
Abstract
BACKGROUND:
Over the past two decades, patient-centered care has become internationally recognized as a dimension of high-quality health care. Recent research has shown that patient-centered care has many benefits, which are broadly categorized as patient experience and clinical and operational benefits.
OBJECTIVE:
The study aimed at analyzing the correlation between the application of patient-centered care (PCC) and length of stay, patient satisfaction, and clinical outcome of post-surgical breast cancer patients.
METHODS:
The study design was cross-sectional. A sample of 100 patients was determined and selected with the inclusion criteria. Data were collected using measuring tools comprising patient-centered care and patient satisfaction questionnaires as well as medical records to evaluate the length of stay and clinical outcomes. Bivariate analysis was conducted to analyze the correlation between patient-centered-care and length of stay (LOS), patient satisfaction, and the clinical outcomes of inpatients.
RESULTS:
A correlation was found between patient-centered care (PCC) application and patient satisfaction (p = 0.005), but no correlation was observed between PCC application and length of stay (LOS) (p = 0.176) as well as clinical outcome (p = 0.128).
CONCLUSIONS:
The application of patient-centered care can be attributed to patient satisfaction but is not correlated to length of stay and clinical outcome of post-surgical breast cancer patients. The hospital should create an accepted definition and commonly agreed set of dimensions used for the concept of operationalization and its measurement to implement PCC and improve overall patient satisfaction and clinical outcome and reduce the length of stay as expected.
Keywords
Introduction
The qualities of care and patient safety have long been a topic of interest and have become global issues in healthcare services, particularly in Indonesia. Numerous reports presented strong evidence of widespread quality deficiencies and highlighted a need for substantial change to ensure high-quality care for all patients. Hospitals in Indonesia are required to obtain accreditation periodically at least once every three years as part of efforts to improve the quality of care [1]. The quality of care is high on the agenda due to a paradigm shift in healthcare provision, that is, public demand for high-quality service is increasing due to the advances in technology, knowledge, and access to information. Healthcare organizations have not adequately improved the mechanisms for delivering care despite the aforementioned advancements; in many cases, the delivery of care has remained unchanged over the past several decades [2].
The Institute of Medicine (IOM) identified patient-centered care (PCC) as one of the six objectives for improving healthcare quality in the 21st century; thus, many healthcare organizations have embraced the notion of PCC as central to their strategic mission and values [3,4]. The concept of PCC originates from a holistic paradigm, which suggests that people must be observed in their bio-psychosocial entity, and draws medical attention to the personal identities of patients [5,6]. However, a globally accepted definition of PCC is still lacking despite many proposed definitions to explain this concept. Compared with the traditional biomedical perspective, the main component of PCC focuses on the comprehensive perspective on the patient’s situation, the patient’s understanding and experience of his/her situation, and his/her participation in the decision-making [7]. In a report by the IOM, PCC is defined as health care that establishes a partnership among practitioners, patients, and their families (when appropriate) to ensure that decisions respect the wants, needs, and preferences of patients and education and support necessary to make decisions and participate in their care are provided. In the same report, PCC is mentioned as one of the six fundamental goals of the healthcare system in the United States [3]. In an effort to operationalize PCC from the perspective of the patient, the Picker Institute conducted extensive research and found that patients generally define PCC in eight dimensions. The dimensions comprise the following: (a) respect for the values, preferences, and needs of the patient; (b) coordination and integration; (c) information, communication, and education; (d) physical comfort; (e) emotional support and reduction of fear and anxiety; (f) involvement of family and friends; (g) transition and continuity of care; (h) access to care [8].
