
Abstract
Lymph node microcalcifications are rare events, and when they are accompanied by neoplasia, they usually seem to be associated with a metastatic condition. We present a case of a patient with breast cancer and lymph node microcalcifications undergoing neoadjuvant chemotherapy (NCT). A change in the calcification pattern towards becoming coarse was observed. Calcification represented a marker of axillary disease, and it was resected after NCT. This is the first report of a patient with lymph node microcalcification undergoing NCT. We observed a change in the calcification format, which facilitated lymph node sentinel identification. Pathological evaluation indicated metastatic disease.
Introduction
Mammography is the main imaging method associated with decreased mortality due to breast cancer [1]. To standardize mammography findings, the BI-RADS classification is used to determine the probability of predicting breast cancer. Some rare events, such as axillary lymph node microcalcifications, have not been widely studied.
For locally advanced breast cancer (LABC), neoadjuvant chemotherapy (NCT) allows the increased of breast [2] and axillary preservation, making it essential to analyse axillary radiologic findings [3,4], although there is limited radiological and pathological correlation [5,6]. By evaluating the pathologic response after NCT in the breast, we can observe the absence of disease, the presence of ductal carcinoma in situ (DCIS), a concentric reduction or a fragmentation, which are associated with distinct radiological alterations. Sentinel lymph node (SLN) evaluation must be considered after NCT, but for axilla evaluation, the criteria for suspicion were created based on upfront evaluation, such as lymph node shape, cortical thickening, smooth margins or hilum alteration [7], with no standard evaluation. In patients undergoing NCT, the BI-RADS system presents the results in a generic way (BI-RADS 6), and imaging exams are used to guide clinical decisions by predicting the pathological response. Breast magnetic resonance imaging (MRI) is the exam that is closest to pathological response to NCT in the breast [8], and ultrasound helps us to evaluate the axillary response.
The presence of axillary lymph node microcalcifications associated with breast cancer is extremely rare [8–13] – only one such case has been reported after NCT [14]. However, no case of lymph node microcalcifications observed before or after NCT has been reported, making this report of particular interest.
Case report
A 42-year-old woman reported a 7-month history of areolar nodulation, retraction and breast hardening. Physical examination revealed a 5 × 4 cm retroareolar tumour in the left breast with central skin peau d’orange appearance (5 × 5 cm) and a suspicious lymph node measuring approximately 2 cm in the axilla, clinical stage T4bN1M0. The patient underwent biopsy, and an invasive ductal carcinoma, histological grade 2, luminal A was observed.
In the mammogram, architectural distortion in the medial lower quadrant, retroareolar retraction in the left breast, and the absence of microcalcification in the breast were observed, despite its presence in the axillary lymph node (Fig. 1a). Ultrasonography revealed an irregular nodule with spiculate margins located in the central and medial lower quadrants of the left breast (4.2 × 2.4 × 2.6 cm), and round lymph nodes in level I axillary, thickened cortex and echogenic foci were observed (Fig. 1b). Pretreatment evaluation (abdominal and thoracic tomography associated with bone scintigraphy) showed no systemic disease. If surgery was indicated, the patient was considered a candidate for mastectomy with axillary lymphadenectomy. Because clinical stage, NCT was indicated, and lymph node microcalcification was considered a marker for lymph node evaluation after NCT.
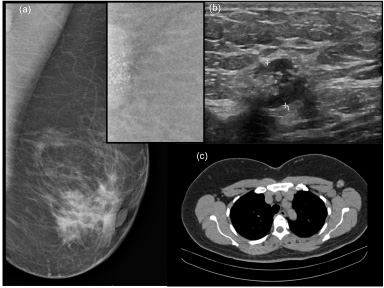
Prechemotherapy lymph node microcalcifications in the axilla. (a) Mammography; (b) Ultrasonography; (c) Thoracic tomography.
The patient underwent NCT with the 4AC (adriamycin and cyclophosphamide), followed by a 12 T (Paclitaxel/Taxol®) regimen. After NCT, she underwent new breast staging tests. Clinically, the disappearance of breast oedema, a hardened retroareolar area (4 × 4 cm) and axillary fibrosis were observed. On mammography, architectural distortion disappeared, and lymph nodes with microcalcifications showed heterogeneous gross calcifications (Fig. 2a). On US, there was a dimensional reduction in the irregular nodule, measuring 2.8 × 1.4 × 2.3 cm, and unsuspected lymph node metastasis, despite the presence of lymph node calcification (Fig. 2b). Breast magnetic resonance imaging (MRI) showed architectural distortion and heterogeneous retroareolar enhancement, indicating a partial pathologic response (Fig. 2c). In the preoperative imaging evaluation, lymph node calcification was observed in all exams (Fig. 2a, b, c).
