It comprises synovial joints in the anterior region and tough ligaments (syndesmosis) in the posterior region (Fig. 1) [1], connecting the sacrum and the ilium. Due to the strong ligaments connecting the joint partners, the SIJ has comparably low mobility. The range of motion is generally considered to be limited to a few millimeters and degrees [2–4]. The representative movements of SIJ, called nutation and counter-nutation, mainly include forward and backward rotations of sacrum on the sagittal plane, respectively. The sacrum is deeply driven into the pelvic ring fixed by the pubic symphyses anteriorly, and the posterior pelvic ligaments, considering this state as being the most stable form for the SIJ [5]. SIJs are assumed to serve primarily as a damper, redirecting impact between the upper and lower part of the body, thereby transmitting it effectively [6]. Unexpected or unphysiological impact is believed to cause pain at the SIJ [7]. SIJ dysfunction has been hypothesized to be caused by SIJ ligament laxity resulting in joint misalignment. Therefore, fixation of the SIJs to prevent excessive motion is considered an effective therapy to relieve SIJ pain.
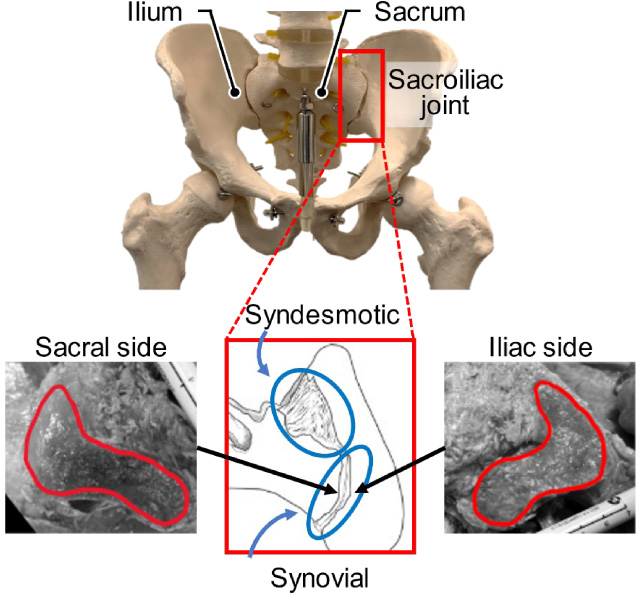
The anterior and posterior sides are synovial joints and ligamentous regions, respectively. The edges of synovial joint area are shown in red lines.
The synovial joint area comprises the auricular surfaces of both the ilium and the sacrum. Fetuses have unfused sacral vertebrae and SIJs surfaces are not formed until Carnegie stage [8]. After birth, the five separated sacral vertebrae start to coalesce and it completes by the age of 25 to 30 [9,10]. SIJ surfaces probably remain relatively flat until puberty [11], however, they are covered with fine irregular elevations and depressions [12]. In general, the auricular surface on the sacral side is concave, whereas the auricular surface on the iliac side is convex [5,12,13]. In detail, however, the upper and lower parts of sacral surface are concave and convex, respectively [5,14]. In addition, the major axis slopes from antero-superior-lateral to posterior-inferior-medial and is twisted caudally [5]. Furthermore, the proportion of immobile joints increases with age [15]. Solonen [16] stated that articular surfaces are formed by mechanical loading during growth and upright stance. The fetal human pelvis and SIJ closely resemble in the structures of quadrupeds [16]. The stimulation of completely upright bipedal walking, unique to humans, may involve in the formation of a distinct SIJ surface morphology, which in other joints may be considered pathological [17]. Movements of the SIJ are considered to take place around a lateral axis at the level of the second sacral vertebra [18]. Toyohara et al. [6] could demonstrate that the center of rotation changes throughout the walking cycle, suggesting that the SIJ is exposed to a complex dynamic environment. Contemporary research explains the SIJ motion being limited by the joint partners, ligaments [19–21] and muscles [22]. Previously, motion resistance by the morphology of SIJ surfaces were, however, investigated only by the group Vleeming et al. [23], who measured the static coefficient of the SIJ surface. The mobility of SIJs to date has not been well characterized in relation to its surface morphology. Since the articular surfaces of SIJs is aligned almost vertical to the line gravity, loading from the trunk results in significant shear force exerted to the SIJ [24]. Thus, the joint surface morphology may help prevent the SIJ from excessive sliding and affect joint motion. This given study aims to clarify how the SIJ surface affects resistance of the joint motion. It was hypothesized that the shape of the joint surface potentially restricts the direction and range of motions in the SIJ.