Recent research has shown that PCC has many benefits, which are broadly categorized as patient experience and clinical and operational benefits. Stone (cited in Charmel and Frampton 2008) found that the benefits of implementing PCC in inpatient units showed a short average LOS, remarkably low cost of care per case, and an increased patient satisfaction score. Charmel and Frampton (2008) also reported that PCC provides financial benefits in terms of increasing staff retention, decreasing readmission, and reducing the LOS [2,7,9–16]. Hasanuddin University Hospital is a class B teaching hospital owned by Hasanuddin University located in Makassar. Medical records from the Hasanuddin University Hospital revealed several cases of LOS that extend beyond the established standard, especially post-surgical breast cancer patients. LOS is defined as the interval between admission and discharge of inpatients and is one indicator of the quality of inpatient services set by the Indonesian Ministry of Health with an average standard of 6–9 days [17]. The extension of the patient’s LOS can cause various losses, especially to the hospital. The study aims to analyze the correlation between the application of PCC and length of stay, patient satisfaction, and clinical outcome of post-surgical breast cancer patients.
Methods
This study was conducted at Hasanuddin University Hospital from August 2022 to September 2022. The study was a quantitative analysis with a cross-sectional design approach. This study was designed to analyze the correlation between the independent variable (PCC application) and three dependent variables (LOS, patient satisfaction, and clinical outcome). The Ethical Committee of the Faculty of Public Health, Hasanuddin University Makassar, Indonesia, approved this study (number: 10987/UN4.14.1/TP.01.02/2022). The population in this study included post-surgical breast cancer patients who were hospitalized at Hasanuddin University Hospital for three days minimum. The total sample was 100 patients. The inclusion criteria were as follows: (a) patients aged >18 years, (b) suffered from breast cancer, and (c) underwent mastectomy surgery. The exclusion criteria were patients with multiple comorbidities, including diabetes mellitus, coronary artery disease, stroke, other cancers, pulmonary diseases, and kidney failure.
Data collection
Data were collected using measuring instruments in the form of a PCC application questionnaire, patient satisfaction questionnaire, and patient’s medical record to review the LOS and clinical outcome of inpatients. Clinical data and baseline variables were collected from the medical records of patients. The following information was extracted: sex, age, marital status, ethnicity, occupation, income, payment method, education, inpatient room, comorbidities, and LOS.
Statistical analysis
Statistical analyzes were conducted using SPSS software version 26 (IBM Corp., Armonk, NY, USA). Univariate analysis was performed to describe the frequency of the PCC application and its dimensions. Bivariate analysis of the Chi-square test was performed to examine the correlation between the application of PCC and LOS, patient satisfaction and clinical outcome of post-surgical breast cancer patients. If the P-value of the test was <0.05, then the results were statistically significant.
Results
Characteristics
Table 1 presents the characteristics of respondents of 100 post-surgical breast cancer patients. The samples were all female, and their mean age was 50 years old. The majority of the samples were married, and approximately 50% of these samples were Bugis ethnicity. A total of 42% samples were unemployed and have an annual household income IDR < 1.000.000. A total of 100% of samples used national insurance as their payment method. Most of the patient’s last education was in high school. A total of 60% of the patients stayed in the class 3 inpatient room.
Characteristics of participants
Characteristics of participants
Table 2 presents the frequency of variables, including the application of PCC, LOS, patient satisfaction, and clinical outcome. The application of PCC is the patient’s perception of care while receiving treatment at Hasanuddin University Hospital, covering the following eight dimensions: respect for the patient’s values, preferences, and needs; coordination and integration; information, communication, and education; physical comfort; emotional support and reduction of fear and anxiety; involvement of family and friends; transition and continuity of care and; access to care, as measured by the PCC application questionnaire. LOS is the number of days between admission and discharge from the hospital based on data in the patient’s medical record. Patient satisfaction is a feeling of satisfaction or dissatisfaction from patients that arises after comparing patient expectations of service quality after treatment at the Inpatient Unit in Hasanuddin University Hospital considering the dimensions of interpersonal behavior, technical quality, access/convenience, financial aspect, and physical environment as measured by the patient satisfaction questionnaire. As an indicator of the service quality, clinical outcome is the result of interventions from a health service provided to patients. The clinical outcome assessment in this study focused on the surgical site infection, which was evaluated during the patient’s stay up to three days post-mastectomy surgery before being discharged from the hospital using data from the patient’s medical record.
