
Abstract
BACKGROUND:
The histological tumor grade influences the prognosis of breast cancer. In metastatic breast cancer, stromal cells produce chemokine (CXC motif) ligand 12 or stromal cell-derived factor-1 as a chemoattractant, which binds to chemokine (CXC motif) receptor 4 (CXCR4) expressed by breast cancer cells.
OBJECTIVE:
This study aimed to determine the expression of CXCR4 in invasive breast cancer in relation to lymphovascular invasion (LVI) and lymph node metastasis.
METHODS:
This observational study retrospectively investigated a paraffin block archived sample diagnosed with invasive breast cancer. The results of immunohistochemical staining with CXCR4 antibody and expression analysis were evaluated using light microscopy. The data were statistically analyzed using the chi-square test and presented in a table using SPSS version 18. P-values of <0.05 were considered statistically significant.
RESULTS:
The expression of CXCR4 was significantly associated with the incidence of LVI and lymph node metastasis in invasive breast cancer (both p = 0.001).
CONCLUSIONS:
The results show that the expression of CXCR4 varies and support its decisive role in the incidence of LVI and lymph node metastasis in invasive breast cancer.
Introduction
Breast cancer (BC) is one of the most common malignancies in women worldwide. According to the Global Cancer Observatory 2020, there are 2,261,419 (11.7%) new cases detected, with 684,999 (6.9%) new deaths annually [1]. The Jakarta Cancer Registry shows that BC has the highest incidence among all types of cancer in Indonesia, with a prevalence of 18.6 cases per 100,000 yearly [2,3]. Invasive BC of no special type refers to a group of breast cancers that cannot be classified morphologically into a specific histological type [4].
Metastasis or spread of tumor cells can occur either lymphogenously or hematogenously. BC generally metastasizes lymphogenously, and histopathological examination is the gold standard procedure for detecting metastases to regional lymph nodes [5]. The prognosis of BC is influenced by several factors, including histological tumor grade, vascular invasion, and lymph node metastasis [6–8].
Chemokine (CXC motif) receptor 4 (CXCR4) is a member of the CXC chemokine receptor group [9,10]. The only ligand of CXCR4 is chemokine (CXC motif) ligand 12 (CXCL12), also known as stromal cell-derived factor-1 [11]. The binding between CXCR4 and CXCL12 activates various intracellular signal transductions that can affect the ability of tumor cells to invade and metastasize [7,12,13]. CXCL12 also regulates cell survival through two mechanisms: increased transcription of cell survival-related genes and post-translational inactivation of the cell death machinery [7,12]. CXCR4 activation through the G𝛽𝛾 subunit also induces the expression of the Ras protein, activating RAF. Furthermore, it activates extracellular signal-regulated kinase, increasing the proliferation and migration abilities of tumor cells [7,12,13].
This study aimed to determine the relationship of CXCR4 expression with lymphovascular invasion (LVI) and regional lymph node metastasis by comparing CXCR4 expression scores between grades 1, 2, and 3 invasive BC.
Methods
This cross-sectional study aimed to assess the expression of CXCR4 in invasive BC. It was conducted at the Anatomical Pathology Laboratory, Hasanuddin University Hospital, Makassar, Indonesia from June to November 2021.
The study population was paraffin block archived samples from mastectomy resection tissues sent to the Dr. Wahidin Sudirohusodo Hospital, Sentra Diagnostik Patologia Makassar, and Anatomical Pathology Laboratory at Hasanuddin University Hospital, Makassar, Indonesia diagnosed with BC based on hematoxylin and eosin (HE) staining results. Ethical approval for this study was obtained from the Research Ethics Committee of the Faculty of Medicine, University of Hasanuddin, Makassar, Indonesia (no. 0619/UN4.6.4.5.31/PP36/2021).
The sample included the entire population that met the inclusion criteria. Consecutive sampling was performed, and using the Lemeshow formula, we found that the minimum required sample size was 58. The inclusion criteria were as follows: (a) breast tumor diagnosed by a pathologist as grades 1, 2, and 3 invasive BC; (b) block paraffin from grades 1, 2, and 3 invasive BC tissue processed in accordance with the standard protocols for CXCR4 immunohistochemistry examination; and (c) CXCR4 immunohistochemical results interpreted by a researcher and two anatomical pathologists. Meanwhile, the exclusion criterion was paraffin block preparation of invasive BC tissue damaged during CXCR4 immunohistochemical examination.
