
Abstract
Keywords
Introduction
The World Health Organization (WHO) emphasizes the importance of integrating patient perspectives into healthcare evaluations to improve service delivery, enhance patient outcomes, and strengthen health systems.1,2 In recent years, patient-centered care has emerged as a key determinant of healthcare effectiveness.3–5 This approach places the individual patient's unique needs, preferences, values, and circumstances at the center of all clinical decisions and care delivery. 3 It emphasizes the importance of understanding how patients perceive their interactions with healthcare providers, the care environment, and their overall healthcare experience.4,5
Two primary approaches to capturing patient perspectives in healthcare quality assessment are patient satisfaction and patient experience. 6 Traditionally, healthcare systems rely on patient satisfaction surveys to gauge performance. 7 However, many researchers argue that general satisfaction ratings are insufficient for capturing the complexities of modern healthcare and the diverse expectations of patients.4,8–10 While closely related, patient experience and patient satisfaction are conceptually distinct. 4 Patient experience focuses on what actually occurred during the care process—such as communication with providers and timeliness of services—whereas patient satisfaction reflects how well these experiences met individual expectations.10,11 The Donabedian model provides a useful framework for understanding this distinction, categorizing healthcare quality into structural components (eg, facilities and staff), process elements (eg, communication and care delivery), and outcomes (eg, patient satisfaction). 12 From this perspective, improvements in structure and process are expected to enhance patient experience, which in turn influences overall satisfaction. 12
High-income countries are increasingly shifting from assessing patient satisfaction to systematically monitoring patient experiences. 13 For instance, the National Health Service (NHS) in England introduced a national patient survey in 2001, followed by the United States with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. Countries such as Australia, New Zealand, and many in Europe have also institutionalized national strategies for measuring patient experience. 14 Prominent organizations, such as the Picker Institute, the Health Foundation, and the Beryl Institute, now advocate for experience-based measures over traditional satisfaction ratings. Most validated instruments, including the Picker Patient Experience Questionnaire and the HCAHPS survey, focus primarily on patient experience, with only a few items assessing overall satisfaction. Findings from these tools indicate that patients’ satisfaction is often shaped by specific aspects of their care experiences. 4 Despite this global shift, research on patient experience in low- and middle-income countries (LMICs), particularly in sub-Saharan Africa, including Ghana, remains limited. 15
Ghana's healthcare system—comprising public, private, and traditional providers—is structured into 3 main levels: primary, secondary, and tertiary care. The public system includes a wide network of facilities ranging from community-based health planning and services (CHPS) compounds to teaching hospitals. 16 Oversight is provided by the Ministry of Health, with service delivery primarily managed by the Ghana Health Service and other implementing agencies. 17 While reforms such as the National Health Insurance Scheme (NHIS) have improved access to care, 18 gaps remain in understanding how patients perceive their hospital experiences. Existing studies have largely focused on general satisfaction and perceived service quality,19–25 with limited empirical research specifically examining patient experience in Ghanaian healthcare settings. 15 Moreover, challenges such as staff shortages, overcrowding, and inadequate pain management practices are widespread in Ghanaian hospitals 15 and have important implications for patient experience outcomes. Studies in other resource-limited settings, such as Smerat et al, 26 have similarly highlighted how staffing constraints and overcrowding undermine service quality and patient-reported experiences, suggesting cross-regional parallels. In addition, Salim et al 27 underscore barriers in pain management for intubated patients, a gap that resonates with documented concerns in Ghanaian inpatient care. These contextual challenges reinforce the need to investigate how patients perceive their care in order to identify priorities for improving service delivery.
Therefore, this study explores patient experiences of inpatient care and examines how these experiences relate to patient characteristics in a multicentered sample of hospitals in Ghana. By addressing this gap, the study provides context-specific insights into patient-centered care in a low- and middle-income setting. The findings are expected to contribute to the literature on patient experience and offer evidence to guide healthcare managers, policymakers, and providers in strengthening the quality and responsiveness of hospital services in Ghana.