Pelvic surface model with sacroiliac joints
Computed tomography data of the lumbar spine and pelvis of three patients were provided by the JCHO Sendai Hospital (Sendai, Japan) for this study. Two of them suffered from unilateral SIJ dysfunction, the contralateral unaffected sides were used for modeling. All patients provided the written informed consent for use of their data. The whole pelves were automatically segmented to construct a pelvic surface model. The articular (cartilaginous) surfaces of the sacrum and ilium were manually segmented with 1-mm slices. The SIJs were cut in the sagittal planes at intervals of 30 mm centered on the articular surfaces (Fig. 2). The cases of right SIJ models were reversed and all SIJ models were assumed to be on the left sides. The SIJ articular surface models were placed on a base (100 mm wide, 100 mm long, 2 mm depth). All surface models were 3D printed in ABS resin using a 3D printer (da Vinci 1.0 Pro 3D Printer, XYZ printing Inc., Tokyo, Japan). The printed models were exposed to acetone in vapor form for one hour to obtain smooth model surfaces. After drying sufficiently, casts were made with silicon and the articular surface models were duplicated with polyester resin.
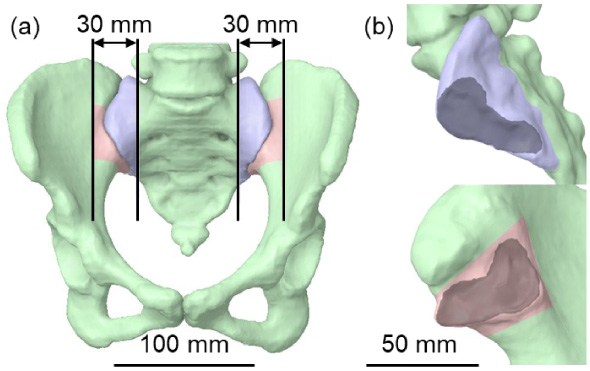
(a) Surface models on a pelvis. The blue and red models were models representing the sacroiliac joint parts of the sacrum and ilium, respectively. The black lines were the cutting lines with intervals of 30 mm. (b) Surface models of a sacrum (blue, top) and ilium (red, bottom). The dark areas indicate surface regions.
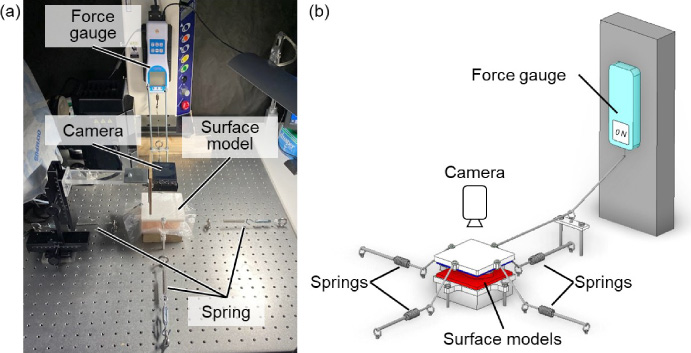
A joint motion resistance test device. (a) Experimental setup. (b) Schematic configuration.
A customized testing device (Fig. 3) was developed for this study. The tests were designed to mimic the stress environment to reflect both compressive and shear stresses to the SIJ. It comprised of a force gauge (DTG-100N, Digitech Co., Ltd., Osaka, Japan), a digital camera (DSC-WX500, Sony Corp., Tokyo, Japan), springs and the 3D-printed SIJ surface models. The force gauge pulled the models to apply and measure shear force. The springs caused the surface models to compress and pull them back to their initial position. The camera tracked the displacement of the models. In addition, vinyl was placed between the models to prevent the resin models from sticking to each other. A shear resistance coefficient is given by the following formula.
