
Abstract
BACKGROUND:
Breast cancer in Indonesia has continued to increase. One diagnostic modality is immunohistochemical examination to determine breast cancer subtypes.
OBJECTIVE:
To determine breast cancer metastasis and mortality rates based on molecular subtypes.
METHODS:
A descriptive study was conducted based on retrospective data from hospital medical records from January 2016 to December 2019. The data comprised age, clinical stage, histopathological grade, molecular subtype, location, metastasis, and breast cancer mortality. The data were processed and analyzed.
RESULTS:
This study involved 172 patients. The most prevalent breast cancer subtypes were luminal A (60, 34.8%), followed by HER2 (47, 27.4%), triple-negative (38, 22.4%), and luminal B (27, 15.4%). The metastasis rate was 37.21% (64/172), with bone the tissue most affected (32 cases, 50%), followed by lung (24 cases, 37.5%) and liver (8 cases, 12.5%). The highest rates of bone, lung, and liver metastases were subtypes luminal A (31%), HER2 (29%), and triple-negative (38%), respectively. The mortality rate was 21% (36/172), with most in the triple-negative group (28.9%), followed by luminal B (25.9%), HER2 (21.2%), and luminal A (13.3%).
CONCLUSIONS:
Determination of breast cancer molecular subtypes through immunohistochemistry can determine the level of metastasis and mortality in breast cancer.
Introduction
Breast cancer is the most common cancer in women worldwide. In 2012, the number of new cases reached 2 million; this increased to 2.3 million in 2020 [1,2]. It has a mortality rate of 15%. Breast cancer has the second-highest new cancer case incidence, after lung cancer, and the highest in women. Breast cancer represents 1 in 4 cases of cancer in women. In Southeast Asia, the incidence of breast cancer in 2018 reached 41.2 per 100,000 [2]. In Indonesia, the incidence of breast cancer in 2019 reached 42.1 per 100,000, with an average death rate of 17 per 100,000 [3].
Factors affecting breast cancer prognosis are divided into major and minor prognostic factors. The major prognostic factors are invasive cancer versus cancer in situ, metastases to lymph nodes, distant metastases, tumor size, advanced local disease, and inflammatory cancer [4,5]. The minor prognostic factors are histologic subtype, tumor grading, proliferation rate, DNA content, and classical immunohistochemical (IHC) markers such as estrogen receptors (ERs), progesterone receptors (PRs), and human epidermal growth factor receptor-2 (HER2) [4–6].
Breast cancer has different histopathological and biological characteristics, showing different treatment responses. Different therapeutic strategies are also needed [7]. Therefore, determining the breast cancer molecular subtype is performed to allow more accurate treatment [4,7].
According to the Consensus of St. Gallen 2017 [8,9] and Dai et al. [4] breast cancer is divided into four subtypes based on molecular intrinsic IHC examination of the expression of ER, PR, HER2, and proliferative index (Ki-67): luminal A, luminal B, HER2 type, and triple-negative/basal-like.
According to Howlader et al. [10] the breast cancer subtype plays a role in the prognosis of the disease; the 4-year survival rate is 92.5% for luminal A, 90.3% for luminal B, 82.7% for HER2, and 77% for triple-negative. This result led to the 8th American Joint Committee on Cancer (AJCC) in 2018 distinguishing between the anatomic stage and prognostic stage of breast cancer [11]. A study found that in the HER2 population, both the anatomic stage and prognostic stage had the same prognostic value [10,12,13].
No wide study evaluating the metastasis and mortality of breast cancer patients by molecular subtype has been carried out in Indonesia. One study is at Wahidin Sudirohusodo Hospital, Makassar. Therefore, we evaluated metastasis and mortality by molecular subtype among breast cancer patients at our institution from 2016 to 2019.
Methods
A descriptive study was conducted on patients diagnosed with breast cancer who came to Dr. Wahidin Sudirohusodo Hospital and Hasanuddin University Hospital, Makassar, Indonesia, from 2016 to 2019. The inclusion criteria were breast cancer patients aged over 20 years, with metastases detected by a radiological examination (chest X-ray, ultrasound, computerized tomography scan, or magnetic resonance imaging), who had undergone mastectomy or breast-conserving treatment (BCT). The exclusion criteria were patients with other cancers, those who had undergone mastectomy or BCT but where the molecular subtype was not clear, smokers, and patients with liver cirrhosis. Ethical approval was obtained from the local institutional review board (number: 063/UN464531/PP36/2022).