Frequency of variables
Table 2 shows that the application of PCC was considered good according to 56% of respondents. The frequency of the dimensions of PCC application in Fig. 1 reveals that the dimension of respect for the patient’s values, preferences, and needs was the highest according to respondents (83%) while that of access to care showed the lowest percentage (55%). A LOS of <6 days was achieved in 91% of respondents. A total of 51% of respondents agreed that they were satisfied with the care and only 4% of respondents did not achieve the clinical outcome. A total of 4% of respondents had organ/space infections based on the diagnosis criteria of surgical site infections.
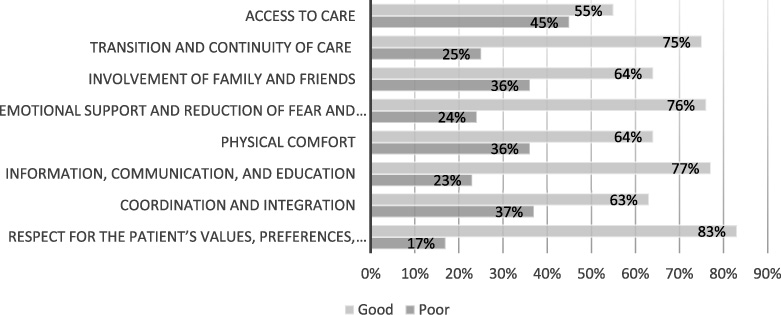
Frequencies of dimensions of PCC application.
Table 3 shows the correlation between PCC application and LOS. The output showed that p-value = 0.176 > 0.05. Therefore, no significant correlation was observed between the application of PCC and LOS in post-surgical breast cancer patients at Hasanuddin University Hospital. Clinically, the application of good PCC achieved LOS up to 94.6% (53 respondents) compared with that of poor PCC, which is 86.3% (38 respondents), despite the absence of correlation between the application of PCC and LOS (p = 0.176) based on the statistical analysis result.
Correlation between PCC application and LOS
Note: Chi-square test.
Table 4 shows the correlation between PCC application and patient satisfaction. The variables were tested using the Chi-square test. The output showed that p-value = 0.005 < 0.05. Therefore, a significant relationship was observed between PCC application and patient satisfaction in post-surgical breast cancer patients at Hasanuddin University Hospital. A total of 64.3% (36 respondents) were satisfied with the care in good PCC applications, while only 34.0% (15 respondents) were satisfied in poor PCC applications.
Correlation between PCC application and patient satisfaction
Note: Chi-square test.
Table 5 shows the correlation between PCC application and clinical outcome. The output showed that the p-value = 0.128 > 0.05. Therefore, no significant relationship was observed between the application of PCC and clinical outcomes in post-surgical breast cancer patients at Hasanuddin University Hospital. Statistically, no correlation was found between PCC application and clinical outcomes (p = 0.128) because the percentage of clinical outcomes achieved was only slightly different between those with good and poor PCC application.
Correlation between PCC application and clinical outcome
Note: Chi-square test.
Application of PCC
The application of PCC was considered good with a percentage of 56% according to respondents (Table 2). The highest percentage among all dimensions of PCC was that considering the values, preferences, and needs of the patient (83%) (Fig. 1). The Picker Institute distinguishes three attributes to this dimension as follows. (1) Illness and medical treatment affect the quality of life of patients; therefore, care should be respectfully provided in the individual atmosphere of a patient. (2) Treating the patient with dignity, respect, and sensitivity to his/her cultural values while (3) keeping the patient informed and involved in the shared decision-making process regarding care process [18]. According to Docteur and Coulter (2012), the dimension of “respect for the patient’s values, preferences, and needs” is the most basic in PCC application; PCC is defined as a healthcare system where patients in each encounter with a given healthcare system are treated as unique persons with their individual needs, values, and preferences [19]. The high achievement of this dimension cannot be separated from the implementation of patient-centered accreditation standards, especially considering the rights of patients and families. According to respondents, patients and families are always involved in the decision-making process related to their treatment plan either by conducting general or informed consent by explaining all the purposes and benefits of procedures, complications, and side effects in a language that can be understood by patients and their families [20].