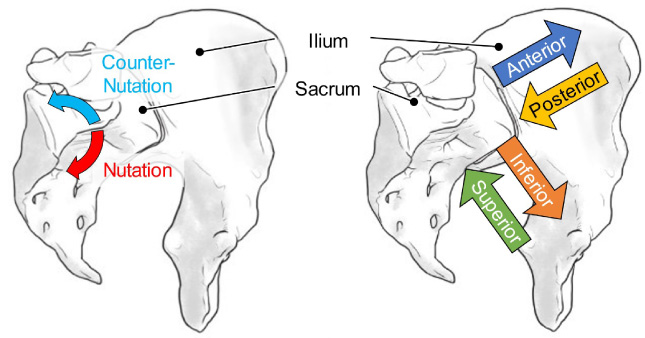
Experimental conditions on (left) alignments and (right) directions.
The force gauge pulled the models at a velocity of 60 mm/min in four given directions, the vertical and anteroposterior direction of the articular surfaces (Fig. 4) and was set to stop at a maximum of 20 N. The sacrum and ilium cartilage surface models were used as the moving and fixed sides, respectively. The force gauge recorded force history, the camera tracked the displacement of the sacrum models. In addition, to investigate the difference in resistance due to the joint surface alignment, the ilium model was rotated by ±5 degrees to represent the extremes of the nutation and counter-nutation positions, respectively. All tests were performed three times for each condition.
Joint repositioning test
The force gauge pulled the models to in the four directions outlined in Fig. 4. The pulling forces ranged between 2 and 20 N in 2-N increments with a displacement of 60 mm/min, and then returned to 0 N. After each experiment, the device was returned to its original position before the next set of experiments was conducted. Likewise, the sacrum and ilium models were used as the moving and fixed sides, respectively. The camera captured the displacements of the sacrum models when the force gauge returned. In addition, to investigate the difference in repositioning capacities due to the combination of joint surfaces, the ilium model was rotated by ±5 degrees to reproduce the nutation and counter-nutation positions. All tests were performed one time for each condition.
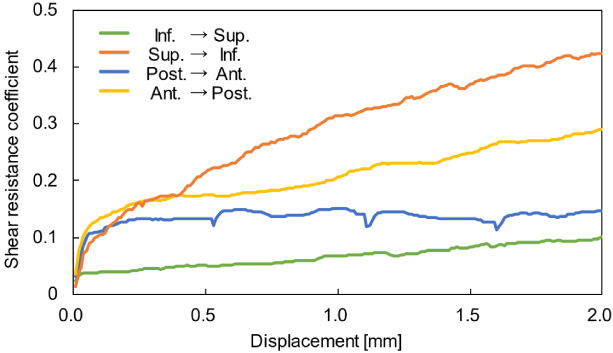
A representative shear coefficient on the in vivo condition. Ant.: anterior, Inf.: inferior, Post.: posterior, Sup.: superior.
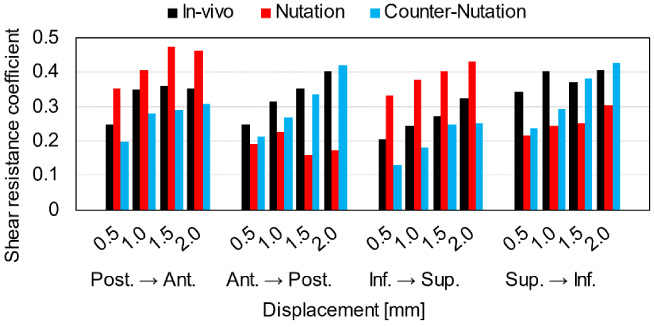
Shear coefficients at four displacement points from initial positions (a) on the in vivo conditions and (b) on all conditions. Ant.: anterior, Inf.: inferior, Post.: posterior, Sup.: superior.
