
Abstract
ER−/PR+ is a controversial subtype and is not formally recognised as molecular subtype of breast carcinoma. Few studies concluded that this subtype does not exist and is due to technical errors, however, in contrast others consider it to be distinct entity with different response to therapy and clinical outcome. It is also essential to know whether this subtype shows any distinct histomorphological features or prognosis.
Therefore, the present two cases of controversial subtype ER−/PR+ breast cancer is being reported with both the cases showing neuroendocrinal differentiation.
Introduction
Steroid hormone estrogen and progesterone receptors (ER and PR) along with human epidermal growth factor receptor-2 (HER-2 neu) are essential for clinical management and prognosis of breast carcinoma. Immunohistochemical expression of these biomarkers provides molecular classification of breast carcinoma which is broadly classified into Luminal A, Luminal B, HER-2 neu and triple negative breast carcinoma [1]. ER is a nuclear receptor which controls various estrogen regulated genes including progesterone receptor encoding gene [2]. The subtypes of ER+/PR+, ER−/PR− and ER+/PR− have been well recognised, however ER−/PR+ is a controversial subtype and is not formally recognised. Few studies concluded that this subtype does not exist and is due to technical errors [3,4]. However, in contrast others consider it to be distinct entity with different response to therapy and clinical outcome [5]. It is also essential to know whether this subtype shows any distinct histomorphological features of breast carcinoma.
Therefore, the present two cases of controversial subtype ER−/PR+ breast cancer is being reported with both the cases showing neuroendocrinal differentiation.
Case reports
Case 1
A 46 year old female presented with a lump in left breast for one month of size 1 cm. Digital mammography showed dense nodular opacity of 16 × 14 mm in left breast without axillary lymphadenopathy (Fig. 1). Ultrasonography of breast showed irregular lobulated hypoechoic mass with microcalcifications. Core needle biopsy was done which was reported as poorly differentiated malignant tumor with neuroendocrinal differentiation (Fig. 2). It was followed by modified radical mastectomy which confirmed diagnosis of small cell carcinoma, modified Richardson Bloom index of 8, Grade III. Necrosis was present with high mitotic rate of 12-13/10 high power field and lymphovascular invasion. On immunohistochemical staining ER was negative, PR was positive, HER-2 neu was negative (score 0), Ki 67 was 90%, CD 45 negative, CD56 and synaptophysin positive (Fig. 2). In view of ER−/PR+ status repeat immunohistochemistry was done which gave similar results. The patient was subjected to etoposide and cisplatin based chemotherapy. Presently she is doing well and is on regular follow up since last eight months.
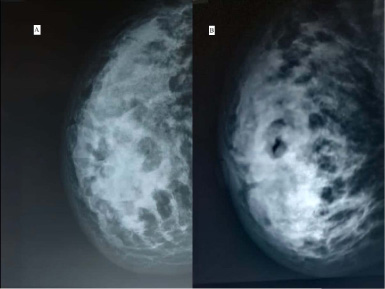
Mammogram of breast in Case 1 (A) and Case 2 (B) showing dense irregular opacity in breast.
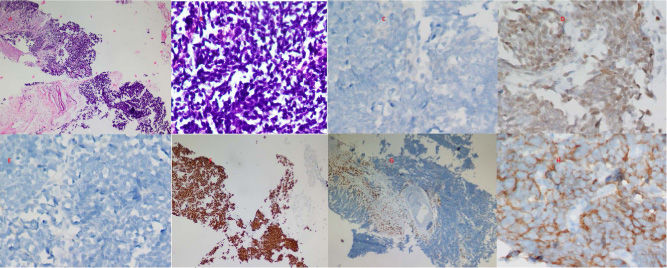
(A) Section from breast biopsy shows infiltration by cellular poorly differentiated tumor (HE; ×10). (B) Section shows malignant tumor with neuroendocrinal differentiation (HE; ×20). (C) Immunohistochemical expression showing ER negativity (ER IHC; ×20). (D) Immunohistochemical expression showing PR positivity (PR IHC; ×20). (E) Immunohistochemical expression showing HER-2 neu negative score (IHC; ×20). (F) Immunohistochemical expression showing 90% Ki67 positivity (Ki 67 IHC; ×10). (G) Immunohistochemical expression showing CD45 negativity (CD45 IHC; ×10). (H) Immunohistochemical expression showing Synaptophysin positivity (Synaptophysin IHC; ×40).
A 40 year old female presented with lump in left breast for 2 months. Mammogram revealed an irregular hypoechoic mass measuring 3.6 × 2.8 cm in upper outer quadrant of left breast (Fig. 1).