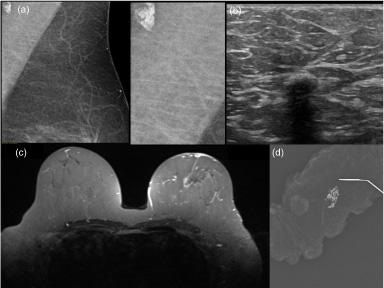
Calcifications in the axilla after NCT. (a) Mammography, with enlargement calcification. (b) Breast ultrasound. (c) Breast magnetic resonance imaging. (d) Surgical specimen mammography.
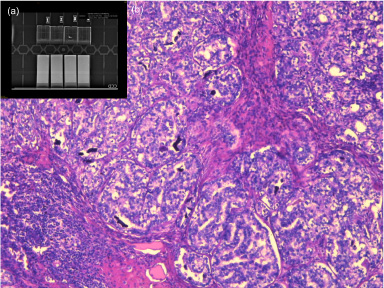
Lymph node with calcification. (a) Radiological control and block selection; (B) Pathological anatomy. HE 100xx. Invasive ductal carcinoma metastasis associated with microcalcifications (black areas).
She underwent central quadrantectomy combined with plug-flap and SLN examination, with resection of the labelled lymph node (Fig. 2d). Intraoperative frozen section evaluation revealed the presence of axillary metastatic tissue, and an axillary lymphadenectomy was performed. The anatomopathological examination showed residual invasive ductal carcinoma (0.3 cm) associated with DCIS, in addition to the presence of lymph node metastases (6/15 lymph nodes) with coarse calcifications in between. Imaging review of the material selected the lamina (Fig. 3a), which showed that the lymph node containing calcifications had metastatic disease (Fig. 3b). She received radiotherapy in the residual breast, supraclavicular fossa and local boost. Eight months after surgery, she was undergoing hormone therapy with tamoxifen, and she was disease free. It is planned tamoxifen for the first five years, followed by anastrozole up to the tenth year. Clinical evaluation is planned every six months for the first five years and then an annual. Radiological breast evaluations were planned to be performed once a year in the absence of symptoms or signs.
When evaluating patients who have undergone NCT for breast evaluation, we usually examine indirect signs such as tumour size, concentric tumour shrinkage, presence of calcifications and lymph node aspects, although limited radiological and pathological correlation related tumour characteristics and tumour size [5,6]. MRI [5] is the best exam for breast evaluation. When we analysed the axilla, axillary ultrasound [15] was superior to the combination of MRI and 18F-fluoro-2-deoxy-glucose positron emission tomography (PET-CT). In our clinical practice, MRI is used for the assessment of tumour size and location, but preoperative surgical planning are frequently performed based on triple ratings (clinical, mammography and ultrasound aspects). In the past, we considered the initial tumour size [16], but now we are descaling the surgery [17]. When we have concentric tumour shrinkage, it is easy, but it is important to consider the potential presence of microcalcifications. The presence of microcalcifications in the breast after NCT is not a condition for the presence of residual disease [18], but they must be removed. The presence of microcalcifications in the axilla after NCT is a rare event, and more reports are necessary to evaluate this condition.
In our breast cancer division, nonmetastatic LABC is routinely evaluated with a triple rating (clinical examination, mammography and breast ultrasound) before and after chemotherapy, with the aim of improving breast and axillary conservation. In special cases, MRI is performed. All surgeons perform oncoplastic breast surgery and have radiology skills, a fact that allows better planning for surgery. For nonpalpable lesions, the surgeons perform preoperative marking of radiologic alterations. Surgeries are indicated based on triple rating findings, and we have intraoperative pathologic evaluation. SLN evaluation is based on quadruple rating [palpation, blue dye in combination radioisotope (technetium-99 m) and frozen section]. When evaluating patients who have undergone NCT, we tried to find a minimum sampling of three lymph nodes, and when we did not find an SLN, the sentinel lymph nodes were positive during frozen section, or after paraffin evaluation, the patients underwent axillary lymphadenectomy.