Joint motion resistance
The compression forces averaged 31 N. In the anterior direction (blue line), the change in friction coefficient was less than 7% at any displacement position (Fig. 5). The friction coefficients in the anterior superior direction (green line) were 0.1. The friction coefficients varied, depending on the pulling direction. The descending order of friction coefficients in the in vivo condition was as follows: superior to inferior (orange line), anterior to posterior (yellow line), posterior to anterior (blue line), inferior to superior (green line) (Fig. 5). The friction coefficient further changed, depending on the joint surface alignment. Furthermore, the friction coefficient increased in the anterior (left bars) and superior (center right bars) directions at the nutation position, hardly changed in the anterior (left bars), posterior (center left bars) and superior (center right bars) directions at the counter-nutation position and decreased on the others (Fig. 6).
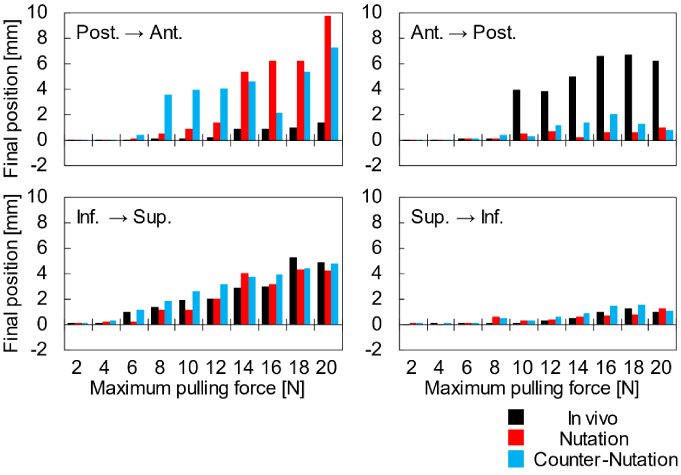
Repositioning on the posterior to anterior (top left), anterior to posterior (top right), inferior to superior (bottom left) and superior to inferior (bottom right) directions. The horizontal axes are maximum pulling force in increments of 2N. The vertical axes are final position returned 0 N on parallel to pulling directions. Ant.: anterior, Inf.: inferior, Post.: posterior, Sup.: superior.
The compression forces averaged 31 N. Figure 7 shows that the surface models did not return to their original positions following an unloading with a load exceeding threshold. The load which caused displacement from the initial positions of more than 2 mm was 10 N (to posterior) and 12 N (to superior) on the in vivo condition, 12 N (to superior) and 14 N (to anterior) on the nutation condition and 8 N (to anterior) and 10 N (to superior) on the counter-nutation condition.
Discussion
To date, very few studies exist on the relationship between SIJ surface morphology and joint resistance. The only study on the topic was conducted by Vleeming and coworkers more than three decades ago [23]. They reported that SIJs had a much higher friction coefficient than knee joints [23] in spite of the diarthrotic (synovial) nature both joints present. Further to this, SIJ with ridges and depressions presented a higher coefficient of friction than those without, as presented by static friction coefficients derived from 11 SIJ auricular surface facets measuring 4 mm squares each [23]. Differences in frictional resistance on whole morphology of the synovial joint regions and in directions of movements, however, have not yet been investigated to the authors’ best knowledge. The given study for the first time investigated the motion resistance depending on alignment of the joint surfaces and the directions of the sliding motion.
The five sacral vertebrae consistently present fuse to form the sacrum by osseointegration in adult [25]. The upper and lower parts of the SIJ surfaces continue presenting the morphological features of the original sacral vertebrae, whilst the central portion is formed by bony fusion. Wolff’s law [26] states that bones adapt to loads by the formation of bones. Whole-body motion during growth may, therefore, contribute to the ultimate SIJ morphology [16], suggesting that SIJ surface morphology is optimized for human movement in an upright posture. A study investigating subchondral bone strength following SIJ arthrodesis showed that mineralization in the sacrum significantly increased 6 months after surgery [27], indicating that the articular surface is affected by changes in mechanical stimulation. Since humans need to support the trunk load at the SIJ during standing, the downward motion of the sacrum needs to be strongly restricted so to be energetically optimized. On the other hand, the upward motion of the sacrum seems non-beneficial for the potential energy loss on efficient swing phase during walking. It is reasonable for bipedal walking that the friction coefficients were high during downward motion and consistently low during upward motion.