HE staining
After the tissue blocks were collected, the tissue was cooled in the refrigerator and then cut using a 4 μm microtome. The tissue was then put into a water bath at approximately 60 °C. The pieces in the water bath were taken using a polysilane object glass, drained to dry, placed on a slide warmer at approximately 60 °C for 15 min, and then stained with HE solution from Merck (Darmstadt, Germany; catalog no. 115938 and 115935) in accordance with the standard protocol.
Immunohistochemical staining
The tissue in the paraffin blocks was cut to a size of 4 m, glued onto a poly-L-lysine slide, and then deparaffinized. Each section was examined using the peroxidase–conjugated avidin–biotin complex (ABC) method, while immunohistochemical staining was performed using the standard ABC method. The unstained slides were incubated with peroxidase-1 for 5 min at 25 °C, followed by the standard ABC procedure. Immunohistochemical staining was conducted using concentrated CXCR4 polyclonal antibody with 1:50 dilution (rabbit anti-CXCR4 polyclonal antibody, catalog no. BZ-0813320F-AP; Bioenzy, Shanghai China,) in accordance with the manufacturer’s instructions. Two senior anatomical pathologists evaluated the immunohistochemical staining results using a light microscope.
Immunohistochemical result interpretation
The expression of CXCR4 is generally evaluated on the basis of the accumulation of proteins in the membrane, cytoplasm, and nucleus of cells detected using immunohistochemical methods. If the expression is positive, it will appear brown at the location of the antigen. Herein, the Olympus CX-43 light microscope (Tokyo, Japan) was used. The expression scores were calculated using a scoring system based on the intensity of the color and proportion of the stained cells. Visually, the expression locations were observed in the tumor cell membrane, cytoplasm, and nucleus (Fig. 1).
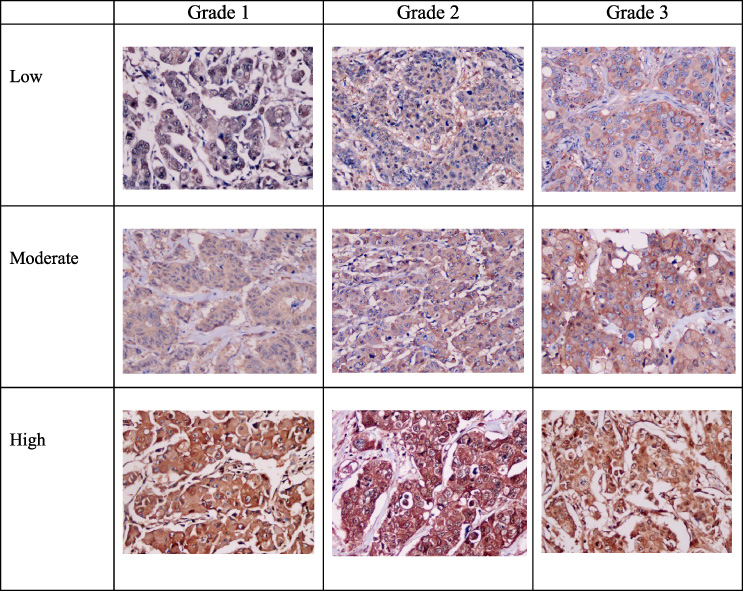
Expression of CXCR4 in invasive breast cancer. Expression of CXCR4 in the membrane, cytoplasm, and nucleus of tumor cells (magnification ×40). (Abbreviation: chemokine (CXC motif) receptor 4).
Invasive BC generally has a mammary epithelial origin based on immunohistochemistry findings or appearance. Herein, BC lacking the histological features to be morphologically classified as a particular subtype of BC was excluded [14]. Histological investigation was performed on the basis of the HE staining results, and diagnosis was made on the basis of the light microscopy results.
Grading
HE staining was used to generate the semi-quantitative grade of cancer based on the appearance of the cells under the microscope, including the tubular shape, nuclear pleomorphism, and number of mitoses [15].