The results of the cross-tabulation between respondent characteristics and PCC application revealed that the application of PCC was considered good the highest in the group of respondents with bachelor degrees, and quite low in the group of respondents who did not attend school. This finding indicates that patients will understand and focus on the service process obtained when the education level is high. Moreover, the results of the cross-tabulation obtained information that the implementation of PCC was mostly considered good for patients treated in class 3 inpatient room, which proves that patients felt that they are not treated differently from those treated in superior inpatient classes. By contrast, the dimension with the lowest percentage is access to care (55%) (Fig. 1). According to the Picker Institute (2013), this dimension encompasses the following attributes: (1) access to the location of hospitals, clinics, and physician offices; (2) availability of transportation; (3) ease of scheduling appointments; (4) availability of appointments when needed; (5) accessibility to specialists or specialty services when a referral is made; and (6) clear instructions provided on when and how to get referrals [18]. Another available literature demonstrates a diversity of characteristics attributed to the domain of access to care, which can be divided into two categories, namely tangible and non-tangible. The tangible category includes all attributes that relate to physical access to care, such as access to specialists (availability of healthcare professionals) and the health center (geographically, availability of transportation, availability for patients with mobility issues). The non-tangible category refers to the timeliness, cultural (cultural differences), educational (support and navigation for illiterate patients; clear instructions provided on how and when to obtain a referral) and language directions (e.g., clear direction in several languages) [21]. Most of the patients in this study complained regarding access to care related to access to location and specialist appointments. Hasanuddin University is a class B hospital located in Makassar and has several centers of excellence, including a cancer center. Most of the respondents from this study are referred from another hospital, decreasing its accessibility for all the respondents. Some respondents even came from another city. In addition, respondents complained about the appointments with specialist doctors. They only occasionally meet with the residents and must wait for a long time to see a specialist. Regarding referral issues, most respondents agreed that information regarding when and how to obtain referrals was clear and always informed by nurses.
Correlation between PCC application and LOS
The target for achieving LOS in this study is ≤6 days, which refers to the clinical pathway in post-surgical breast cancer patients at Hasanuddin University Hospital, especially those undergoing mastectomy surgery. Most of the patients who underwent mastectomy in this study were discharged on the third day after surgery with an average LOS of 5 days. The target LOS of this patient is in accordance with the average length of stay after breast cancer surgery in several previous studies. Data from 22 European countries showed a substantial decrease in the average LOS for breast cancer patients between 1990 and 2005, where the average LOS for breast surgery decreased from 9.8 days in 1990 to 5.2 days in 2005. Especially for those undergoing a mastectomy, the median LOS decreased from 6 to 5 days [22]. In addition, a study in Germany indicated that the average LOS of breast cancer patients after breast surgery was 6.3 days. These studies show that the LOS standard set at Hasanuddin University Hospital, which is 4–6 days, is generally in accordance with the average LOS of post-surgery breast cancer patients.
Out of 100 respondents who were studied, only 9 people did not reach the standard or did not comply with the established clinical pathway. The increase in LOS of these patients occurred in those who experienced perioperative complications, such as requiring blood transfusions and experiencing surgical site infections. LOS that did not reach the standard was also found in patients who underwent breast reconstruction surgery simultaneously after mastectomy. This finding is consistent with a study which stated that the prolongation of LOS in patients undergoing mastectomy surgery occurred those who underwent direct breast reconstruction and emergency surgeries and had certain comorbidities [23]. Respondents in this study with comorbidities, such as diabetes mellitus, coronary artery disease, stroke, other types of cancers, and kidney and other lung diseases, were excluded.