A core needle biopsy was done which was reported as round cell malignancy (Fig. 3). Modified radical mastectomy was done which on histopathology was reported as neuroendocrinal tumor, modified Richardson Bloom index of 8, Grade II. Necrosis was present with high mitotic rate of 7-8/10 high power field and lymphovascular invasion. On immunohistochemical staining ER was negative, PR was positive, HER-2 neu was negative (score 0), Ki 67 was 90%, CD 45 negative and CD56, synaptophysin positive which on repeat immunohistochemistry also gave similar results (Fig. 3). The patient was subjected to chemotherapy comprising of 4 cycles of adriamycin and cyclophosphamide with 4 cycles of taxane based chemotherapy. Presently the patient is doing well and is on continuous follow up since last 7 months.
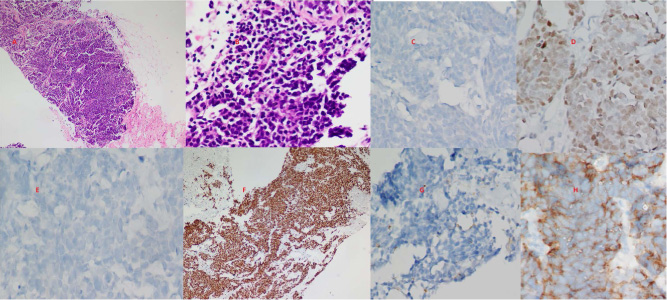
(A) Section from breast biopsy shows infiltration by cellular round cell tumor (HE; ×10). (B) Section shows malignant tumor with neuroendocrinal differentiation (HE; ×20). (C) Immunohistochemical expression showing ER negativity (ER IHC; ×20). (D) Immunohistochemical expression showing PR positivity (PR IHC; ×20). (E) Immunohistochemical expression showing HER-2 neu negative score (IHC; ×20). (F) Immunohistochemical expression showing 90% Ki67 positivity (Ki 67 IHC; ×10). (G) Immunohistochemical expression showing CD45 negativity (CD45 IHC; ×20). (H) Immunohistochemical expression showing Synaptophysin positivity (Synaptophysin IHC; ×40).
Hormone receptor molecular subtyping of breast cancer is essential for the work up and management of these cancers. ER−/PR+ subtype has been rarely reported in literature with prevalence of 0–8% [6,7]. The controversy associated with this tumor is that whether it is a true subtype or is merely technical error of staining. The re-evaluation of the hormone receptor immunohistochemistry is essential in this regard. The present two cases on re-evaluation also gave similar results of ER−/PR+ as previously. Beltjens et al. re-evaluated 49 cases of ER−/PR+ breast carcinoma and observed 55% to show similar results as given on initial assessment. American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) also recommend that ER−/PR+ immunohistochemical expression cases should be repeated for staining to avoid any technical error [8].
It is also essential to determine the clinical and pathological characteristics of ER−/PR+ tumors. Both the present cases were in the fourth decade and histopathologically showed features of small cell neuroendocrinal differentiation. The mitotic activity was high (1–2/hpf) in both the cases and associated with moderate to severe necrosis. On immunohistochemistry, apart from ER−/PR+ status both the cases were Her 2 neu negative and showed Ki67 proliferation index of 90%. These findings show that ER−/PR+ patients are associated with aggressive behaviour and younger age. Previous studies who have considered this entity as a true subtype of breast carcinoma have observed them to be aggressive and associated with intermediate prognosis between ER+/PR+ and triple negative tumors [5,9]. Recently, it has been suggested that inflammation inhibitor might be a potential option for therapy for ER−/PR+ breast cancer patients rather than hormonal inhibitors [10].
The molecular analysis of this subtype observed the up regulation of genes controlled by the suppressor of zest 12 (SUZ 12) which may play role in tumor biology of these cases and further in therapeutic response [5]. However, in the present two cases molecular analysis was not done.
Thus to conclude the present two cases report infrequent controversial subtype ER−/PR+ of breast carcinoma. Both the cases were observed in younger age group and showed morphological neuroendocrinal differentiation, high proliferative index and Her 2 neu negative status. The authors suggest that further studies may be done to establish ER−/PR+ subtype in breast carcinoma and associated prognosis.
Footnotes
Conflicts of interest
None
Financial support
None
Authors’ contributions
SC: Conception, interpretation and generation of data, drafting of manuscript.
SB: Interpretation of data and drafting of manuscript.
SS: Interpretation of data and providing intellectual input.
All the authors approved the final version of the manuscript.