Methods
An institution-based cross-sectional study was conducted between July 2024 and February 2025 among inpatients admitted to the medical and surgical wards of 8 hospitals across the Central, Western, Ashanti, and Northern Regions of Ghana. The hospitals were selected using a convenience sampling strategy due to practical limitations, including budgetary constraints, and logistical challenges. This selection method enabled the inclusion of hospitals where participant access was feasible. The selected facilities were Effia Nkwanta Hospital, Kwesimintsim Hospital, and Father Thomas Alan Rooney Memorial Hospital in the Western Region; Effutu Municipal Hospital and Trauma and Specialist Hospital in the Central Region; Kumasi South Hospital and Saint Martin's Hospital in the Ashanti Region; and Tamale West Hospital in the Northern Region.
Eligible participants were adult inpatients aged 18 years and older who had received care for a minimum of 24 h, were mentally sound, and were willing to participate. A total sample size of 1304 was estimated based on a similar study by Min et al, 28 which involved 1300 participants. The sample was slightly increased to ensure an equal distribution of 163 participants across the 8 hospitals. Recruitment was carried out using consecutive sampling, where eligible patients admitted to the wards were approached sequentially during the data collection period until the required number of participants per hospital was attained.
Patient care experiences were measured using the Picker Patient Experience Questionnaire-15 (PPE-15), a validated instrument developed from the original Picker Patient Experience Questionnaire. 29 The PPE-15 consists of 15 items assessing various dimensions of inpatient care, including information and education (items 1 and 2), coordination of care (item 3), physical comfort (item 10), emotional support (items 4, 8, and 9), respect for patient preferences (items 5-7), involvement of family and friends (items 11 and 12), and continuity and transition (items 13-15). Response options vary by item, ranging from 2 choices (“yes” or “no”) to 4 (“yes,” “no,” “I did not need to,” or “yes, to some extent”). In the original coding, responses such as “I did not need to” and the most favorable answers are scored as “non-problems” (score = 0), while the others are marked as “problems” (score = 1).
For the purpose of this study, the coding was reversed so that responses indicating problems were assigned a score of 0 and positive responses were scored as 1, making higher scores indicative of better care experiences. This adjustment was undertaken to improve the interpretability of the results, ensuring that higher scores consistently reflected more favorable patient experiences, in line with conventional practice in patient-reported outcome measures. 30 Importantly, the recoding did not alter the structure, content, or dimensionality of the PPE-15, but only reoriented the scoring for ease of analysis and clarity in reporting. Similar recoding strategies have been applied in previous applications of the PPE-15 and related patient experience tools,28,31 supporting the validity and integrity of this approach.
In addition to care experience, the PPE-15 captures demographic and clinical details—such as age, gender, education, ward type, length of stay, prior hospital experience, and perceived health status—as well as overall satisfaction and likelihood of recommending the hospital to family and friends. These variables were used to gather the inpatients’ information and to assess their overall evaluation of the care received.
The reliability of the PPE-15 was evaluated using Cronbach's alpha and item-to-total scale correlations corrected for overlap, based on Pearson's correlation coefficient. The internal consistency was satisfactory, with a Cronbach's alpha of 0.79. Item-to-total correlations ranged from r = 0.38 for item 5 to r = 0.65 for item 7, indicating acceptable coherence between individual items and the overall scale.
Data collection was undertaken through structured face-to-face interviews. Patients who met the inclusion criteria were identified after discharge to ensure they could reflect on their entire hospital experience. After the purpose of the study was explained, verbal consent was obtained before interviews commenced. This approach ensured uniformity and reliability in data collection across all sites. In each hospital, we engaged 2 trained research assistants to assist with data collection.
Collected data was entered into Microsoft Excel and analyzed using the Statistical Package for Social Sciences (SPSS) version 20 (IBM© Corporation, Armonk, NY, USA). Descriptive statistics were computed, with continuous variables summarized using means and standard deviations, and categorical variables presented as frequencies and percentages. An overall PPE-15 score, along with domain and item-specific scores, was computed by dividing the total number of positive responses by the total number of applicable items and multiplying by 100, resulting in a score range from 0 to 100. The overall satisfaction rating was converted to a 0–100 scale, where 0 denoted complete dissatisfaction and 100 denoted complete satisfaction. The association between the total PPE-15 score and satisfaction rating was examined using Pearson's correlation, while the relationship between the total PPE-15 score and hospital recommendation was analyzed using Spearman's rank correlation. To explore the relationship between the total PPE-15 score and patient characteristics, a multiple linear regression model was applied. Scatter plots were used to examine linearity between the dependent variable (total PPE-15 score) and explanatory variables (patient characteristics). The normality of the dependent variable was confirmed via the Kolmogorov-Smirnov test (P > .05). Multicollinearity among independent variables was assessed through a correlation matrix and variance inflation factors (VIFs), with correlation coefficients ranging from 0.02 to 0.41 and VIF values between 1.09 and 1.72, both indicating no multicollinearity concerns. Statistical significance for all analyses was determined at a P-value of <.05.