Statistical analysis in this study showed no relationship between PCC application and LOS. Based on the preceding result, a study conducted in Pittsburgh also showed insignificant results between PCC in treatment groups of patients undergoing gastric bypass surgery for hospital LOS. Nurses who provided PCC received 10 h of education that focused on enhancing communication, negotiation, and patient education to improve the interaction between nurses and patients. The training included role playing to further develop skills and confidence. During the preadmission call, the PCC nurses obtained information from the patient that identified his or her perceptions, goals, concerns, and fears regarding hospitalization. This information was used to initiate the patient’s plan of care before hospital arrival. During their hospital stay, participants in the PCC group were actively involved in planning their daily activities/plan of care, establishing daily goals, and planning for their transition to home. Trained nurses were not allowed to interact with participants in the regular care group. This lack of difference between quality indicators could have been supported by the balance between nurses in age and years of experience when caring for both groups [24]. Another study that assessed the relationship between PCC implementation and LOS with insignificant results was that conducted by Cropley (2012). The PCC intervention was in the form of implementing PCC with the relationship-based care (RBC) model, which included the dimensions of (1) communication with nurses, (2) responsiveness of hospital staff, (3) pain management, (4) communication about medicines, and (5) discharge information. The intervention is in the form of training for hospital leaders and staff to implement and instill PCC implementation according to the RBC model. The research was conducted in 2009 and 2010. Data in 2009 and 2010 are regarded as pre- and post-implementation data of the RBC model, respectively. The results showed no significant relationship between PCC implementation and patient LOS. This finding is thought to be due to the location of the study, which is conducted in a small rural hospital in Texas. Therefore, results may not be generalizable to large populations. In addition, the method of admission and discharge of patients followed regionally and culturally acceptable regulations and prevailing norms; therefore, they could not assess the impact of PCC implementation [25]. The LOS of postoperative breast cancer patients is good with an achievement of 91%. However, this result still did not prove a significant correlation between the application of PCC and LOS based on statistical analysis. The LOS achievement was assessed because of the good implementation of clinical pathways. Similarly, the research conducted by Pritts et al. (1999) also showed that the application of clinical pathways was proven to reduce the length of treatment significantly compared with the group treated without the clinical pathway [26]. In addition, insignificant results occurred because no mutually agreed definition of PCC has been established at Hasanuddin University Hospital. PCC implementation in hospitals requires an identifiable framework or implementation guideline to conduct PCC interventions. Without such basic information, PCC implementation runs the risk of inconsistency or absence of improvement [2]. Regarding LOS, PCC has remarkable potential to maximize patient LOS with good discharge planning while maintaining patient satisfaction as in previous studies. Even in some developed countries, several studies show that mastectomy surgery can be performed currently as a one-day surgery; therefore, the average LOS of patients is 1–2 days of course by applying PCC principles [27–30].
Correlation between PCC application and patient satisfaction
The correlation between PCC application and patient satisfaction in this study proved significant. Satisfaction can generally be achieved when quality can meet the expectations and needs of patients. The quality of healthcare and patient safety improves when healthcare administrators, hospitals, patients, and families work together in a partnership, resulting in increased patient satisfaction [31]. A study showed that implementing PCC by acknowledging the specific care needs of a patient may result in remarkably affectionate and trusting interactions with the care provider, fulfilling the need for affection and behavioral confirmation of the patient, which resulted in increased patient satisfaction [32].
