
Abstract
BACKGROUND:
The p53 mutation in breast cancer confers a worse prognosis and is usually associated with p53 overexpression (p53+) on immunohistochemistry. Previous studies have shown that p53+ tumors could be associated with low axillary tumor burden (ATB).
OBJECTIVE:
We aimed to evaluate the association between p53+ and ATB in a large series of breast cancers as an aid to personalizing axillary surgical treatment.
METHODS:
We retrieved 1762 infiltrating breast carcinomas from our database that were treated with upfront surgery in Hospital del Mar from 2004 to 2018. We compared p53+ and p53-negative (p53-) tumors in terms of the percentage of cases with high ATB and overall survival. This comparison was made overall and for each immunophenotype.
RESULTS:
Overall, 18.7% of breast tumors were p53+. High ATB was less common in p53+ tumors than in p53- tumors in the luminal B-Her2-negative immunophenotype (6.2% versus 16.9%, respectively, P = 0.025), but not in the other immunophenotypes or overall. Overall survival was worse in patients with p53+ breast cancer (P = 0.002).
CONCLUSION:
p53+ breast cancers were associated with worse overall survival. However, low ATB was more common in these tumors than in p53- tumors in the luminal B-Her2-negative subtype. Information on p53 expression could be of use to predict ATB in some breast cancer tumors.
Background
Breast cancer outcomes are related to well-known biological factors, such as tumor size, the presence of axillary lymph node invasion, metastasis, histological subtype, the number of foci [1], estrogen (ER) and progesterone receptor (PR) status, human epidermal receptor 2 (Her 2) status, and the Ki67 proliferation index [2].
The TP53 mutation is detected in 23% of breast tumors [3,4] and is usually associated with p53 overexpression (p53+) on immunohistochemistry. It is also related to breast cancer outcomes, as it confers a worse prognosis, including more frequent loco-regional recurrence [5–7].
The histological and molecular characteristics of the tumor are helpful for individualizing local breast cancer treatment [2,8]. Since the publication of the Z0011 trial in 2011 [9], there has been ongoing research to predict axillary tumor burden (ATB) with the aim of personalizing axillary surgery. Identified predictors of ATB include ultrasound features [10], a previous positive axillary biopsy [11], and the HER2+ subtype [12]. These predictors have been used in several predictive nomograms with variable accuracy [13].
p53+ has also been evaluated as a feature that could predict ATB, but the findings are discrepant. While some authors have found no relationship between p53+ and ATB [14,15], our previous studies revealed a significant association between these two biomarkers [16,17].
Given that the contradictory results found in previous studies could be due to the different features of the cohorts studied, the aim of this study was to evaluate p53 expression as a predictor of ATB in a large series of breast tumors for breast cancer as a whole and for each immunophenotype separately.
Materials and methods
Study type and ethics
We performed a retrospective cohort study of data prospectively entered into our Institutional Tumor Registry. The trial was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and was approved by the Clinical Research Ethics Committee of the IMIM, Spanish acronym for Instituto Municipal de Investigación Médica (Municipal Institute of Medical Research) id 2015/6282/I.
The study population comprised all women with a diagnosis of invasive breast carcinoma and upfront surgery treated in Hospital del Mar from January 1, 2004, to September 30, 2018.
Exclusion criteria comprised treatment in another center, in situ carcinoma, neoadjuvant treatments before surgery, and patients with insufficient information in the pathology report.
Pathology processing
Our standardized institutional protocol was followed to process breast surgery specimens. Briefly, all specimens were stained and sectioned at 3-mm intervals and then fixed in 10% neutral buffered formalin for a period ranging from 24–48 h. If possible, the entire specimen underwent paraffin processing. When not possible, the specimen was sampled using systematic mapping. Hematoxylin and eosin (H&E) slides were evaluated. Lesion extent, pathological type and histological grade were systematically reported. Sentinel lymph nodes were examined by serial sectioning: they were cut into 2-mm slices and, for each slice, six sections of 4-μm were obtained, leaving a 20-μm gap between them. Three alternate sections were stained with routine H&E and, if negative, the remaining sections were studied using cytokeratin. For axillary lymph node dissection (ALND), 3-mm slices were obtained for each node and, for each slice, a single 4-μm section was stained with routine H&E.