Preoperative lymph node assessment via fine-needle aspiration cytology (FNAC) or core biopsy prior to chemotherapy can be performed to elucidate the axillary status before NCT; when the evaluation is associated with clips, a decrease in false-negative SLN evaluation is observed [19], and the association between false-negatives and FNAC is high [20]. However, clips are not found in all cases [15]. Axillary evaluation and axillary clips represent an ideal condition, but they add time to patient assessment because patients will undergo two radiology assessments (diagnosis of breast cancer and evaluation of axillary status), thus impacting patient navigation. This condition is important to be considered in developing countries, due to public limitations networks, high demand of patients and logistical limitations, leading to increase the time for first treatment.
There has been an increase of the use of the SLN evaluation after NCT in the United States, despite reports of false-negative SLN [21]. We selected patients based on triple evaluation before surgery and quadruple evaluation during surgery. Although there is a relationship between the breast and axillary responses, this relationship is not linear. In the current era of personalized medicine, we evaluate patient responses separately due to the loss of quality of life associated with mastectomy or limb lymphedema. To increase safety in patient selection, we selected patients based on a triple rating, and we performed the SLN evaluation based on a quadruple rating. During the follow-up period, if clinical or radiological alterations are observed, the patient is examined, and if necessary, lymphadenectomy is performed.
Microcalcifications in the breast are associated with breast cancer in up to 30% of cases, and the cluster of heterogeneous and pleomorphic microcalcifications found in the mammographic study is representative of in situ cancer in up to 90% of cases [22]. Calcification in the axillary lymph nodes is an uncommon mammographic finding and may present in multiple forms, namely, pleomorphic, amorphic or gross. There is no need for mammary microcalcification [12], as in the present case. Lymph node microcalcifications are rare and usually described in case reports; thus, the incidence rate of these events remains unclear. A single study observed 2 cases in a series of 96 patients [8]. Based on their aetiology, they were described as secondary to toxoplasmosis [9], tuberculosis, sarcoidosis [23,24], or metastatic disease from ovarian [25], thyroid [23], or peritoneal cancer [26]. They have also been described to be association with known primary breast cancer [8,9,11,13,14] or unknown breast cancer [12].
When evaluating the format of calcifications in lymph nodes, microcalcifications can be secondary to a foreign body (microcalcification-like), secondary to gold injection in rheumatoid arthritis [11] or associated with the presence of a tattoo [27–30]. When microcalcifications are associated with breast cancer, they are usually diffuse, morphologically presenting as heterogeneously grouped [8,12,13], amorphic/indistinct [9,11,14] or pleomorphic [11].
NCT can alter the appearance of microcalcifications in the breast, and there may be a decrease, increase or maintenance of the findings. Lymph node microcalcification in axilla has been observed after treatment in only one case of mammary carcinoma, and metastatic lymph node disease was observed in that case [14]. To the best of our knowledge, no study has reported a patient undergoing NCT who had previous axillary lymph node microcalcifications, which makes the findings of this study of particular interest. In the present case, a radiological change was observed, with gross calcification that grouped after NCT. In the literature, associated with SLN evaluation and NCT, there is a discussion about the identification and placement of metal clips in the compromised lymph node prior to NCT [19,31]. The presence of calcifications, mainly after NCT seems to be a potential marker of axillary disease, as no previously report, justifying this publication.
In patients with neoplasia, the presence of lymph node microcalcifications is associated with the presence of axillary metastatic disease [12,13,23,25,26], which occurs in 50.7% of thyroid cancer cases [32]. This association is rarely evaluated in breast cancer, although all reported cases had metastatic lymph node disease [8,12–14]. In the case reported herein, there was also a change in the radiological pattern (punctate to grouped punctate), and it was associated with the maintenance of axillary metastatic disease, indicating the need to remove it and a potential marker for the identification of lymph node disease and residual disease.
The presence of axillary calcification is a rare event. Histological evaluation is necessary for the differential diagnosis and better understanding of this condition. The resection should be guided by radiology. It is necessary to better describe the radiologic characteristics to avoid false-positive resection or unnecessary axillary lymphadenectomy. More reports are necessary for a better understanding of this rare situation.
Conclusion
Microcalcifications in the breast after NCT are not always associated with residual disease, but pathological evaluation of the whole area is necessary. Lymph node microcalcifications associated with cancer are a rare event and are possibly associated with axillary metastasis and they are a marker for lymph node evaluation after NCT.
Footnotes
Conflict of interest
We declare no conflict of interest.