The ridges and depressions on the SIJ articular surfaces help contribute to high friction coefficients [23], however, the whole articular morphology may be designed to accommodate upright bipedal walking. In addition, this study suggested that this motion of lifting while bending forward had a low coefficient of friction in SIJs and a large load may be applied to ligaments and muscles. The counter-nutation position has been considered to be the most stabilized state [5], which was not in agreement with the findings of this study. Although there are individual differences, it is necessary to investigate not only the SIJ surface friction resistance but also the pelvic structure including ligaments and muscles for further research on the subject.
SIJ disease can be regarded a joint dysfunction due to minor subluxation of the joints [24], which is a minute but existent misalignment of the joint surfaces one relative to the other. Since conservative treatments such as manual therapy [5,28] aid reducing pain by resolving joint incompatibility [5], the combined position of the joint surfaces may affect the function of SIJs. The repositioning tests demonstrated that nonconformity of the joint partners as a result of the unevenness of the surfaces, thus making it less possible to return to its original configuration even if a large load is applied. Articular surface morphology may be optimized for human motion, however, can adversely affect the joint environment. The range of SIJ motion has been reported to be less than 1 mm [3,6,29–35], which is considered to be the physiological range. In this study, the displacement of 2 mm or more – twice the physiological range after the unloading of shear force – was regarded pathological, i.e., fulfilled the criteria for subluxation of the SIJ. Table 1 shows the results of a preliminary study with a finite element model of a pelvis [6] (analytical condition: 70 kg body weight, double leg standing). In this experimental study, a compressive force of 31 N was applied, which corresponds to shear forces of 5.6 N (backward) and 16.3 N (downward). Permanent displacement occurred as a consequence of relatively small loads in the anteroposterior directions. Subluxation is, however, facilitated to occur in the upward direction. This direction does not receive large loads in vivo and it may be necessary to pay closer attention to impacts such as an acceleration phase when jumping. Due to articular surface morphology, the models were displaced in directions other than the shear direction. Depending on the direction of the loading, large displacements occurred, which may pose a higher risk of subluxation. The alignment position of the joint changes the load that can cause subluxation. Especially in the forward load, the nutation and counter-nutation were greatly displaced even with small loads, suggesting that there was an increased possibility that a sudden backward fall may result in excessive movement potentially resulting in SIJ dysfunction.
Summary of preliminary study for shear and compressive forces on the sacroiliac joint with a finite element model of a pelvis [6]
Summary of preliminary study for shear and compressive forces on the sacroiliac joint with a finite element model of a pelvis [6]
The model based on CT data of a healthy male imported into ANSYS 2021R1 (Cybernet Systems Co., Ltd., Tokyo, Japan) and simulated a double-leg stance with 600 N and 300 N loads applied from the base of the sacrum in the inferior direction and from both femora in the superior direction, respectively. For the other boundary conditions, see the previous paper [6].
There were a number limitations exist for this experimental study. First, the bony surfaces of the ilium and sacrum forming the anterior (diarthrotic) SIJs in vivo are covered with cartilage. Cartilage thickness varies between 2–3 mm on the sacral side and 1 mm on the iliac side [8,17,36]. In consequence, the joint surfaces are softer than bones and should be deformed to larger by friction than bone. This study, however, used a resin model and thus could not consider the deformation behavior of cartilage. In addition, the extent of cartilage mineralization varies between joints [37,38], which may affect sliding motion. Next, the surface models were created based on X-ray CT data and printed out using a 3D printer with a pitch of 0.2 mm. This study therefore cannot reflect the surface geometry with submillimeter accuracy. The surface morphology of the whole joint, however, was reproduced, which was sufficient to investigate relation between the complicated curved surface of SIJs and joint motion resistance. Thirdly, ligament orientations were not considered, although they vary from place to place [25], and may affect joint motion. Finally, the sample size in this study was limited to three. The surface morphology of SIJs varies greatly among individuals [5,14]. For further research, more patient data are needed.
A testing device was developed for joint motion resistance tests and the articular shear resistance of the sacroiliac joint surfaces experimentally investigated. It was suggested that the shear resistance of SIJ changed depending on the shear direction and the alignment position of the surfaces. The SIJ surface morphology may be designed to accommodate an upright bipedal walking and joint misalignment could increase the risk of subluxation.