Results
Of the 1304 questionnaires administered, 1220 (93.6%) were included in the final analysis. The remaining 84 (6.4%) were excluded due to having more than 50% missing values. The majority of the respondents were aged between 18 and 35 years (61.15%), with a mean age of 35.9 ± 13.5 years. More than half (54.5%) were female. Most respondents had attained at least a secondary level of education (73.9%). A higher proportion (53.1%) were admitted to medical wards. The majority had a hospital stay of one week or less (80.2%) and had no prior hospitalization experience (56.1%). Regarding health status, over half (53.4%) reported being in good health. Details of the respondents’ characteristics are presented in Table 1.
Characteristics of the Respondents (n = 1220).
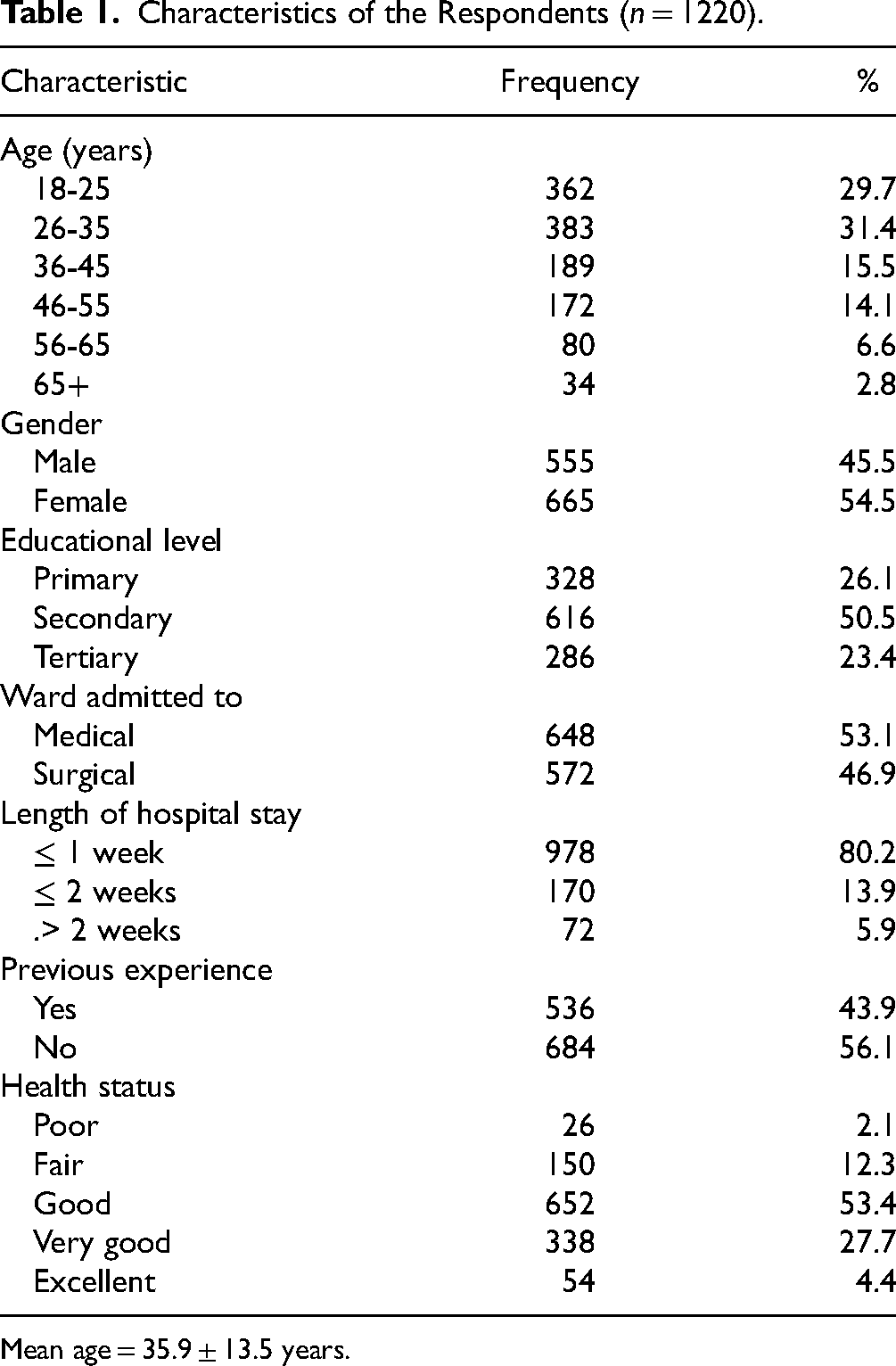
Mean age = 35.9 ± 13.5 years.