In the result of the PCC application, the highest percentage among all dimensions of PCC was the dimension of “respect for the patient’s values, preferences, and needs”, Docteur and Coulter (2012) defined this dimension as the core dimension of PCC, “A patient-centered healthcare system and the processes associated with service delivery are designed to anticipate and respond to patient’s concerns and solicit meaningful patient input in all decisions regarding how health care is furnished [19]”. This achievement supported the increasing patient satisfaction at Hasanuddin University Hospital. A study conducted by Wolf et al. (2008) showed a significant difference in the satisfaction of patients treated with PCC compared with those who did not. The application of PCC in this study was in the form of preadmission interviews by telephone, which enabled nurses to initiate PCC interventions before patient arrival and develop treatment plans with a comprehensive understanding of patient expectations, perceptions, and concerns. This intervention attempts to make patients feel welcome, comfortable, less anxious, and actively involved in their care. In addition to patient satisfaction, the satisfaction of nurses who run PCC also increased. On average, a PCC nurse estimates spending 10 to 20 additional min with each patient. However, this additional time does not affect the ability to complete other daily routines/tasks [24]. Another study showed that the implementation of PCC in an acute care setting leads to an increase in the level of patient satisfaction with care. This positive relationship is consistent with findings from previous studies conducted in various places [33–35]. Working together according to the needs and preferences of patients in solving their health problems endows patients the perception that they are cared for well, which translates into increased satisfaction levels [36].
In addition, the study by Abubakar et al. (2020) proved the effect of PCC application on patient satisfaction after cesarean section in Makassar in two Mother and Child Hospitals. The implementation of PCC was also assessed using a PCC questionnaire instrument with eight dimensions, with the highest result also being on the dimension “respect for the patient’s values, preferences, and needs.” The PCC application increases patient perceptions of improved healthcare quality and create new value in services. This phenomenon explains the reasons for implementing PCC, which positively impacts patient satisfaction [37]. Other studies on cataract surgery patients also demonstrated similar results to the application of PCC in this study in the form of preoperative assessment, patient education, informed consent, and management of surgical outcome expectations. Education in this study is in the form of basic knowledge about cataract disease, the effect of cataracts on patient care and surgical procedures. This study indicates that patient education is one of the important dimensions in the application of PCC [38]. In another study, Mallinger et al. (2005) surveyed 182 patients who had completed active treatment for breast cancer. Patients reported implementing PCC in their interactions with their physicians, providing improved mental health outcomes and demonstrating increased satisfaction with the information they received regarding treatment options and survival issues. Mallinger et al. (2005) concluded that providers using a PCC approach know patients beyond their biomedical needs, and this can assist in individualizing information for each patient [39].
Therefore, the application of PCC plays a role in increasing patient satisfaction and is proven to have a statistically significant relationship based on the aforementioned explanations. The application of PCC, namely making partnerships with patients and their families and individualizing treatments, specifically according to patient needs and preferences, can generally increase patient satisfaction with services. The needs and expectations of patients for the desired service quality can be met by fulfilling the PCC principles. This explains why the application of PCC is said to be related to patient satisfaction at Hasanuddin University Hospital.
Correlation between PCC application and clinical outcome
The clinical outcome assessed in this study was surgical site infection (SSI). This site is defined as an infection occurring within 30 days after a surgical operation and affecting either the incision or deep tissues at the operation site [40]. The clinical outcome was successfully achieved if three clinical outcome indicators comprising superficial, deep, and space/organ infections are absent. Data regarding the clinical outcome of a patient were assessed in the medical record of the patient before its discharge. In this study, the statistical test showed no correlation between PCC application and clinical outcome. Many previous studies showed that the application of PCC has a positive impact on clinical outcomes, such as reducing postoperative complications, postoperative pain, anxiety, increased physical well-being and social well-being through the combination of teamwork, communication, interpersonal relationships, understanding, appreciation, and flexibility; however, the current study proved otherwise [4,6,13,32,41–43].
A cross-sectional study of post-cesarean patients in Makassar revealed that PCC has no effect on the clinical outcomes of patients in the form of LOS, phlebitis, SSI, and hospital-acquired infection. The clinical outcomes in this study were influenced by many factors other than PCC, including the application of clinical pathways and infection control and prevention programs at the hospital [1]. Another study on chronic disease patients explained that the application of PCC by implementing patient-centered communication can increase patient satisfaction but cannot modify patient outcomes, such as health status, because patient-centered communication emphasizes interpersonal aspects between patients and service providers [44]. In addition, most of the patients who participated were diagnosed with a chronic disease, but their health status may have remained relatively unchanged by definition. Furthermore, the two-week evaluation time in this study may be excessively short to detect patient-reported health changes. In addition, the lack of a correlation between PCC application and health outcomes may indicate that the correlation is nonlinear, and excessive patient-centered communication may have a poor relationship with patient outcomes. Physicians can also lose focus on the disease because they provide excessive attention to the disease experience of the patient [45].
