
Abstract
Breast cancer is the most incidental and deadly neoplasm worldwide; in Mexico, very few epidemiologic reports have analyzed the pathological features and its impact on their clinical outcome. Here, we studied the relation between pathological features and the clinical presentation at diagnosis and their impact on the overall and progression-free survival of patients with breast cancer. For this purpose, we collected 199 clinical records of female patients, aged at least 18 years old (y/o), with breast cancer diagnosis confirmed by biopsy. We excluded patients with incomplete or conflicting clinical records. Afterward, we performed an analysis of overall and progression-free survival and associated risks. Our results showed an average age at diagnosis of 52 y/o (24–85), the most common features were: upper outer quadrant tumor (32%), invasive ductal carcinoma (76.8%), moderately differentiated (44.3%), early clinical stages (40.8%), asymptomatic patients (47.8%), luminal A subtype (47.8%). Median overall survival was not reached, but median progression-free survival was 32.2 months (29.75–34.64, CI 95%) associated risk were: clinical stage (p < 0.0001) symptomatic presentation (p = 0.009) and histologic grade (p = 0.02). Therefore, we concluded that symptom presence at diagnosis impacts progression-free survival, and palpable symptoms are related to an increased risk for mortality.
Introduction
Breast cancer (BC) is one of the most relevant public health problems. According to the Global Cancer Observatory (GLOBOCAN), there were 2 261 419 new cases and 684 996 deaths of BC worldwide in 2020. In Mexico, GLOBOCAN reported 29 929 new cases and 7 931 deaths in 2020 [1]. This information contrasts with the official data reported by the government of 12 102 new cases and 7 875 deaths in 2020 [2,3].
Screening strategies for breast cancer in our country, Mexico, specify the use of mammography as the primary detection method for women aged 40 or more [4–6], however, current clinical guidelines indicate that women should perform monthly self-clinical examinations starting at the age of 20 and with support of a clinician after the age of 25 during annual check-up to corroborate if the patient is performing the self-examinations properly. These clinical screening methods are controversial, because there is no evidence of their impact on mortality. Nonetheless, clinical studies are still trying to prove their efficacy through different populations [7–9].
Since reliable epidemiological information will improve public health, descriptive studies of signs and symptoms of breast cancer in the Mexican population have been conducted, either by public or private centers, in an attempt not for fixing the discordance, but for extend the knowledge of pathological characteristics of the BC patients [10–17]. Here, we studied the relation between pathological features present in a population treated in public centers, their baseline characteristics and their impact on the overall and progression-free survival of Mexican patients with breast cancer in Baja California Sur.
Methods
This study is a descriptive, longitudinal, observational, and retrospective analysis of patients registered in the database of “Registro de cáncer de Baja California Sur” from October 1, 2019, to April 26, 2021. Since this was a noninvasive study without direct contact with the patients, and all the information was acquired using an informed consent format for research an approval of an ethics committee was not needed.
Inclusion and exclusion criteria
We considered female patients aged 18 years or older with breast cancer diagnosis confirmed by biopsy, and available clinical records with informed consent for data usage in research. We excluded patients with incomplete or conflicting clinical records and non-primary breast tumors, Fig. 1. Since this work uses database information, unconventional variables rely on not-available information, whether of loss of the following patients or because of undifferentiated grade of classification, like unknown patients’ status, unspecified occupation and unclassifiable histopathology. At the same time, our inclusion criteria include a specific population of age and clinical conditions, and many records were discharged in the first step of eligibility, from 3, 302 to 356 clinical records. Exclusion criteria reduced even more our database to 199 clinical records, which can be a not so representative sample of the general population, therefore, we must take this into account as our principal limitations.
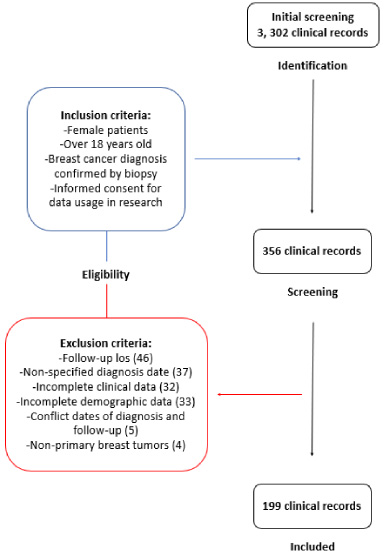
Record screening selection process.