Immunohistochemical analysis was systematically performed including ER, PR, p53, Her2Neu, and Ki67. ER, PR and p53 were reported using a semi-quantitative scale, describing the percentage of positive cells and staining intensity. Ki67 was reported describing the percentage of positive cells. Her-2-Neu expression by immunohistochemistry was reported as negative (0,1+), positive (3+) or borderline (2+); in situ hybridization (ISH) was conducted in borderline cases to rule out Her-2-Neu gene amplification.
Association of p53 with other features and survival
We evaluated the association between p53 expression and tumor size, stage, number of foci, ATB, immunophenotype, and overall survival.
We divided ATB in two categories: low ATB, defined as ≤2 positive axillary nodes, and high ATB, defined as >2 positive axillary nodes. We chose this cut-off following the concept of low and high ATB used in the Z0011 trial [9,18] and the recommendations of international guidelines [19].
We defined five immunophenotypes following the recommendations of the 2013 St Gallen conference [2]: Luminal A-like (ER+, PR ≥20%, Her2-, ki67 <14%), luminal B-Her2- (ER+ and/or PR+ but PR <20%, and/or ki67 ≥ 14% and Her2-), luminal B-Her2+ (ER and/or PR+ and HER2+), Her2+-like (ER−, PR− and HER2+) and triple-negative-like (ER−, PR−, HER2-). Luminal B tumors were analyzed separately according to Her2 expression as their prognosis and management usually differ [20].
Variables evaluated as predictors of ATB
The variables analyzed as candidate predictors of ATB were p53 expression, histological subtype, histological grade, lympho-vascular invasion, Ki67, number of foci, tumor size, ER, PR, Her2 and immunophenotype.
Statistical analysis
We performed the statistical analysis using PAWS version 18.0. Continuous variables were compared using the Kruskall--Wallis or Spearmans Rho tests. We analyzed categorical variables with thechi-square and Fisher exact tests in the univariate analysis. Variables that were significant in the univariate analysis or significant in previously published research were entered into a multivariateanalysis, performed using multiple linear regression. Overall survival was analyzed using Kaplan-Meyer tests. Differences were considered significant if the p value was ≤0.05.
Results
Cohort description
During the study period, 2766 patients underwent surgery for primary breast cancer in Hospital del Mar. We excluded 699 patients treated with upfront systemic treatment and 342 patients because of missing pathological information on axillary nodes. The remaining 1725 patients underwent 1762 interventions (37 bilateral cases). The mean age was 61 years (range 23–92) and the mean tumor size was 18.91 mm (SD 14.55).
The median number of affected axillary nodes was 0.93 (range 0–30). Cases with a high ATB were less frequent in the luminal A subtype (19 of 362, 5.2%) compared to the Her2+ subtype (12 0f 79, 15.2%, P = 0.007). Other features of the study population are summarized in Table 1.
Main pathology features of the cohort
Main pathology features of the cohort
Overall, 329 of 1762 tumors (18.7%) were p53+. P53+ was more frequent in larger tumors (P = 0.001) and those in more advanced stages (P = 0.003). No differences were found between unifocal and multifocal/multicentric tumors (P = 0.669). These data are shown in Table 2.
Main pathology features in relation to p53 expression
Main pathology features in relation to p53 expression
Data on p53 expression and ATB are summarized in Table 3. High ATB was more frequent in p53- than in p53+ tumors (12.7% versus 4.5%, P = 0.025) in the luminal B Her2- subtype, but there were no significant differences in the remaining immunophenotypes or for the overall population.
p53 expression in cases of low and high ATB, overall and for each immunophenotype
In the luminal A subtype, there were 19 p53+ tumors (15.6%), 89 in the luminal B-Her2- subtype (15.6%), 41 in the luminal B Her2+ subtype (29.9%), 48 in the Her2+ subtype (60.8%), and 88 in the triple-negative subtype (49.7%).
We registered 198 deaths during the study period (11.98%). Overall survival was significantly higher in p53- than in p53+ patients (P = 0.0018), as shown in Fig. 1.