CXCR4 expression score
The CXCR4 expression score (0–12) was obtained by multiplying the fraction of the tumor area that stained positively (0–4) by the intensity of CXCR4 staining (0–3) [7].
Determination of the histopathological grade
The histological grade of BC was evaluated using the Elston and Ellis modification of the Scarff–Bloom–Richardson grading method [6,16,17].
Immunoexpression of CXCR4
The immunoexpression of CXCR4 was assessed on the basis of a semi-quantitative estimate obtained using a scoring system assessing the intensity and proportion of the stained area [18,19].
Immunoreactive score
The immunoreactive score was obtained by dividing the intensity by the proportion of the stained region. The score can range from 0 to 12. A score higher than 5 indicates a high CXCR4 expression, while a score lower than 5 indicates a low CXCR4 expression [18,20].
Statistical analysis
Data were statistically analyzed using the chi-square test and presented in tables using SPSS version 18 (IBM Corp., Armonk, NY, USA). The statistical data were considered significant when the p-value was <0.05.
Results
The average age of the patients with invasive BC was 51 years (standard deviation, 10.98 years). Fifty-five patients (55.0%) were aged over 50 years. The distribution of the samples based on the histopathological diagnosis showed that the most common grade of invasive BC was grade 2 (n = 40; 40.0%), followed by grade 3 (n = 35; 35.0%) and grade 1 (n = 25; 25.0%) (Table 1). The CXCR4 expression was evaluated, revealing that the majority was strongly expressed (n = 77; 77.0%).
Characteristics of patients with invasive breast cancer
Characteristics of patients with invasive breast cancer
LVI, lymphovascular invasion; CXCR4, chemokine (CXC motif) receptor 4.
Table 2 shows that among the 100 cases of invasive BC, 65 had positive LVI, and 35 had negative LVI. Seventy-seven cases had a high CXCR4 expression, including 63 (50.1%) with positive LVI and 14 (27.0%) with negative LVI. Meanwhile, 23 cases had a low CXCR4 expression, of which 2 (15.0%) had positive LVI, and 21 (8.1%) had with negative LVI. We found a significant difference between CXCR4 expression and LVI (p < 0.001).
Table 2 Difference between CXCR4 expression and LVI
∗chi-square test; LVI, lymphovascular invasion; CXCR4, chemokine (CXC motif) receptor 4.
Table 3 shows that among the 100 cases of invasive BC, 72 had lymph node metastases, and 28 had no lymph node metastases. Of the 77 cases with a high CXCR4 expression, 67 (55.4%) had lymph node metastases (positive lymph nodes), while 10 (21.6%) had no lymph node metastases (negative lymph nodes). Meanwhile, of the 23 cases with a low CXCR4 expression, 5 (16.6%) had lymph node metastases, while 18 (6.4%) had no lymph node metastases. The CXCR4 expression was found to be significantly associated with positive and negative lymph nodes (p < 0.001).
Difference between CXCR4 expression and lymph node metastasis
∗chi-square test; CXCR4, chemokine (CXC motif) receptor 4.
BC is the most common malignant tumor affecting women worldwide. It remains the leading cause of high mortality rates in female malignancies, although the mortality rates appear to be significantly reduced with early detection. Most mortality in patients with malignancies is attributed to tumor cell metastasis to other organs. Tumor metastasis can occur either lymphogenously (lymphatic drainage) or hematogenously. For malignancies of epithelial origin (carcinoma), most tumor cells spread via the lymphatic system [5].
A new marker with a strong predictive value that could be independently obtained is needed to determine the disease prognosis. CXCR4 is a transmembrane protein belonging to the paired G protein receptor group, which binds to a specific ligand, namely CXCL12. The binding between CXCR4 and CXCL12 activates various intracellular signal transductions that can affect the invasiveness and metastasis of tumor cells [21–23].
In this study, the majority of the patients with invasive BC were aged over 50 years, which indicates a higher risk for invasive BC in older populations. This result is in line with that reported by Kumar and Abbas [24] that 75% of invasive BC cases are found at the age of more than 50 years and 5% at the age of 40 years. The increased risk for BC in old age is associated with reproductive factors, such as late menopause, early menarche, nulliparity, late age of the first pregnancy, and postmenopausal hormone replacement therapy [6].