Clinical and pathological characteristics of the population
The values for quantitative variables are represented with medians and the minimal and maximum values between brackets. Hormonal receptors [HR].
After the clinical record selection of 3, 302 clinical records, we extracted clinical and pathological information from 199 patients. Determination of clinical stage at diagnosis were based on clinical and radiologic criteria that categorized patients into early disease stages (I–IIA), locally advanced disease stages (IIB–IIIC), and metastatic disease (stage IV). On the other hand, according to the Allred score, we determined the hormone receptor (HR) status by immunohistochemistry (IHC) [18]. Following the classification made by Harvey (1999), an IHC scale greater than 2, corresponding to as few as 1% to 10% weakly positive cells was considered positive for estrogen (ER) and progesterone receptors (PR) [19]. Human epidermal growth factor receptor 2 (HER2) status was determined by IHC, and fluorescent in situ hybridization (FISH). Tumors were considered HER2-positive in cases reported as 3+ by IHC or amplified FISH. Luminal A and B classification was made using the method of Gennari (2021) where Luminal A is positive for HR and negative for HER2- (HR+, HER2-); Luminal B referees to a positive profile of HR and HER2 (HR+, HER2+); finally, HR-negative tumors that presented ER−, PR−, and HER2-, were classified as triple-negative (TNBC) [20]. Overall Survival and Progression-Free Survival were analyzed from the date of diagnosis until the last contact with the patient, median follow-up was 53 weeks, nine patients presented recurrence, but this was not considered for a cutoff-date.
Treatment information
Information of the patient’s treatment was obtained from the database of “Registro de cáncer de Baja California Sur” from October 1, 2019, to April 26, 2021. Their treatment was established following the indications of the ESMO Clinical Practice Guideline [22].
Statistical analysis
With the collected data, we constructed a database (Supplementary material S1) and performed statistical analysis in R studio (version 1.4.1106) using the ggplot2, survival, and survminer libraries. Overall and Progression-free survival were analyzed using the Kaplan–Meier method and associated risks through a Cox regression model.
Results
Asymptomatic middle-age females were the prevalent population
Clinical and pathological variables of the patients are shown in Table 1. We observed an average age of 52 years old (24–85) between the reported findings. The most common features were upper outer quadrant localization of the tumor (32%), the most common histological type was invasive ductal carcinoma (76.8%), primary invasive tumor (98%), moderately differentiated (44.3%), clinical-stage I (25.1%).
Most of our patients were asymptomatic (47.8%), but among symptomatic patients, the most common sign was a palpable mass (35.5%) followed by palpable adenopathies (21.2%); meanwhile, local hyperemia, nipple deformation and excoriation were the less present symptoms (0.5%, each one). The most common immunohistochemical pattern was Luminal A (47.8%). Likewise, most of our patients were treated with surgery (67.3%) and/or chemotherapy (42.36%), however, many patients did not receive any treatment (57.60%); finally, the treatments less required were radio- and targeted therapy (10.8% & 3%, respectively). Some patients received only palliative drugs (1.5%) or different treatments (0.86%).
Progression-free survival is related to pathological characteristics
Our population was made up of patients in their early adulthood (<40 years old, n = 26 patients), middle adulthood (40–65 years old, n = 146) and late adulthood (>65 years old, n = 31 patients). Overall and progression-free survival analysis were performed using the Kaplan–Meier method with 199 of our patients, median overall survival was not reached.
Our patient’s median progression-free survival was 32.2 months (29.75–34.64, CI 95%) (Fig. 2). Subgroups were stratified and analyzed according to previous variables. We found significant differences among the groups classified by symptomatic presentation (p = 0.009), clinical-stage (p ≤ 0.0001) and histologic grade (p = 0.02) (Fig. 2). The rest of the analysis, that was available to make taking into account the limitations that we had about the data of the patients, is available for consultation in Supplementary materials S2. Finally, all our variables were analyzed using univariate models. Statistically significant results were analyzed in a multivariate model. We appreciate that the clinical stage is a predictor for overall and progression-free survival (p = 0.036 and p ≤ 0.001, respectively).