Inpatient Care Experiences
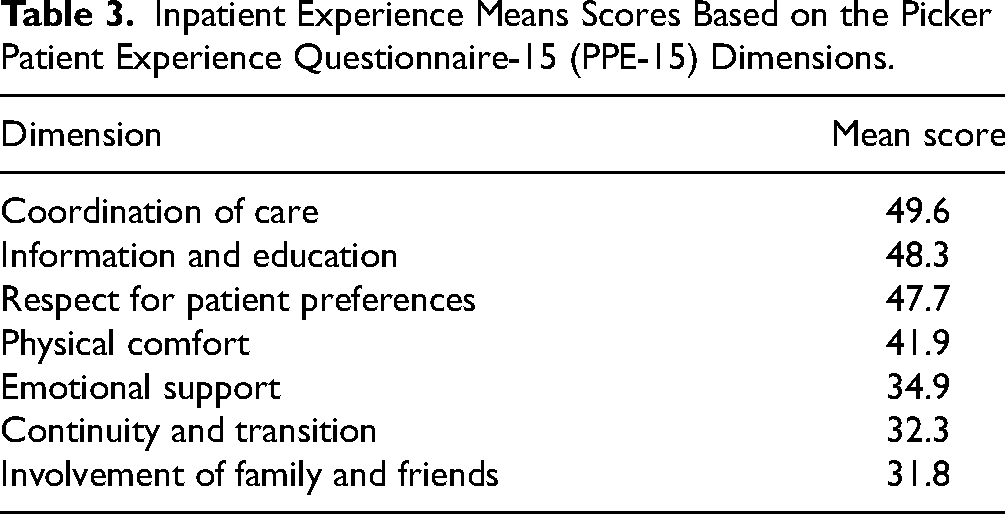
The total inpatient experience score was below average at 39.8 ± 11.2 (range, 6.7-100), with the weakest contributions stemming from key areas that directly affect patients’ overall well-being and recovery. The lowest scoring dimensions were involvement of family and friends (31.8) and continuity and transition (32.3), underscoring substantial deficiencies in postdischarge preparation and external support. For instance, 70.7% of patients reported that their families did not receive adequate information to assist in their recovery, and 73.2% were not informed about potential side effects of medications before discharge. These figures point to critical communication breakdowns during discharge planning.
Emotional support also emerged as a significant area of concern, scoring only 34.9. Alarmingly, 65.2% of respondents indicated they could not find someone on the hospital staff to talk to about their fears or anxieties. Pain management was another notable shortfall, with 58.1% of patients feeling that hospital staff did not do everything possible to control their pain. More details are provided in Tables 2 and 3.
Responses to the Picker Patient Experience Questionnaire-15 (PPE-15) Items (n = 1220).