The medical record data taken as research data included age at diagnosis of breast cancer, clinical stage based on TNM, tumor location, metastasis and location, molecular subtype, histopathological grading, and mortality. The molecular subtype classifications used were luminal A, luminal B, HER2, and triple-negative [4–6]. The International Union Against Cancer recommends the staging classification based on the clinical stages of the TNM classification from the World Health Organization and AJCC, based on the size of the primary tumor (T), regional lymph nodes (N), and metastases (M) [11]. Classification based on metastases is cancer has spread beyond the place of origin, causing symptoms according to the location of the emergence of metastases.
The data were processed using Microsoft Excel 2010 (Microsoft, USA). Univariate analysis was carried out to determine the distribution of patient characteristics in percentages. The data processing results are presented in tables, graphs, and narratives.
Results
A total of 172 breast cancer patients were included in this study at Wahidin Sudirohusodo Hospital Makassar Sub-Division of Surgery Oncology. The characteristics of the participants can be seen in Table 1. The greatest proportion of cases were aged 50–59 years (31.4%), and the fewest were aged 80–89 years (1.7%). The highest clinical stage was stage 3b (45.9%), and the lowest was stage 2 (2.9%). Based on the degree of histopathology, the highest grade was moderate (72.7%), and the lowest grade was low (11.6%). The most common breast cancer subtype was luminal A (34.9%), and the least common was luminal B (15.7%). Most tumors were found in the right breast (57.6%), followed by the left breast (37.2%) and bilaterally (5.2%). The proportion without metastases was 62.8%, and the proportion with metastases was 37.2%. The most common site of metastases was bone (18.6%), followed by lung (14.0%) and liver (4.7%). The proportion of patients who lived was 49.4%, and 50.6% died.
Patient characteristics
Patient characteristics
The distribution of the rate and location of metastases by breast cancer molecular subtype is shown in Table 2 and Fig. 1. The rate of metastases was 30% in luminal A, 48% in luminal B, 40.4% in HER2, and 36.8% in triple-negative. The organ metastases diagram shows that the group with bone metastases included 10 cases of HER2 (31%) and nine cases of luminal A (28%). The most pulmonary metastases were found in cases of HER2 and luminal A (7 cases, 29%). The triple-negative group showed more liver metastases in three cases (38%).
Distribution of metastasis level and location by breast cancer molecular subtype
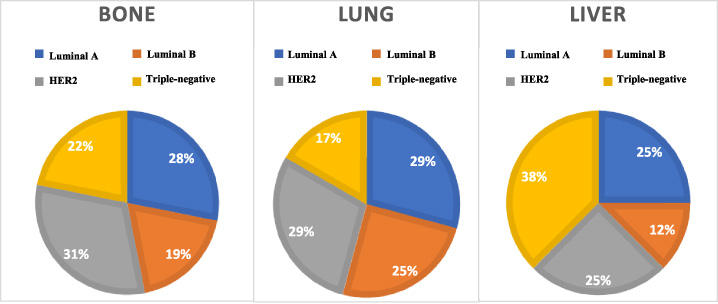
Distribution of metastasis locations by breast cancer molecular subtype.
The distribution of mortality rates by breast cancer subtype is shown in Table 3. In general, the mortality rate in this study was 21% (36/172 cases). The greatest proportion of deaths was in the triple-negative group (28.9%), followed by the luminal B and HER2 groups (25.9% and 21.2%, respectively).
Distribution of mortality rates by breast cancer molecular subtype
The majority of patients in this study were aged 50–59 years. This result follows GLOBOCAN 2018 data, where most breast cancer patients in Southeast Asia were aged in their 30s (38.1%) [2]. A study by Andriyanto et al. found that breast cancer patients were most commonly in the 35–49 year age group [14]. Our study found that most participants were at stages III and IV, which was similar to previous studies [14,15]. Sama et al. reported that approximately 90% of cases were in early stages [16]. Agarwal et al. [17] found that in developed countries, more cases were early-stage breast cancer, whereas, in developing countries, 50% of cases were locally advanced and metastatic. This may be because breast self-examination is better in developed countries than in developing countries.