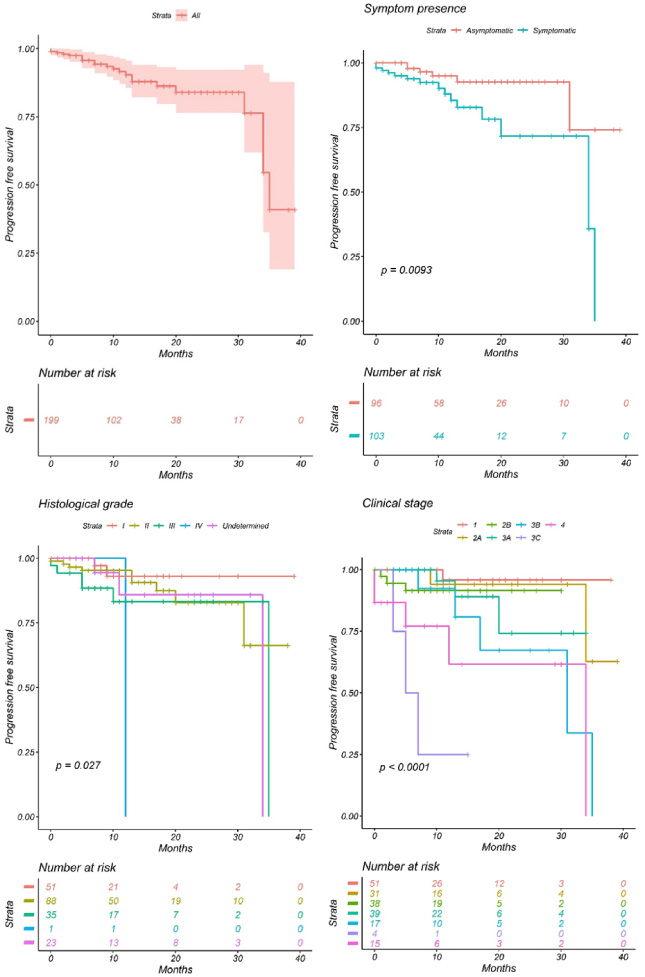
Progression-free survival analyses.
In this project, the impact on overall survival and progression-free survival of pathological variables in a Mexican population was analyzed. First of all, we must comment that the sample of 199 patients is not fully representative of the original data (356 records), but it is a first step in an attempt for increasing our population in the future, and works for the purposes of this project. At the same time, we specified that this population comes from a database of a public clinic, so this data is even more restricted to a specific population and it is not representative of the entire Mexican population. However, our population had an average age that matches previous reports in our country (50–60 years) [12–14]. Although breast cancer in young women is associated with more mortality and progression of the disease [23], we did not find a correlation in our population. This difference might be due to insufficient population size or not enough follow-up [12,14,24].
Previous studies in other countries established a worse prognosis for tumors in the central area of the breast (C500, C501) [22,24]. Even though our population shared the most frequent localization of the tumor, upper outer quadrant, with the population of these studies, we did not recruit a significant number of patients with this high-risk presentation (C504) [n = 1]; thus, we did not observe this relation. This study is the first one, to our knowledge, that evaluates the association between tumor localization and clinical outcomes in the Mexican population, contributing to some considerations for future studies.
Regarding the histological grade, we have a corresponding prevalence with previous national and international reports describing the histological subtypes, with the Luminal A pattern as the most prevalent [10,12,14]. Specific patterns have been associated with a worse prognosis [25–28]; however, we did not observe these associations.