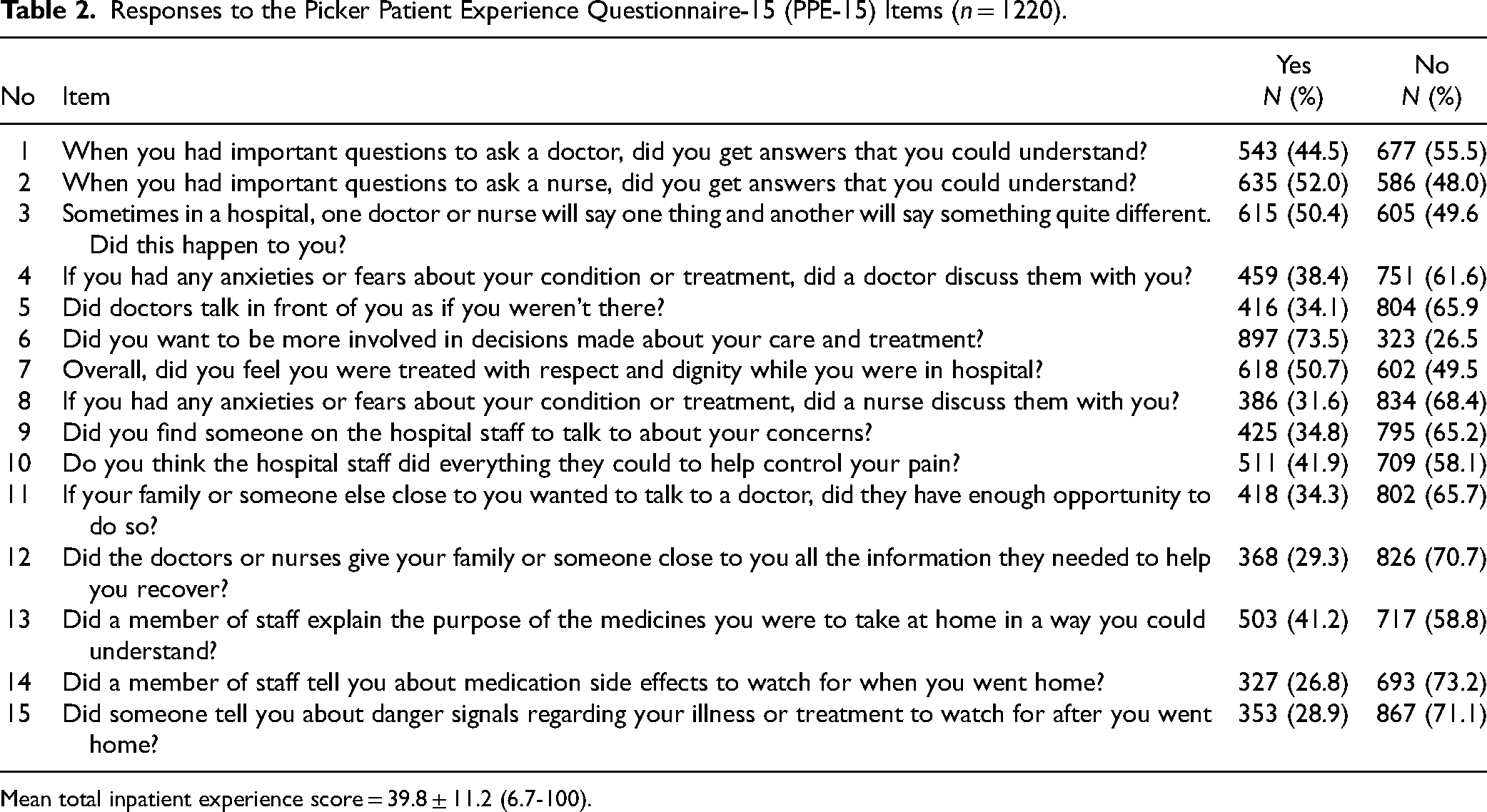
Mean total inpatient experience score = 39.8 ± 11.2 (6.7-100).
Inpatient Experience Means Scores Based on the Picker Patient Experience Questionnaire-15 (PPE-15) Dimensions.
Overall Satisfaction Ratings and Their Relationship With Inpatient Care Experiences
The overall inpatient satisfaction score was 61.2 ± 19.4 (20-100), indicating a moderate level of satisfaction among the inpatients. Regarding recommendation of the hospital to friends and family, 79.1% of respondents were likely to recommend it (48.7% “probably yes” and 30.4% “definitely yes”), while 22.9% were unlikely to do so (14.8% “probably no” and 8.1% “definitely no”) (see Supplemental Figure S1). A significant positive correlation was observed between the total inpatient experience score and both overall satisfaction (r = 0.425, P < .001) and recommendation of the hospital (ρ = 0.257, P < .001).