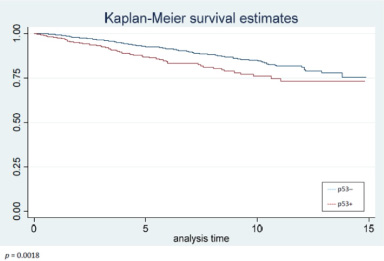
Differences in overall survival between patients with p53- and patients with p53+ breast tumors.
In the univariate analysis, variables associated with high ATB were lobular histological subtype, tumor size, lympho-vascular invasion, Ki67 > 14%, high histological grade, and multifocality/multicentricity, but not p53 expression (data shown in Table 4).
Pathology features and their relation with axillary tumor burden
Pathology features and their relation with axillary tumor burden
∗ATB, Axillary tumor burden. ∗∗ Non-specified type.
In the multivariate analysis, the factors that remained significantly associated with high ATB were lymphovascular invasion (P = 0.001), Ki67 > 14% (P = 0.04), and p53- (P = 0.029).
In this study, ATB was lower in p53+ than in p53- tumors in the luminal B Her2- subtype. Importantly, in the multivariate analysis using the whole cohort, p53- expression was a predictor of high ATB.
Personalizing surgical treatments, particularly in axillary surgery, is becoming of the utmost importance to minimize the number of unnecessary axillary dissections and their unwanted secondary effects. Therefore, a better understanding of the different factors that predict ATB could be of use to better select the optimal technique for the staging and treatment of the axilla. Currently, ongoing trials are being conducted on tailored axillary surgery [21] and on the avoidance of axillary staging in good prognosis tumors [22]. The results of this study indicate that both approaches would be much more precise if information on molecular factors, such as p53 expression, were to be included in those trials.
A surprising finding was that p53+ was not associated with low ATB in the univariate analysis including all the subtypes, and then showed an association in the multivariate analysis. An explanation is that this finding reflects a previously described statistical phenomenon called the Simpson paradox [23], in which a specific correlation between two outcomes can take an inverse direction when more parameters are combined.
When we analyzed the immunophenotypes separately, the fact that p53+ was predictive of low ATB only in the luminal B-Her2- subtype strongly suggests that nomograms predicting ATB should be built for each immunophenotype. This is also supported by previous findings [24].
The rates of p53+ tumors overall and for each immunophenotype reported in this study are concordant with those described in previously published articles [25]. This homogeneity between different research groups is reassuring as it suggests that evaluation of p53 expression with immunohistochemistry could be comparable between different centers.
The fact that p53+ was associated with low ATB in luminal tumors on the one hand, but with worse overall survival on the other, could be deemed contradictory. We hypothesize that p53+ tumors have a higher propensity for hematological but not for lymphatic dissemination, a feature already described for basal-like breast cancer [26].
A strength of this study is that, to our knowledge, it reports the largest case series with information on p53 expression. Another strength is the long follow-up. However, it also has some limitations. The first is that the number of patients in some subgroup analyses was insufficient. The second is that patient selection was biased to good prognosis immunophenotypes and stages, as we included only patients with upfront surgery. The reason for excluding patients receiving neoadjuvant treatment was that chemotherapy could alter both ATB and p53 expression, as observed by other authors [27]. Finally, another limitation is that we did not include any data on recurrences due to the limited information we retrieved on this subject.
Conclusion
In this study, p53+ was associated with low ATB in the luminal B-Her2- immunophenotype. In the era of personalized cancer treatments, this information could be used when individualizing axillary surgery. Further research is needed to determine whether the inclusion of information on p53 expression in ATB predictive nomograms is useful.
Footnotes
Acknowledgments
We thank Gail Craigie for her help in editing this manuscript.
We thank Sergi Mojal for his advice and support regarding the statistical analysis.
The authors would like to thank Josep M. Corominas, former pathologist in the Hospital del Mar, Barcelona, for his advice on the conduct of this study.
The study was funded by the Breast Diseases Unit of Hospital del Mar, Barcelona, Spain.
Conflict of interest
The authors declare that they have no conflicts of interest.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Author contributions
Conception: Pau Nicolau, Maria Vernet-Tomás.
Data interpretation or analysis: All authors.
Preparation of the manuscript: Pau Nicolau, Maria Vernet-Tomás.
Revision for important intellectual content: All authors.
Supervision: Maria Vernet-Tomás.