In our study, the clinical stage was the most relevant predictor for overall and progression-free survival. We could appreciate that the locally advanced stages (IIB–IIIC) were more prevalent (49.1%) than early stages (I–IIA, 33.2%), followed by the advanced stages (IV, 7.4%). Finally, in-situ carcinomas were the least common (0.5%), confirming our country’s reported epidemiology [9]. Current American Joint Committee on Cancer (AJCC-TNM) recommendations contemplate the immunohistochemical profile for staging patients with breast cancer [29,30]. Since we did not observe any correlation between this profile and the prognosis of our patients, we decided to explore further variables involved in manual breast examination, such as tumor size and lymph nodes. First, we divided our population in two groups, patients with symptoms at the time of the diagnosis, and asymptomatic. Then, we stratified the symptomatic patients in two subgroups, patients with palpable symptoms, like breast tumors and palpable lymph nodes, and non-palpable symptoms (see Table 1) as described in previous studies [15]. Finally, we analyzed the outcome of each group and subgroup. We observed that symptomatic patients with palpable symptoms had a higher mortality risk (HR 1.61, (1.13–2.31) CI 95%, p = 0.009, Table 2), and asymptomatic patients had better clinical outcomes than the symptomatic group, regarding progression-free survival (p = 0.009, Fig. 2). We should consider that for palpable symptoms, both breast tumors and lymph nodes must have at least 2 cm of diameter to be palpable [31,32], which means it is more likely for patients with these symptoms to be in more advanced stages.
Cox regression for overall survival and progression-free survival
Cox regression for overall survival and progression-free survival
As mentioned previously, the recommended screening method for young women in our country is the clinical examination. However, it might only detect breast cancer in advanced stages; therefore, we should screen more patients with imaging studies, like mammography, to detect early stages with better prognosis, as we observed in our study with the better outcome present in the asymptomatic group.
The therapeutic approach of our patients was similar to that previously reported in our country [14]. Most of the patients had surgical treatment (84–97%), not conservative (83.2%), compared to previous data from Reynoso–Noverón (2017) in a public center, only 42.36% of our patients received chemotherapy, contrasting to 82.13% in their study; in addition, the chemotherapy in our patients was adjuvant (26.6%), meanwhile, in that study, it was used as neoadjuvant (51.9%); the use of radiotherapy and hormonal therapy was more common (65.3% and 67.1%, respectively), in our population only 18.22% received radiotherapy, and 19.21% received hormonal therapy. We also had six patients that received target therapy (2.95%) compared to none of the mentioned trials [14].
It is worth to say that our study had limitations, starting with its retrospective nature, which may lead to bias in selecting medical records [35]. The standardization of terms and variables was complicated, which caused many of them to be excluded; nonetheless, a representative sample could be obtained. Thus, our study helps to shrink the lack of information in overall and progression-free survival of patients with breast cancer in developing countries. Descriptive epidemiologic reports such as ours can improve the knowledge in our current landscape, and design strategies for the future of our patients. Despite the local authorities promoting early diagnosis by the self-clinical examination, these strategies seem insufficient, as the incidence and mortality continue to arise compared to developed countries. Campaigns focused on realizing mammographies to the recommended female population are needed to prevent diagnosis in advanced stages.
This study showed the relevance of mammography screening, which should be implemented especially in the countries with low availability of efficient treatments. Additional patients information, such as the clinical-stage showed as the most relevant predictor of prognosis in overall and progression-free survival. The presence of symptoms at the diagnosis impacted the progression-free survival, as the asymptomatic patients had better outcomes than those with symptoms. The presence of palpable symptoms had an increased risk for mortality. More studies with a larger sample of population that evaluate the clinical presentation and the manual breast examination as a predictor for the outcome in the Mexican population are needed to re-design more efficient screening strategies.
Footnotes
Acknowledgements
Registro de Cáncer de Baja California Sur.
6.
The author declares that they have no conflict of interest.
Author contributions
Conception: Gozalishvilli-Boncheva; Interpretation or analysis of data: Gozalishvilli-Boncheva; Gonzalez-Espinoza; Castro-Ponce; Preparation of the manuscript: Castro-Ponce; Bravo-Gutiérrez; Revision for important intellectual content: Montes-de-Oca-Moreda; Aguirre-Flores; Coyotl-Huexotl; Orozco- Luis; Chiquillo-Domínguez; Supervision: Garibay-Díaz; Aranda-Claussen; Ponce-de-León; Sánchez-Sosa; Sabaté-Fernández.