Several studies have evaluated the expression of CXCR4 in tumor cells and its association with clinicopathological parameters and cure rates in various types of cancer. Cabioglu et al. [25] and Yasuoka et al. [26] showed that the expression of CXCR4 in the cytoplasm of tumor cells was significantly related to the incidence of axillary lymph node metastasis in BC. In contrast, the expression of CXCR4 in the nucleus of tumor cells was not significantly associated with the incidence of lymph node metastases. Furthermore, Salvucci et al. [27] showed that tumor cells with CXCR4 expression in the nucleus were associated with a higher grade, more advanced stage, and lower survival rate. The mechanism underlying CXCR4 expression in the nucleus of tumor cells remains unclear, necessitating further research in this area. The binding of CXCR4 with CXCL12 could induce translocation of CXCR4 into the cytoplasm and nucleus of cells. Translocation of CXCR4 into the cell nucleus can activate transcription factors in the nucleus [28]. Another study suggested that endosomes facilitate the translocation of CXCR4 through clathrin-coated pits and requires the Hsc73 molecule [29].
In this study, we assessed the expression of CXCR4 and found that it was associated with invasion and metastasis. Specifically, CXCR4 expression was found to be significantly related to LVI and lymph node metastasis. We also analyzed the sensitivity and specificity of CXCR4 expression in predicting the incidence of lymph node metastases in invasive BC and obtained the following values: 93.1% and 64.3%, respectively. Dayer et al. [30] examined the expression of CXCR4 using the quantitative real-time polymerase chain reaction method in tumor tissues from patients with invasive BC; they found that CXCR4 expression was higher in those with lymph node metastases than in those without. Cabioglu et al. [25] used immunohistochemical methods to evaluate BC tissues and found that BC tumor cells with lymph node metastases express CXCR4 more strongly than do those without lymph node metastases. They also examined the sensitivity and specificity of CXCR4 expression in predicting lymph node metastases and obtained values of 11% and 95%, respectively.
LVI is a crucial step in the complex process of tumor metastasis and is an important criterion in determining therapy. Thus, it is considered one of the significant prognostic factors of invasive BC with local and distant recurrence [31]. In cases that have already metastasized, the life expectancy is only about 2–3 years. One of the important steps in detecting the presence of metastases and staging in BC is to detect the presence of metastatic tumor nests in regional lymph nodes. Regional lymph nodes are the primary lymphatic drainage route from all areas of the breast, and the presence of lymph involvement is a strong predictive factor for recurrence and survival [5].
Another study found that primary tumors secrete vascular endothelial growth factor (VEGF)-C, VEGF-D, and other growth factors, which bind to VEGF-3 receptors on the endothelial cells of lymphatic vessels. This binding triggers the proliferation and formation of lymphatic capillaries that lead to the formation of lymphatic vessels. Lymphangiogenesis is associated with an increased incidence of metastasis to regional lymph nodes [5,32–34].
CXCR4 can increase the incidence of tumor cell metastasis through angiogenesis. The binding between CXCR4 and CXCL12 increases the activation of endothelial progenitor cells to come to the environment around tumor cells and form new blood vessels. CXCR4 is associated with the expression of VEGF and platelet-derived growth factor-D, which is related to the formation and stabilization of new blood vessels around the tumor. The formation of new blood vessels around cancer tumors increases the incidence of metastasis from tumor cells. CXCR4 can also affect the immune system around tumor cells. It can attract dendritic cells to come into the environment around the tumor. Meanwhile, dendritic cells can suppress antitumor immunity by inactivating cytotoxic T lymphocytes [35].
A limitation of the study was the use of a single marker—cancer stem cells (CSCs)—with only one immunohistochemical modality. This causes the expression analysis to be less accurate. Consequently, we were unable to analyze the complexity and relationship between the CSC marker CXCR4 and other molecules involved in the invasion and metastasis of invasive BC.
Conclusion
CXCR4 expression is significantly associated with LVI and lymph node metastasis. Further research is needed to identify the link between CXCR4 expression in invasive BC and hormonal status (luminal type).
Footnotes
Acknowledgements
The authors would like to thank Muhammad Faruk, MD, for his contributions in editing this manuscript, and express their gratitude to all individuals who participated in this study.