Association Between Overall Inpatient Experience Score and Patient Characteristics
The multivariable linear regression analysis revealed that age, level of education, ward type, length of stay, previous experience, and health status were significantly associated with inpatient experience. Older age (B = 0.287, P < .001), higher education level (B = 4.403, P < .001), and better health status (B = 8.718, P < .001) were positively associated with higher inpatient experience scores. In contrast, admission to a surgical ward (B = –2.775, P = .007), longer hospital stays (B = −0.303, P = .005), and previous hospital experience (B = −4.830, P < .001) were linked to lower scores. Gender was not significantly associated with inpatient experience (P = .065). The model explained 23.7% of the variance in inpatient experience scores (R2 = 0.237). More details are presented in Table 4.
Multivariable Linear Regression Results of the Association Between Inpatient Experience and Patient Characteristics.

Statistically significant at P = .05, CI = confidence interval, R2 = 0.237.
Discussion
Overall, the inpatient experience score was below average, highlighting that a significant proportion of patients encountered considerable challenges during their hospital stay. This poor rating reflects not just isolated service gaps, but systemic deficiencies within Ghana's inpatient care system. In particular, the low scores in discharge communication, emotional support, pain management, and family involvement point to deeper structural and operational shortcomings in patient-centered care practices. In the Ghanaian context, where healthcare systems often operate under constraints such as staff shortages, limited training in patient communication, and overcrowded facilities,32,33 these challenges are further exacerbated. The observed lack of clear communication regarding postdischarge care and medication side effects not only increases the risk of complications and readmissions but also undermines trust in the health system. Similarly, the failure to provide emotional support or involve family members in care reflects a gap in holistic approaches to healing. This is especially relevant in culturally communal societies such as Ghana, where collectivist norms—as described by Hofstede's framework—position the family as a central actor in caregiving. In this context, limited family engagement not only diminishes patient well-being but also reduces the effectiveness of care coordination.34,35 These findings underscore the urgent need for policy and institutional reforms focused on improving interpersonal aspects of care, enhancing staff-patient communication, and integrating family involvement as a standard part of inpatient care in Ghana.
Although the overall satisfaction score was moderate, the notably low inpatient experience score indicates that relying solely on satisfaction ratings may not provide a comprehensive or accurate reflection of the true quality of care or the full spectrum of patient needs. Expectation confirmation theory offers an explanation for this discrepancy: patients may report moderate satisfaction when their baseline expectations are already modest, even if their actual care experiences are suboptimal. 36 This helps to explain why satisfaction scores appear somewhat favorable despite clear evidence of deficiencies in patient experience. This observation is consistent with the extant literature, which emphasizes that patient satisfaction scores can sometimes mask underlying issues related to the patient experience.4,6,8,37 Nevertheless, the observed positive correlation between the total inpatient experience score and overall satisfaction indicates that patients who report better experiences also tend to express higher satisfaction. This suggests that enhancing the specific dimensions of patient experience—such as effective communication, emotional support, and coordinated discharge planning—can directly contribute to higher levels of patient satisfaction. In the context of Ghana's healthcare system, this underscores the importance of investing in systemic improvements that address both the technical and interpersonal aspects of care to achieve meaningful gains in patient-centered outcomes.
The observed associations of higher inpatient experience scores with older age, better health status, and higher education align with existing literature,38–40 which suggests that these groups tend to report more favorable experiences—likely due to factors such as greater health literacy, 38 more realistic expectations,38,39 and higher levels of engagement with healthcare providers. 40 In contrast, the lower experience scores linked to surgical ward admissions, longer hospital stays, and prior hospitalizations reflect well-documented challenges, as these factors are often associated with more complex care needs, increased physical and emotional stress, and greater exposure to systemic shortcomings, all of which can negatively influence patient perceptions of care.41,42
Study Limitations
Several limitations should be acknowledged when interpreting the findings of this study. The use of convenience sampling limits the generalizability of the results to all hospitals in Ghana. The sample was restricted to adult inpatients from medical and surgical wards, thereby excluding important populations such as pediatric, maternity, and other specialized unit patients whose experiences may differ significantly. Data were collected through self-reported responses, which are prone to biases such as social desirability and recall error, particularly given the face-to-face interview format. Although interviewers received standardized training, the potential for interviewer influence cannot be fully ruled out, raising ethical considerations around response accuracy. Additionally, Ghana's unique healthcare infrastructure, shaped by reforms such as the National Health Insurance Scheme (NHIS), may limit the comparability of these findings with those from other low- and middle-income countries. Despite these limitations, the study provides valuable insights into patient experiences and satisfaction in Ghanaian hospitals and offers a foundation for future research and quality improvement efforts.