Most histopathological grading in this study was intermediate. This result is in line with the research of Engstrom et al. [7], which showed that of 909 tumors, 12.9% were grade 1, 53.7% were grade 2, and 33.4% were grade 3. According to Lal et al. [18], low grades are often found in Western regions, whereas intermediate and high grades are the most common histopathological grades in Indonesia. The tumor location in this study was predominantly the right breast. This is in line with the study of Prihantono et al. [19], who showed that tumor location was most often unilateral (92%) rather than bilateral (8%). Perkins et al. [20] proposed that left-sided dominance reflects a detection bias. Given that most women are right-handed, it may be easier to detect a palpable lump in the breast.
The dominant molecular subtype in this study was luminal A, followed by HER2 and triple-negative. The luminal B subtype represented a minority in this study. This is similar to a study by Kennecke et al. [21]. They showed that the largest group among new cases of breast carcinoma was luminal A (43.9%). The study of Xiao et al. [22] of 312,035 new cases in the Asian region found that most groups were luminal A (68.1%), followed by triple-negative (10.6%), luminal B (9.53%), and HER2 (4.12%).
The location of metastases in this study was predominantly bone, followed by the lung and liver. Xiao et al. [22] also reported that the prevalence of metastases in breast cancer was 3.28% in bone, followed by 1.52% in the lung and 1.2% in the liver. In cases with HER2, the most common site of metastasis was the liver (OR 2.52), whereas, in triple-negative cases, the most common site was the brain (OR 1.85).
In this study, bone and lung metastases were common in the HER2 and luminal A subtype groups. This follows the study of Molnar et al. [23], where the HER2 subtype had a better metastatic prognosis than the hormonal type by 42%, and the luminal A subtype had a 23% lower risk of metastases. Metastases to the liver in this study were more common in the triple-negative subtype. This contrasts with research by Soni et al. [24], where the triple-negative group had more metastases in the brain by 31% and more liver metastases by only 15%. Xiao et al. [22] stated that the triple-negative group showed more metastatic spread to the brain (OR 1.85).
Bado et al. [25] stated that breast cancer metastasis has several interrelated processes: intravasation, circulation, extravasation, proliferation, and angiogenesis. In the hormonal subtype group of breast cancer, it is 72% easier for bone metastases to occur. This is caused by the activation of cyclooxygenase-2 (COX-2), which increases prostaglandins and further increases the expression of the aromatase enzyme. In addition, ERs and PRs are found in the bone stroma, supporting the formation of an osteogenic niche so that metastases in the hormonal subtype develop into macrometastases in the bone.
Chen et al. [26] found that the HER2 subtype showed more lung and liver metastases. HER2 is related to epidermal growth factor receptor, so angiogenesis increases, and the intravasation process in the primary tumor increases. However, metastasis in breast cancer is not a single process; various chemokines and other growth factors are also involved. Therefore, both hormonal and non-hormonal breast cancer can metastasize to more than one organ.
In this study, the proportion of death in each breast cancer subtype was highest in the triple-negative group (28.9%), followed by the luminal B and HER2 groups. Recent results show that the triple-negative molecular subtype and breast cancers expressing HER2 have higher mortality than the hormonal subtype. This is supported by the study of Chen et al. [26], who reported that the triple-negative and HER2 subtypes were associated with increased recurrence and mortality, with respective hazard ratios (HRs) of 2.05 (95% CI 1.31–3.20; P = 0.002) and 1.89 (95% CI 1.20–2.97, P = 0.006). This is also supported by the study of Kulkami et al. [27], who showed that in the Asian population, the triple-negative and HER2 groups had higher mortality, with HRs of 2.15 (1.95–2.36) and 1.31 (1.12–1.53), whereas the luminal A group had a lower mortality rate, with an HR of 0.59 (0.55–0.63) [27].
This study has several limitations. The number of samples for each molecular subtype group was not equal, which may have affected the study results and the possibility of bias. In addition, this study is descriptive, so it cannot analyze the prognostic value of these molecular subtypes more deeply. Nevertheless, this study succeeded in strengthening previous research showing that molecular subtypes can help determine breast cancer patients’ mortality and metastasis rates.
Conclusion
This study’s molecular subtypes of breast cancer showed similar metastasis and mortality distributions to previous studies. This IHC-based subtype determination is a potential predictive factor for metastasis and mortality in breast cancer. Further studies are needed to analyze this possibility.
Footnotes
Acknowledgements
The author would like to thank all staff in the Division of Oncology, Department of Surgery, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia, who helped conduct this study, and Muhammad Faruk MD, for his help in providing us with the linguistic assistance for this study.