Another study assessed the correlation between the application of PCC in the form of patient autonomy in making clinical decisions with two clinical outcome variables, namely subjective and objective clinical outcomes. In the clinical outcome objective variable that was assessed, glycemic control in the form of HbA1c was evaluated from the medical record of the patient while the subjective clinical outcome was from the quality of life physically and mentally. The results proved the absence of correlation between the application of PCC with glycemic control and physical quality of life. The implementation of PCC is said to require changes in the healthcare system by improving the overall quality of care to be able to influence patient clinical outcomes. PCC applications require clear definitions and training in their application [46,47]. Another study that assessed the relationship between the application of PCC and glycemic control in the form of HbA1c also provided insignificant results. The results of this study indicate that PCC has an influence on the self-care behavior of a patient but does not have a sufficient impact to produce sustainable behavioral changes that can improve glycemic control. In this study, the application of PCC must fulfill all medical treatment processes, not only certain processes. These findings suggest that PCC is an important factor in diabetes self-management but may need to be extended to the rest of the healthcare system before changing outcomes, such as glycemic control [48]. Similar results were also obtained in the study of Gulliford, Naithani, and Morgan (2007), who found that PCC application was associated with satisfaction in type 2 diabetic patients 10 months after their initial visit but was not associated with clinical outcomes, such as HbA1c, systolic blood pressure, BMI, or physical component scores on the SF-12 [49]. These studies reveal that the relationship between PCC implementation and clinical outcomes is still mixed. Donabedian (1988) emphasized that many important patient outcomes can only be observed in the long term and many additional variables may emerge, increasing the difficulty of the identification of immediate predictors [4]. Another factor contributing to this study lies in surgical site infection (SSI), which is the assessed clinical outcome. SSI is defined as infections occurring within 30 days after a surgical operation and affecting either the incision or deep tissue at the operation site. This study assessed the SSI only up to 3 days after operation because the LOS according to the clinical pathway of the surgical breast cancer patient in the hospital is 4–6 days. However, SSIs are most commonly reported between days 7 and 9 [50,51]. In addition, SSI was associated with patient-related factors, including old age, preexisting infection, colonization with Staphylococcus aureus and other potential pathogens, and smoking. Procedure-related factors, including poor surgical technique, duration of surgery, quality of preoperative skin preparation, and inadequate sterilization of surgical instruments, also influence the occurrence of wound infections [51,52].
Therefore, the insignificant relationship between PCC implementation and clinical outcomes could be influenced by many other factors that were not investigated. The achievement of the incidence of surgical wound infections, which only reached 4% and did not meet the standards, can occur because the implementation of PCC at Hasanuddin University Hospital did not yet have the framework and guidelines as previously described and had not been applied to the entire patient care process. In addition, the aforementioned phenomenon might occur because the hospital infection control and prevention program has not been implemented properly at Hasanuddin University Hospital.
Conclusions
The study showed that the application of PCC was attributed to patient satisfaction but was not correlated to the LOS and clinical outcomes in post-surgical breast cancer patients. The hospital should improve the application of PCC, specifically in the dimension of access to care. In addition to the hospital accessibility for all patients (such as a conveniently located hospital for the patient), access to specialists or specialty services, easily scheduled appointment, and acceptable waiting time should get additional attention. However, the hospital should create an accepted definition and commonly agreed set of dimensions used for the concept of operationalization and its measurement to implement PCC and improve overall patient satisfaction and clinical outcome and reduce the LOS as expected. A large sample size is also needed to examine the impact of PCC application on LOS and clinical outcomes of patients.
Footnotes
Conflict of interest
The authors declare no conflict of interests.