Conclusion
This study highlights the importance of patient experience as a distinct and essential component of healthcare quality assessment in Ghana. The findings demonstrate that overall satisfaction scores alone may not fully capture the complexities of inpatient care. A deeper insight into patients’ actual interactions and perceptions can inform meaningful improvements in care delivery. As Ghana continues to strengthen its health system, incorporating patient perspectives will be critical to advancing patient-centered care and enhancing hospital performance.
Practice Implications
The findings of this study have important implications for healthcare practice in Ghana, particularly the need to strengthen patient-centered care across hospitals. Low scores in areas such as discharge communication, emotional support, pain management, and family involvement indicate that the interpersonal and supportive dimensions of care are not receiving adequate attention. These deficiencies call for system-level action in staff training, policy development, and future research.
First, incorporating empathetic communication modules into continuous professional development programs for healthcare providers, as supported by the literature, 43 could enhance provider–patient interactions and responsiveness to patient needs. In terms of policy, the development of standardized discharge protocols and the creation of family liaison roles would help ensure that patients receive clear, consistent information and that families are meaningfully engaged in the care process, reflecting the communal caregiving traditions central to Ghanaian society. From a research perspective, the adoption of mixed-methods designs would allow for a more comprehensive understanding of unmet patient needs. Moreover, the disparities observed across subgroups—particularly among surgical patients and those with longer hospital stays—underscore the importance of targeted strategies. Integrating comprehensive patient experience metrics, beyond general satisfaction, into routine hospital performance assessments can help drive sustained quality improvement and foster more responsive, equitable, and holistic inpatient care in Ghana.
Figure 1 presents a conceptual model of the key drivers of inpatient experience identified in this study, and how they influence overall satisfaction and patient-centered outcomes. This model can guide hospital managers, policymakers, and educators in designing interventions that strengthen patient-centered care in Ghana. Details of the model are provided as a Supplemental Material (see Supplemental Figure S2).

A Conceptual Model of the Key Drivers of Inpatient Experience and Overall Satisfaction.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251406355 - Supplemental material for Patient Experience of Inpatient Care: Insights From a Multicentered Study in Ghanaian Hospitals
Supplemental material, sj-docx-1-jpx-10.1177_23743735251406355 for Patient Experience of Inpatient Care: Insights From a Multicentered Study in Ghanaian Hospitals by Veronica Penaman Asamoah, Emmanuel Kumah, Michael Afari Baidoo, Samuel Egyakwa Ankomah, Adam Fusheini and Samuel Kofi Agyei in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251406355 - Supplemental material for Patient Experience of Inpatient Care: Insights From a Multicentered Study in Ghanaian Hospitals
Supplemental material, sj-docx-2-jpx-10.1177_23743735251406355 for Patient Experience of Inpatient Care: Insights From a Multicentered Study in Ghanaian Hospitals by Veronica Penaman Asamoah, Emmanuel Kumah, Michael Afari Baidoo, Samuel Egyakwa Ankomah, Adam Fusheini and Samuel Kofi Agyei in Journal of Patient Experience
Footnotes
Acknowledgments
Not applicable.
Authors Contributions
Veronica Penaman Asamoah: formal analysis, methodology, investigation, and writing original draft. Emmanuel Kumah: conceptualization, investigation, supervision, methodology, formal analysis, and writing review and editing. Michael Afari Baidoo: methodology, formal analysis, writing review and editing. Samuel Egyakwa Ankomah: formal analysis, and writing review and editing. Adam Fusheini: formal analysis, and writing review and editing. Samuel Kofi Agyei: formal analysis, and writing review and editing.
Data Availability Statement
The data used in this analysis are available from the corresponding author on request.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Institutional Review Board of the Ghana Health Service (Protocol No. GHS-ERC: 037/10/24). In addition, we obtained permission from the authorities of the participating hospitals before commencing the study. All participants provided oral informed consent prior to their involvement in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.